
Abstract
BACKGROUND:
Treatment of distal intra-articular humerus fractures is still a technical challenge. Until now, little is known about the regain of strength and elbow agility after surgical treatment of these fractures. Due to small collectives there is only limited data.
OBJECTIVE:
Investigation of regained strength and elbow agility in patients with intra-articular distal humerus fractures.
METHODS:
A total of 28 patients were treated with distal intra-articular humerus fractures followed up for an average period of 62.3 months. The following parameters were examined: Arthrosis, heterotopic ossification, functional outcome (MEPS, DASH score, LES) and isometric strength of the elbow in extension and flexion was tested in 30
RESULTS
: There was a high complication rate with 32%. At the 60th month post injury, range of motion (ROM) of the elbow was 114
CONCLUSIONS:
Functional impairment in terms of reduced ROM and muscle force is a common complication after distal intra-articular humerus fracture. Patients over 60 years have a higher deficit of motion in the injured elbow joint and an inferior clinical outcome. Superiority of modern angle-stable implants could yet not be shown.
Keywords
Background
Fractures of the distal humerus are rare with 2–3% of all fractures. Approximately 60% of these fractures are intra-articular [1, 2]. Due to the constant aging of the population, the rate of osteoporotic fractures will continue to increase [3, 4]. The goal of surgical treatment should be a free range of motion and a painless function of the joint. The gold standard in the treatment of unstable fractures remains to be surgical with better results than in conservative therapy [2, 5]. Surgical therapy is still a technical challenge, although new innovative anatomical and multidirectional locking plates promise great potential. Nevertheless, the risk of complications remains high. The main complications expected postoperatively are a decrease of the range of motion (ROM), ulnar nerve damage, non-union and heterotopic ossification [3, 4, 6, 7, 8, 9]. Due to the low incidence of this kind of injury, there is very little information in this regard found in the current literature. The overwhelming proportion of patients has a loss of function in the sense of a significantly reduced muscular strength, which is hardly considered in the literature [7, 9, 10].
Therefore, the goal of this study was to investigate the rate of complications, functional impairments in regard to the elbow agility in terms of a reduction of the ROM and the reduction of muscle force following surgical treatment of distal intra-articular humerus fractures.
Methods
The study was conducted in compliance with the current laws applying in Germany and follows the Declaration of Helsinki for ethical principles for medical research involving humans. The study was approved by the local ethics committee (250/11). Patients’ verbal and written consent to participate in this study was taken.
The retrospective study only included patients with a unilateral distal intra-articular fracture as a mono injury of the upper extremity which subsequently underwent surgery. Twenty-eight patients of a total of 32 patients (87.5%) were examined. Medical charts were analyzed with regards to specific parameters including age, gender, fracture mechanism, fracture type according to the AO classification [11], operative procedure and complications during the treatment during the hospital stay. At the clinical follow-up the function of the joint was examined and the radiographic findings during the treatment were analyzed for postoperative results. The onset of arthrosis was rated according to the classification of Kellgren and Lawrence [12] and heterotopic ossifications according to Brooker [13]. The subjective functional outcome was evaluated by the Mayo Elbow Performance Score (MEPS) [1], Disabilities of the Arm, Shoulder and Hand Score (DASH) [14] and the Liverpool Elbow Score (LES) [15]. To evaluate the quality of life (QoL) the SF-36 questionnaire was used [16].
ROM of the elbow joint was measured clinically. The isometric strength of flexion and extension was quantified in 30
Statistical analysis was carried out using IBM SPSS Statistics (version 20; IBM Deutschland Ltd., Ehningen, Germany). All scale variables were tested for normality with the Shapiro-Wilk test. If normal distribution was given the Student’s
Results
Gender distribution was equal (14 female and 14 male patients). There was a bi-headed curve for the age of the patients at the time of injury with one peak at 25 years and another peak at 65 years (Fig. 1). The average age at the time of injury was 52.6 years (range 20–82 years). Patients were followed up at 62.3 months (range 24–104 months) post injury. There were 7 type B-fractures and 21 type C-fractures according to the AO-classification [11] with 15 injuries belonging to the subgroup C-3 (Fig. 2). There were 9 fractures on the left side and 19 on the right side. In 11 patients the dominant arm was injured. Causes of injury included 8 high-energy traumas, 11 moderate traumas and 9 low-energy traumas. Seven fractures (25%) were open fractures (2
Clinical setup for strength-measurement.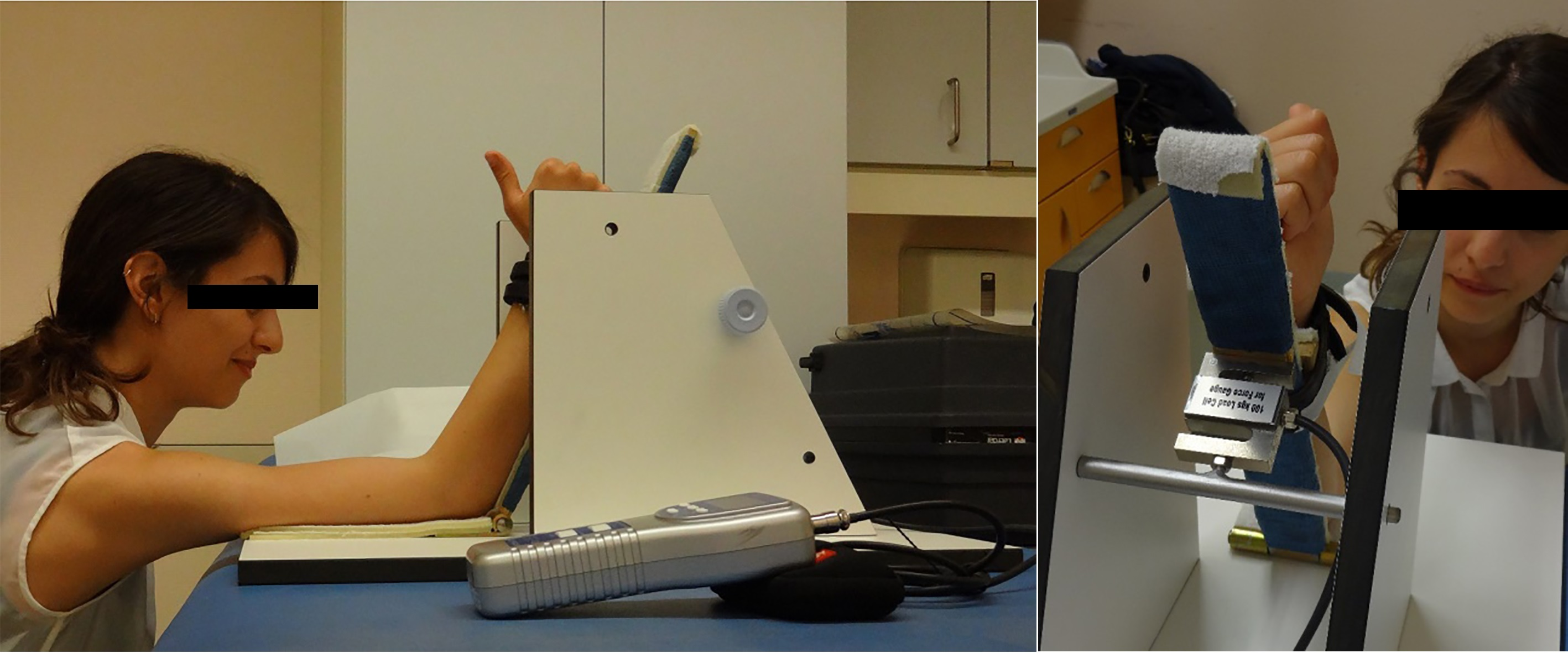
Age and gender distrubution at time of injury.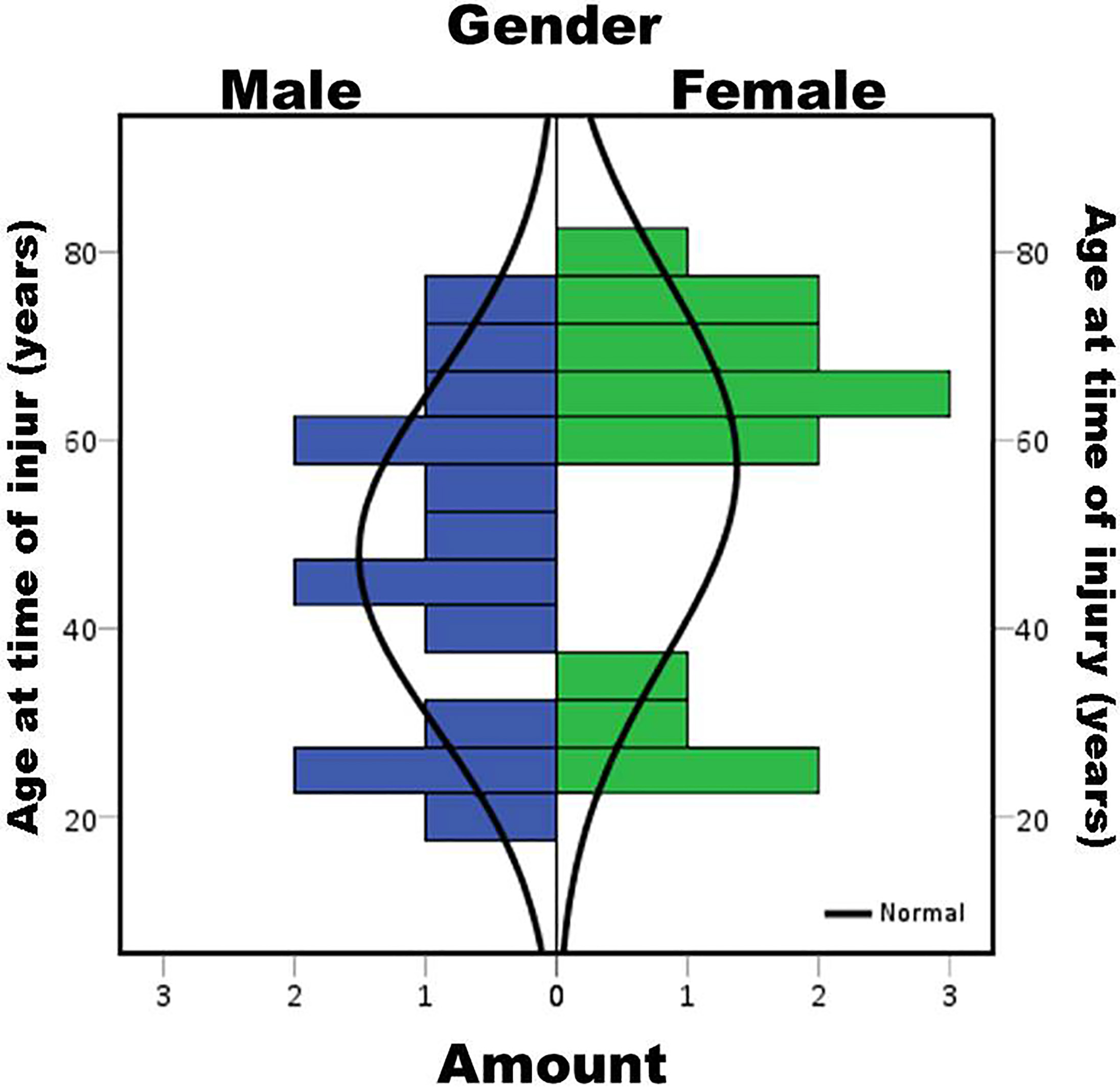
a. AP and lateral x-ray of a distal humerus fracture classified by AO/OTA as 13C3. b. Postoperative x-rays (ap and lateral) of the distal humerus fracture (AO/OTA 13C3) treated with double plating osteosynthesis (angle stable implants). c. AP and lateral x-ray of a distal humerus fracture classified by AO/OTA as 13C2. d. Postoperative x-rays (ap and lateral) of the distal humerus fracture (AO/OTA 13C2) treated with double plating osteosynthesis (conventional implants).
All patients were treated operatively: 5 patients received osteosynthesis by screw or pin fixation only, in 23 patients a plate osteosynthesis was carried out (3
There was a high rate of complications (9 patients, 32.1%). In 4 patients (14.3%) surgical revision was necessary. One patient suffered of superficial wound infection. In 4 patients the ulnar nerve was irritated and in 1 of these patients a sensible neuropathy still remained at the follow-up. 14.3% (4 patients) had a non-union including 2 implant failures (7.1%) which had to be surgically revised. After, full bony consolidation was seen.
In 20 patients reduction of the articular surface of the distal humerus was anatomical, in five cases there was an intra-articular step of 1–3 mm and in 2 cases a step of
Radiologically, heterotopic ossification could be seen in 4 patients (2
ROM on the injured side was reduced to 114.1
For muscle force measurement the contralateral healthy side was defined as the control with 100%. The average maximum extension force was 87.9% in 30
Fracture type distribution according to the AO-classification.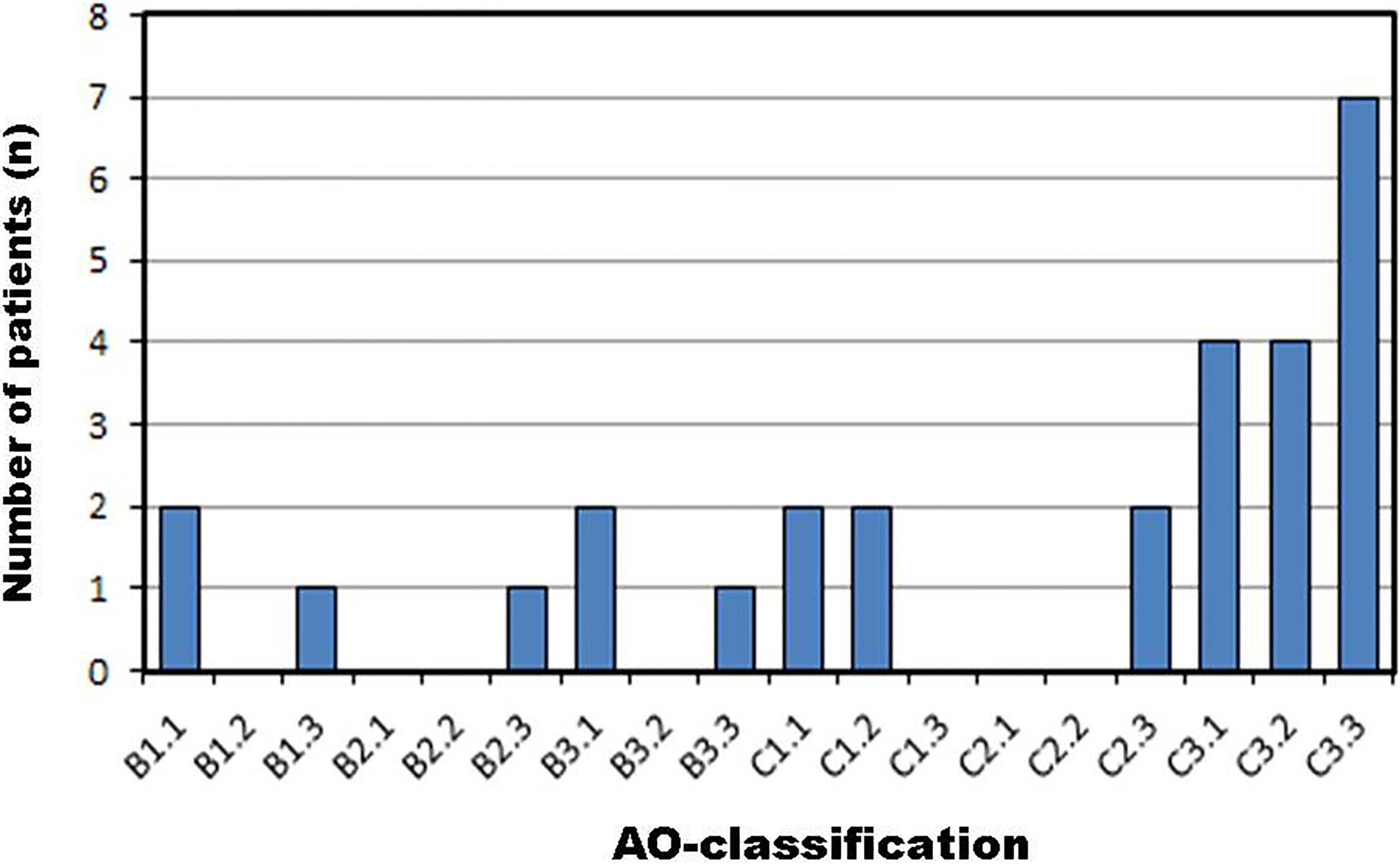
Average muscle force (extension/flexion in 30
MAYO score revealed 87.1 (
Correlations between outome (scores) and loss of flexion.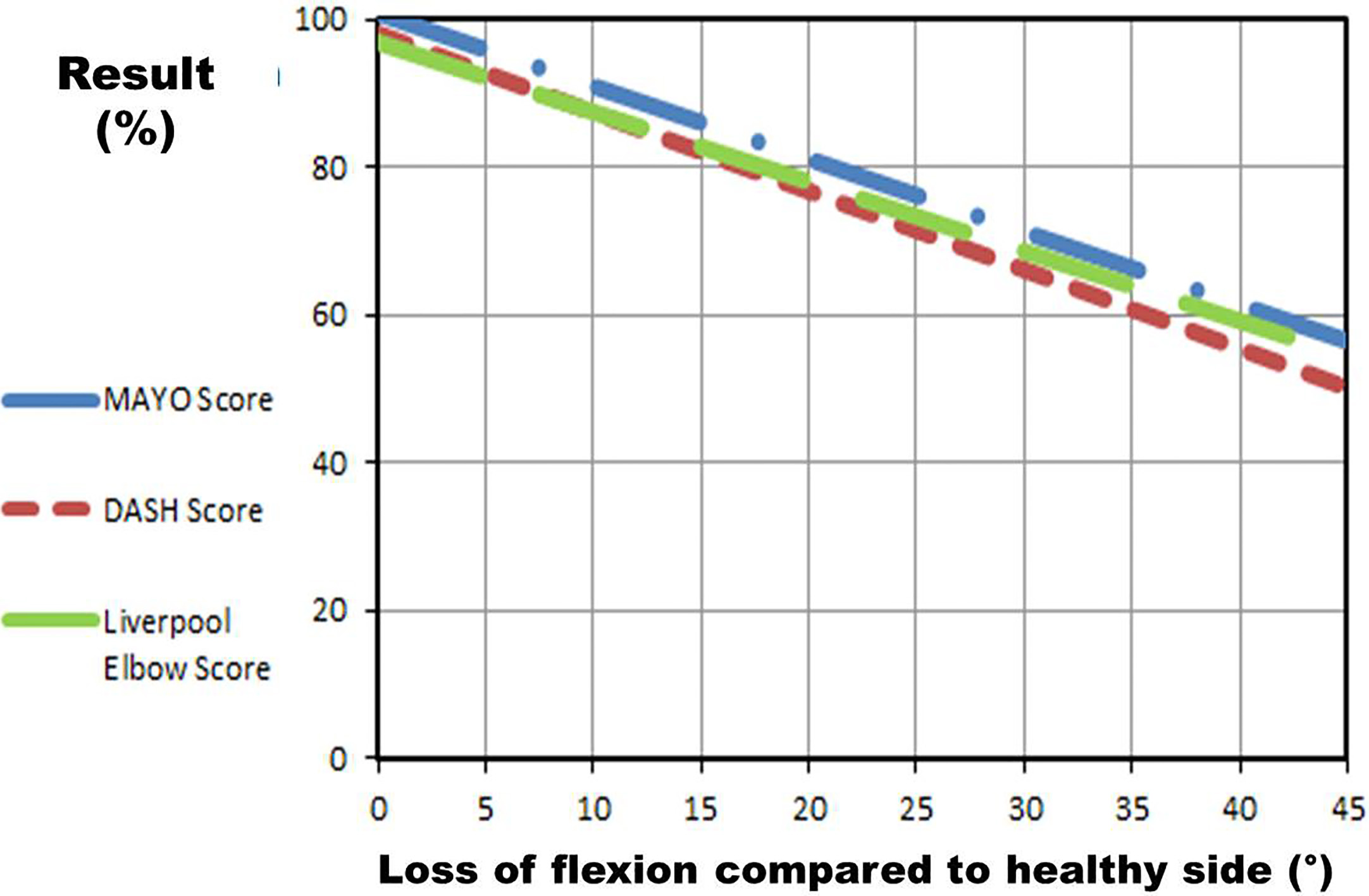
Correlations between outcome (scores) and reduction of muscle force.
Quality of life measured by the SF-36 questionnaire was reduced with a physical health of 46.1 (
There were differences in age distribution. In patients with more than 60 years of age (
Open reduction and internal fixation still remains the gold standard for the majority of distal intra-articular humerus fractures in order to restore the anatomy of the joint and in regard to the best possible function of the elbow joint [18, 19, 20]. The main benefit of operative treatment is the possibility of an anatomical reconstruction of the joint surface and the possibility of a timely postoperative functional treatment to reduce posttraumatic arthrofibrosis [6, 9].
Reconstruction of the radial and ulnar column by double plating is done in most of the cases. Due to the low incidence of these injuries there is only limited data on the functional results in the literature with rather small and often heterogeneous cohorts. Not only in osteoporotic bone multidirectional fixed-angle implants seem to be biomechanically superior. But until now, the clear advantage of these implants in distal intra-articular humerus fractures could not be demonstrated, especially in regard to the restoration of muscle force [2]. In contrast, regarding to Kaiser et al. [21] no complications like non-unions, loss of reposition or infection in a sub-analysis of ten patients over 60 years with a type C-3 fracture could be seen. The follow-up included 7 patients with MEPS of 86 points which was similar to the outcome of younger patients. Schmidt-Horlohé et al. [22] published results of their follow-up with 44 patients including 45 fractures 13 months post injury. In this study MEPS of the patients was 87.5 points with a DASH score of 14.2 points. Average ROM was 110
In accordance to the results of the current literature we can confirm that 71.4% of the patients had good to excellent results (MEPS
There is very limited data on reduction of force after distal humerus fractures. To our knowledge there are only two studies in the current literature with a partially comparable setup: Greiner et al. [7] showed similar results in 14 cases of AO type B- and C injuries with a flexion force of 75.3% and an extension force of 70.7% in a 90
In our study this particular bias was excluded by positioning the sensor just proximal to the ulnar head in a neutral position of the forearm. Overall, our results show a slightly reduced strength compared to the other studies with a flexion force of 81.5% and a extension force of 91.7%.
Limitation of the study: This is a retrospective study with a relatively small collective of patients although our collective is homogenous compared to other study setups. As there is still a lack of data showing the advantage of angle stable implants in distal intra-articular humerus fractures, a prospective randomized study is desirable.
Conclusion
Functional impairment in terms of reduced ROM and muscle force is a common complication after distal intra-articular humerus fracture. Patients older than 60 years have a higher deficit of motion in the injured elbow joint and an inferior clinical outcome. Superiority of modern angle-stable implants could yet not be shown.
Footnotes
Acknowledgments
This publication was funded by the German Research Foundation (DFG) and the University of Wuerzburg in the funding program Open Access Publishing.
Conflict of interest
All ICMJE Conflict of Interest Forms are on file with the publication and can be viewed on request. There are no conflicting interests that are related to the work submitted for consideration of publication.