
Abstract
BACKGROUND
: Fractures of the talus often lead to permanent restrictions of the affected limb. Possible alterations after these fractures in gait have not been evaluated yet.
OBJECTIVE:
To evaluate possible alterations of gait by pedybarography after talar fractures.
METHODS:
We conducted a retrospective single-centre study at a level I trauma center. Twenty patients with operatively treated talar fractures were followed up. Objective and subjective function of the ankle was measured using range of motion, clinical scores and dynamic pedobarography (emed-M; Novel, Germany).
RESULTS:
There were 11 talar neck and 9 talar body fractures. All patients received screw fixation. There was a significant reduction in range of motion. The outcome was moderate to satisfying and the severity of the injury correlated with the clinical outcome and the range of motion. The presence of posttraumatic arthritis and joint incongruity lead to a decreased function of ankle and subtalar joint and resulted in a worse clinical outcome. AVN rate was associated to initial displacement. Dynamic pedobarography showed no significant changes in gait pattern.
CONCLUSIONS:
Fractures of the talus lead to dissatisfaction, pain and malfunction. However, a change in gait pattern could not be proved.
Background
Fractures of the talus are extremely rare and make up less than 0.5% of all fractures. They often lead to devastating results and are a challenge to surgeons. Results are often dissatisfying for patients due to pain and malfunction and complications are common [1, 2, 3].
Talus fractures are mainly caused by high energy trauma a. e. car accidents and falls from great height. The classification systems divide the talus into head, neck and body fractures, of which the most common neck fractures make up to 50–80% [1, 2]. The widely-appreciated Hawkins classification for talar neck fractures differentiates three types based on the amount of dislocation and the involved joints [4]. A further type IV with additional dislocation in the talonavicular joint was later added by Canale and Kelly [5]. Marti and Weber introduced a further classification including talar body, neck and peripheral fractures (type I) according to the amount of displacement [6].
High complication rates have been reported. Besides malunion, infection and malalignment, especially the risk of avascular necrosis which is mainly dependent on the initial degree of displacement, is one of the greatest fears treating talus fractures and therefore anatomical reduction, surgical approach and soft tissue management play a substantial role [7, 8].
Studies have been conducted to evaluate the clinical outcome but not many have reported on changes in gait pattern including all types of fractures to the talus and not exclusively talar neck fractures.
Objective
The objective of our study was to evaluate the postoperative clinical and radiological outcome of fractures of the talus and show possible alterations to gait and load bearing as well as assess differences between talar neck and body fractures.
Methods
We conducted a retrospective study. It concluded all patients treated operatively at our level I trauma center with a fracture of the talus between 2007 and 2015. Inclusion criteria were: unilateral fracture, no other injury of the lower extremity, aged over 18 and an absence of psychiatric comorbidity. Inclusion criteria were strict to be able to allow the evaluation of pedobarographic results.
The study has been performed in accordance with the Declaration of Helsinki and has been approved by the ethical Committee of the University of Würzburg (Ethical Committee Approval no. 19/15).
Besides patients’ characteristics (age, gender, weight, fracture type, return to work, etc.), we evaluated the time to operation, operative procedure, cause of injury, complications and postoperative treatment. All patients received pre- and postoperative CT scans.
The follow-up consisted of a physical examination with measurement of range of motion of the ankle joint and subtalar joint, alteration of gait, soft tissue status as well as neurological status. The following questionnaires assessing the clinical postoperative outcome were obtained; VAS foot and ankle, AOFAS and Maryland Foot Score [9, 10, 11]. Radiological assessment was undertaken on the most recent available x-ray (a.p., sagittal) and the existence of posttraumatic arthritis graded according to Kellgren and Lawrence [12].
Dynamic pedography was carried out in an area measuring 1.2
Statistical analysis was carried out using IBM SPSS Statistics (version 17; IBM Deutschland Ltd., Ehningen, Germany). Shapiro-Wilk test showed normal distribution of the cohort. The student’s
Results
Forty-nine patients with operatively treated talus fractures between 2007 and 2015 were recorded. Twenty-five met the inclusion criteria. Twenty could be followed up (FU 80%) at an average time postop of 63 months (range, 20 to 122 months). One further patient had to be excluded from the pedography, as he had received an ankle arthroplasty due to osteonecrosis. Sixteen male and 4 female patients with an average age at time of accident of 30.7 years (range, 19–54 years). Nearly all fractures were due to high velocity injuries. Main recorded causes of injury consisted of falls from a height of over 1 m (30%) and road accidents (60%) as well as sport accidents (quad bike, paragliding).
The fractures could be divided into four groups: neck fractures according to Hawkins [4] (modified by Canale/Kelly [5]), fractures involving the body (including fractures to the lateral processus and fractures of the posterior processus) by Marti and Weber [6]. The largest group, talar neck fractures, consisted of eleven patients. There were three type I, four type II, three type III and one type IV fractures (Hawkins/Canale). There were nine talar body fractures by Marti and Weber of which there were six type I and three type II fractures. All patients underwent partial weight bearing (20 kg) for six weeks.
Only one fracture was open (type II Gustilo and Anderson [13], Hawkins I) and required a skin transplant after definitve fixation surgery. Time to operation was on average 4.75 days (range, 0–13 days). In one case an external fixation had to be used before definitive surgery could be performed. The average time of surgery was 119 minutes (range, 38–255 minutes). All patients were treated with screw osteosynthesis, in one case in combination with medial plate osteosynthesis (Fig. 1). In two cases, percutaneous screw fixation could be performed, which decreased time of surgery significantly (38 and 52 minutes). Surgery was always performed by senior consultants. The overall complication rate was 40% (
Postoperative complications
Postoperative complications
Case of 26 year old male with Hawkins type II fracture treated operatively with screw fixation.
Case of 30 year old male with avascular osteonecrosis 2 years postoperatively (a.p., and lateral view of x ray).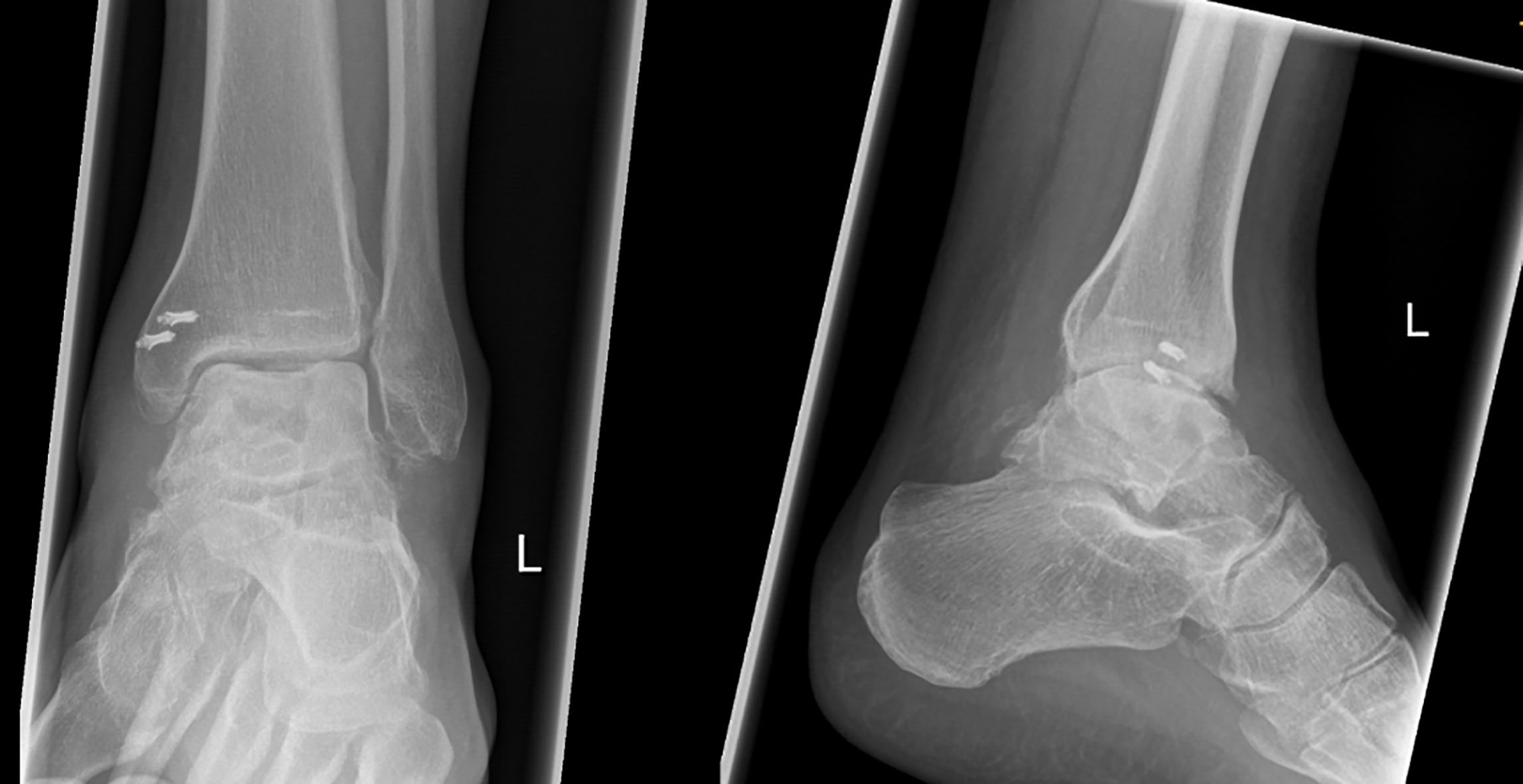
Malfunction consisted of a significantly decreased range of motion both for the ankle as well as for the subtalar joint on the fractured side in comparison to the healthy side (Ankle: 38.75 degrees
The clinical outcome was moderate to satisfying with mean scores of 64.25 points (AOFAS), 62.9 points (VAS) and 78.55 points (MFS). A positive Pearson correlation could be seen between range of motion and score outcome (
The severity of the injury in the group of talar neck fractures classified by Hawkins also showed a negative correlation with the postoperative clinical scoring in the AOFAS (
If postoperative complications occurred it resulted in a reduced range of motion of the subtalar joint (
Radiographic results were obtained and examined on the most recent available radiographs (average 640 days postoperatively). Posttraumatic arthritis was classified using the Kellgren and Lawrence classification [12] and was seen in at least early stages in every patient (11 type I, 5 type II, 3 type III and 1 type IV). In 50% of all patients both ankle and subtalar joint were involved. Further 10% also showed arthritic signs in the talconavicular joint. Postoperatively a CT scan was performed on every patient. The joint incongruity was measured in millimetres using the postoperative sagittal and coronar CT scan. Eleven cases showed a step of less than one millimetre. In seven cases a step of one to three millimetres was recorded and only two patients showed an incongruity of more than 3 millimetres. The greater the joint incongruity and the stage of arthritis the worse the postoperative outcome in scores and range of motion (
a. Pedobarographic force results. No differences in force can be detected. b. Pedobarographic pressure results. No differences in pressure can be detected.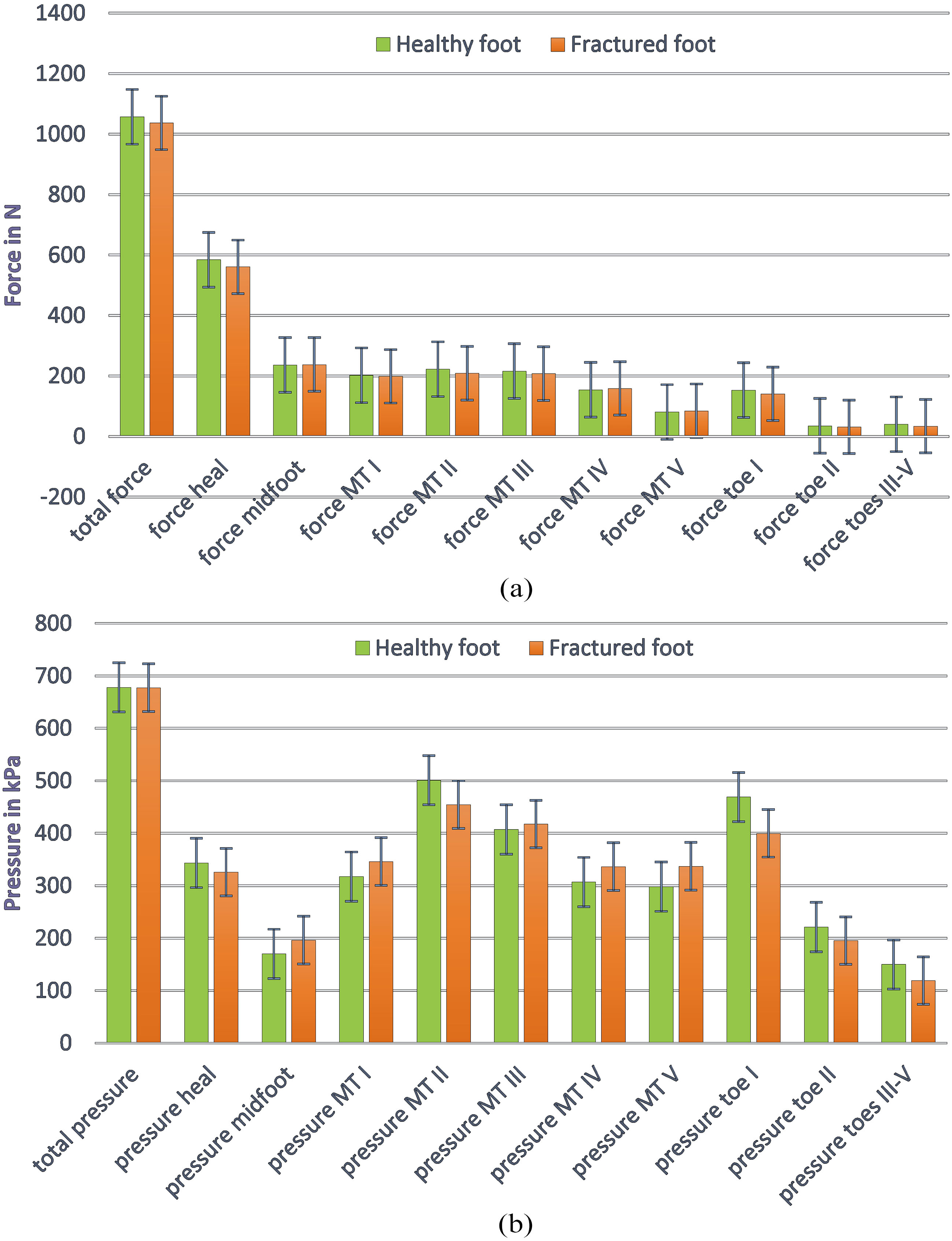
Fracture healing was recorded with all but three within the first six months.
There was one case of nonunion to the fracture of the posterior processus, but the patient had no problems and excellent clinical results so no revision surgery was performed. A further case of nonunion in a Hawkins type II fracture in combination with low grade infection was left without surgical revision due to comorbidities and lack of patient compliance. One type III Hawkins fracture showed a delayed union at eleven months postoperatively.
The pedography showed no significant difference for either force, pressure, contact time or roll over process between the fractured foot and the other side (Fig. 3a and b). Neither could changes be seen in the subdivided parts of the foot. Only in a small amount of areas a correlation was shown between the pedobarographic results and the clinical outcome.
Treatment of talus neck fractures is still extremely challenging. Time of surgery, surgical approaches and the risk of complications have been widely discussed in recent literature as factors influencing the outcome. We aimed to discuss both clinical and radiographic results as well as pedobarographic findings and compare talar neck and talar body fractures.
In our group of 20 patients with singular, ipsilateral talar neck (
We could not show any significant changes in gait pattern as for plantar pressure and force in our cohort. Colak et al. proved differences in pedobarographic findings in a similar setup to ours following up 19 patients with talar neck fractures [16]. They showed a reduced peak pressure and force in the hindfoot and an increase of pressure in the forefoot. The average follow up was much shorter in comparison to our study (29 vs 57 months), so changes may be less likely at a later stage and could explain the lack of changes in our study. Second, they did not exclude patients with multiple injuries to the extremities which may lead to biased results.
Posttraumatic arthritis is a major issue after talar fractures. In our cohort over 50% of all patients showed changes in the ankle as well as the subtalar joint and in fewer cases even involved the talonavicular joint. These findings are supported by other studies with rates of posttraumatic arthritis up to 100%.
Our overall complication rate of 40% coincides with the rates according to recent literature. We found a low infection rate of 10% (2/20) which is compatible to other studies. The non-union rate of 10% (2/20) was similar or slightly higher in comparison to other studies [11, 15, 17, 18].
We reported a low rate of avascular necrosis of 10%. Both cases occurred in talar neck fractures type Hawkins III. Therefore, we had an AVN rate of 66% of all type III Hawkins fractures. None of the talar body fractures showed any signs of AVN.
Vallier et al. elaborated predictive indicators for AVN and concluded that the main predictor is the degree of initial dislocation and therefore interruption of blood supply [18, 19, 20]. Immediate reduction is widely approved but as Vallier did we neither found any correlation between delay of definitive fixation and an increasing risk of AVN. Both our cases of AVN were associated with a great dislocation at time of injury. With only one open fracture it is not possible for us to make any conclusions about open injuries increasing the risk for AVN.
Treatment options for AVN are still being discussed. In a systematic review by Gross et al. [21] options were divided in two groups: joint sacrificing (arthrodesis, arthroplasty, talectomy) and joint sparing procedures (conservative, bone graft). Conservative methods mainly means prolonged partial weight bearing and splinting and does often lead to the necessity of further operative procedures. But is definitely an option, especially for patients with comorbidities at high risk for an operation.
DeVries [22] discussed retrograde intramedullary nail arthrodesis for AVN patients and reported about good union results. The study does not elaborate on the clinical patient outcome and satisfaction.
Bone grafting is a well-used treatment option and also undertaken in our study. Both patients with AVN after type Hawkins III fractures underwent revision operations with bone grafting for the distal tibia or the pelvis combined with bracing and partial weight bearing for at least 12 weeks, but still showed poor postoperative functional results. Nunley and Hamid [23] recently described a vascularized pedicle bone graft as a reliable method resulting in adequate pain relief and improved functional outcome.
Especially joint replacement as well as talectomy should still be seen as last options and salvage procedures instead of first line treatment.
But we did find that the length of the operative procedure was significantly higher in the group of patients with postoperative complications. Therefore, if adequate reduction and fixation is possible percutaneous or minimally invasive surgery should always be considered.
As also seen by Sanders et al. we showed the presence of postoperative complications to result in worse clinical outcome (scores) and a reduced range of motion [15].
Talar neck fractures presented with a lower range of motion of the ankle joint and achieved less satisfying results in the clinical scores in comparison to talar body fractures. This stands in contrast to findings of other studies. Elgafy et al. were able show better postoperative results of talar neck fractures than body fractures [24] whilst Ohl et al. showed no significant difference [14]. In our study, most body fractures were Marti and Weber type I which may explain the good outcome.
Limitations of our conducted study are the small number of patients but as for the rarity of talar fractures it is difficult to find large cohorts and to be able to have reliable pedographic results injuries should be singular and limited to one side.
Conclusion
Fractures of the talus are rare but challenging injuries and very often associated with high complication rates. The postoperative outcome is not always satisfying for patients and often leads to permanent pain and lack of function in daily live. Anatomical reconstruction and the immediate treatment in case of dislocation are standard but we could not demonstrate better clinical results by immediate fixation. But if postoperative complications occur this has a major impact on the outcome especially the presence of avascular necrosis. In cases with complications we saw a very much longer duration of operative procedure so further studies investigating percutaneous or minimally invasive approaches emphasising time limitation should be performed. In our study, we could not show an alteration of gait pattern and axis caused by talus fractures. Further studies with larger cohorts have still to proof these findings.
Footnotes
Conflict of interest
None to report.