
Abstract
BACKGROUND AND OBJECTIVE:
Musculature affected during spondylodesis surgery may benefit and recover faster if supported by spine orthosis postoperatively.
METHODS:
This prospective study included 50 consecutive patients undergoing one- or two-level spondylodesis. The intervention group received a lumbar spine orthosis (
RESULTS:
Patients wearing an orthosis postoperatively reported a higher degree of subjective stability. However, both intervention as well as control group did not show any significant differences for each of the follow-up points regarding VAS, ODI or the use of analgesics.
CONCLUSION:
Wearing an orthosis has neither impact on subjective pain, the need for analgesics nor for postoperative functionality. However, patients reported that they profited from wearing the orthosis by feeling more stable, thereby nicely improving their postoperative mobility. Thus, novel patient reported outcome measures have to be developed to assess these features in future studies.
Introduction
Stabilizing lumbar spinal orthoses are widely used in the conservative treatment for degenerative, posttraumatic, or malignant situations to ensure spinal stability [1]. To provide intrinsic spinal stability, spondylodesis presents a suitable surgical treatment option for direct fixation. Both treatment concepts generate stability, yet spondylodesis may postoperatively not directly result in the individual perception of stability, while the orthosis’ restriction of patients’ trunk mobility results in the sensation of stability and the subjective feeling of security and shielding [2, 3]. These features may be advantageous to enhance postoperative treatment following spondylodesis. Thus, physiological healing processes are supported by biomechanical and sensatory means as intraoperatively damaged muscular structures experience relief of stress and tension and may regenerate faster by wearing an orthosis [4]. However, there is some evidence, that there are no significant differences between patients wearing a lumbar corset or brace in the postoperative phase after spondylodesis [5].
Thus, we aimed to investigate whether postoperative treatment using tight spinal orthoses has a significant effect on relevant clinical outcome parameters.
Material and methods
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional ethical committee and with the 1964 Helsinki Declaration and its later amendments. Written informed consent was obtained from all patients included in this study.
Inclusion and exclusion criteria
In this study all patients receiving a one- or two-level spondylodesis between L3 and S1 were included if they were older than 18 years, not operated previously at the spine, were free of relevant systemic diseases (e.g. diabetes) and had no neurological deficits. Furthermore, they were excluded if they had a restricted mobility due to osteoarthritis in major joints of the lower extremity. Patients that were pregnant or breastfeeding at the time of operation were excluded from the study as well.
Patient recruitment
All patients (
Clinical outcome parameters
Patients were required to answer several questionnaires preoperatively (t0), upon discharge from the hospital (t1; 5-9 days postoperatively), six weeks (t2), twelve weeks (t3), six months (t4), and twelve months (t5) after surgery. Questionnaires used were the Oswestry Disability Index (ODI – a score for assessing quality of life in relation to lumbar back pain) [6], a Visual Analogue Scale for back pain, a questionnaire regarding demographic data such as profession, gender, age, times of sick leaves, etc. and a questionnaire for evaluation of the usage of analgesics (according to the WHO analgesia scheme). To specifically evaluate the subjective sensation of stability when wearing a lumbar orthosis after spine surgery, patients were asked to rate how well they felt stabilized and protected by wearing the orthosis using a scale from “not at all” to “very good” and free text answers.
Spondylodesis and orthosis
In all patients, dorsal stabilization and posterior lumbar interbody fusion (PLIF) was performed using pedicle screws of the type WSI MX/PX-Titan
Statistics
Level of significance was defined as
Results
In total, 52 consecutive patients were primarily included in this study. For final evaluation there were 23 patients (12 females/11 males) randomly allocated to the orthosis group (Group 1) and 27 patients (15 females/12 males) in the control group (Group 0). Detailed demographic information is shown in Table 1.
Demographic data of both intervention (Group 1) and control (Group 0) groups. There were no significant differences between both groups regarding gender, age, or BMI
Demographic data of both intervention (Group 1) and control (Group 0) groups. There were no significant differences between both groups regarding gender, age, or BMI
There were two patients lost for follow-up. One patient rejected further participation in this study due to uncomfortableness of wearing the orthosis and another patient died of coronary ischemia immediately after surgery (both Group 1).
There were no significant differences for attested sick leaves preoperatively. This regards all categories of sick leaves starting from less than three months to more than 12 months within the past 24 months preoperatively (
Periods of incapacity to work prior to surgery. For each category/period of incapacity to work, there were no significant differences between both groups.
In both groups the peak value for ODI was recorded immediately after surgery (Group 0
Oswestry Disability Index. Shown are cumulative ODI scores for each point of follow up (preoperatively (0), one week after surgery (1), six (2) and twelve (3) weeks after surgery as well as six (4) and twelve (5) months after surgery). At all points of follow-up there were no significant differences between both groups.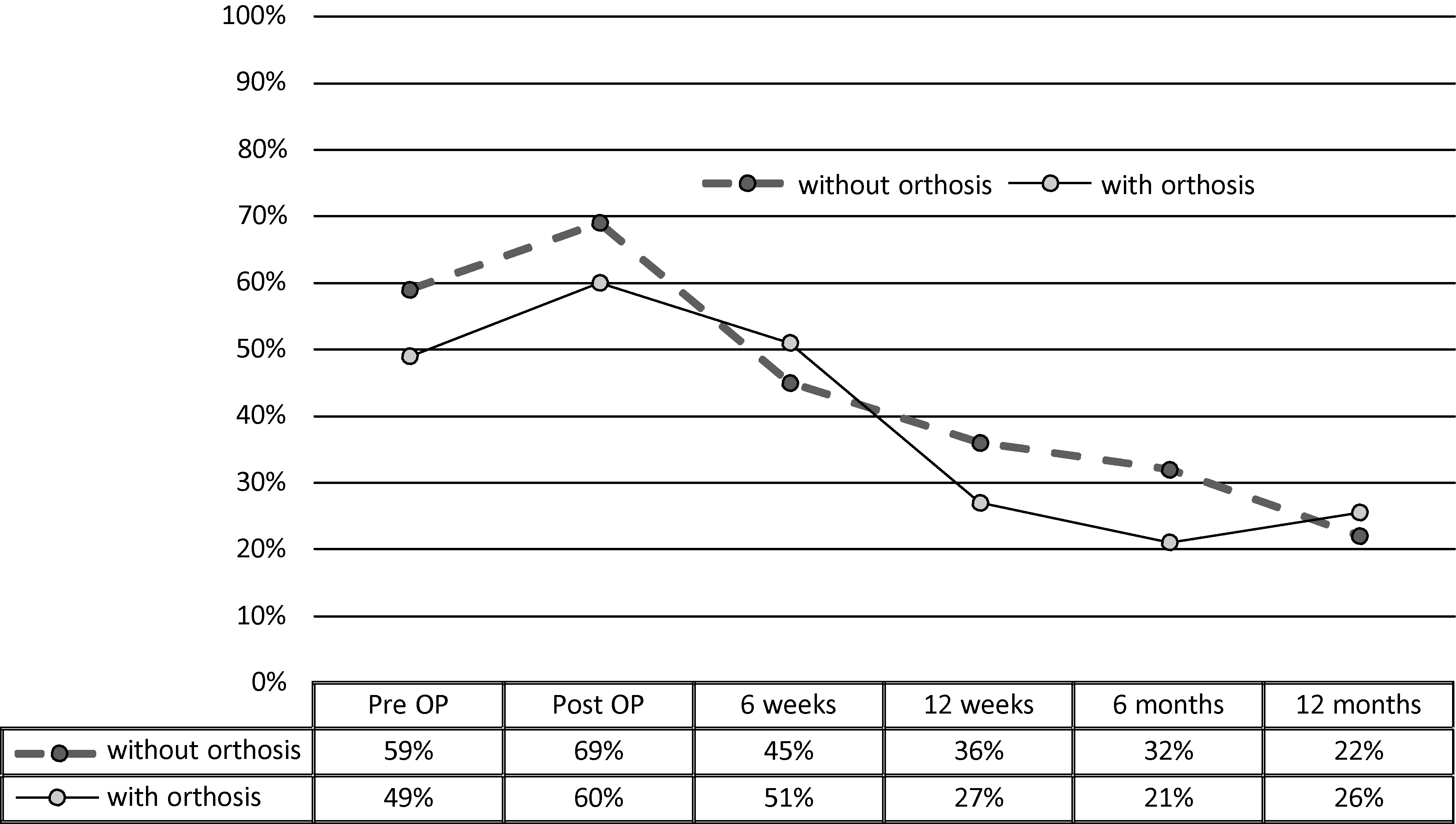
Baseline value for VAS-pain was VAS
Visual Analogous Scale for pain. Shown are cumulative VAS values for each point of follow up (preoperatively (0), one week after surgery (1), six (2) and twelve (3) weeks after surgery as well as six (4) and twelve (5) months after surgery). At all points of follow-up there were no significant differences between both groups. 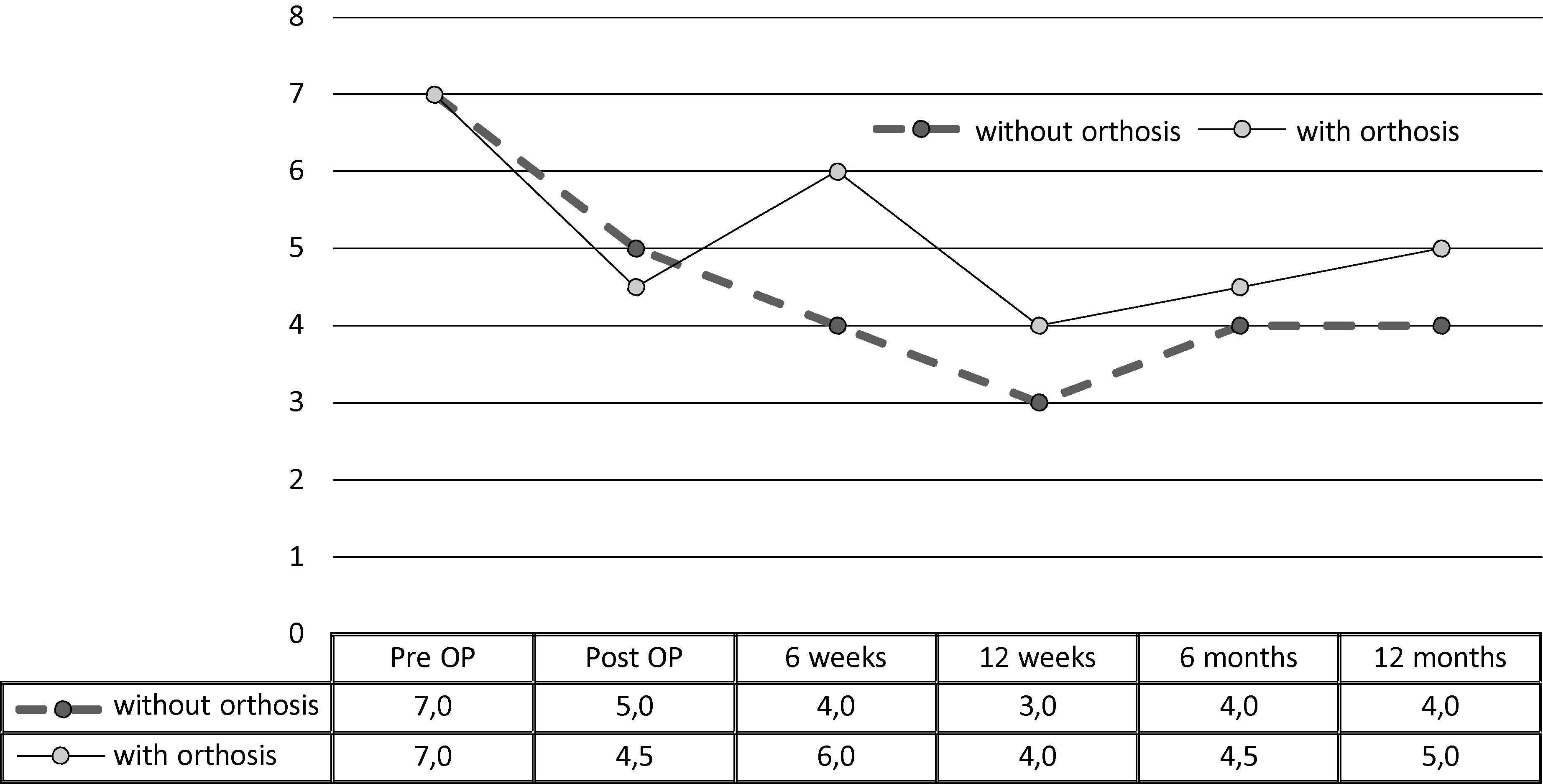
Preoperative need for analgesics was similar in both groups (
Need for analgesics at all points of follow up according to the WHO analgesia scheme. Although some differences were recorded between both groups, none of these was significant which is in accordance to recorded pain levels (VAS).
At all times of this study, Group 1 patients felt a sense of additional security, which was not the case in Group 0 (Fig. 5). Thus, 48% of patients at the six-months follow-up stated that they were wearing the orthosis for 1–5 hours per day and 8% for 5–10 hours per day. At twelve months postoperatively, the ratio of patients wearing a spinal orthosis for 1–5 hours per day decreased to 17%.
Subjective sensation of stability when wearing a lumbar orthosis after spine surgery. In the initial postoperative phase, more than two thirds of all patients described an “excellent” feeling of stability. At later points of follow-up, this effect was reduced but more than 90% of all answers remained within the top two categories “excellent” and “very good”.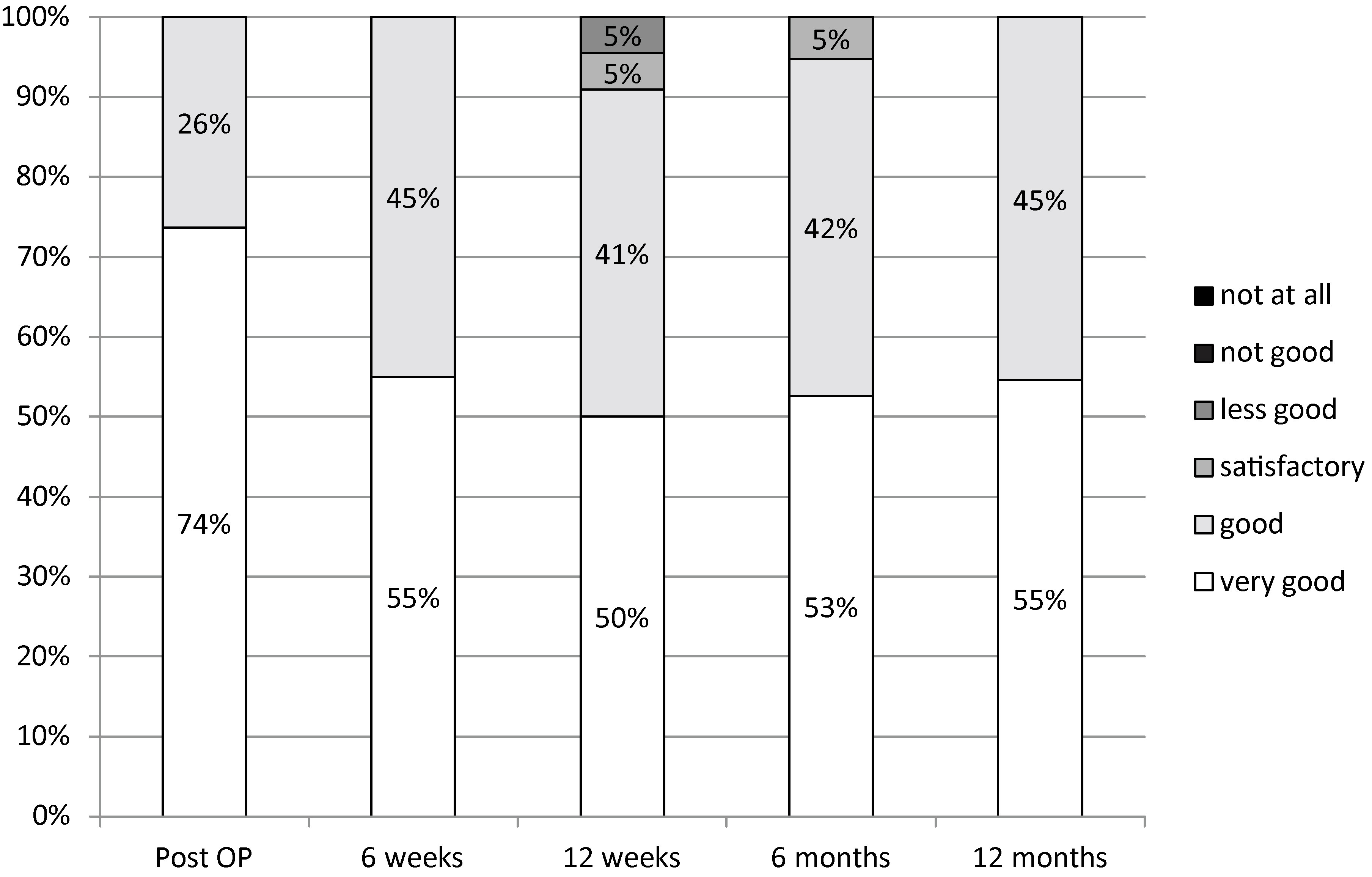
Back pain is one of the most important diagnosis for sick leaves or inability to work and thus imposes an immense economic burden [7]. Furthermore, the number of spine surgeries performed per year is constantly rising [8]. This is especially important as the peak prevalence of back pain is among patients aged 55 to 59 years [7] – a collective of established and experienced workers- which will create large secondary costs if absent from work (which is well reflected by the mean age of patients included in this study) [9]. Hence, it is of great interest to investigate and optimize postoperative treatment procedures in order to return patients to activities of daily life and work as quickly as possible. Consequently, this study investigated the influence of postoperative use of stabilizing back orthosis and whether this treatment may result in improved clinical outcomes and regeneration.
The rationale for the use of a brace or corset depends on the goals of therapy. Such goals may include limiting mobility, aiding in the relief of pain following surgery, improving fusion rates, or improving patient-reported functional outcomes. In principle, tensioning strap systems extending from the abdomen in a dorsocranial and dorsocaudal direction are integrated to build a three-point principle, which has the effect of reducing lordosis.
Moreover, ventral fasteners, which have a low level of elasticity, can result in increased intraabdominal pressure, thus straightening the lumbar spine region and providing relief for the back extensor muscles [10]. So far, numerous authors have reported the use of lumbar braces or corsets [11, 12, 13, 14] and another study by Yee and colleagues did not find any significant differences if corsets were worn or not [5]. Furthermore, it has been debated controversially for which exact period of time an orthosis should be worn postoperatively. A study by Connolly and Grob recommended that an orthosis should be worn for six to twelve weeks, depending on the type of fusion [15]. In an expert questionnaire, Bible et al. described postoperative use of up to eight weeks [16].
In our study, we found a significant pre- to twelve-months postoperative decrease in ODI values with an average decrease of 30% (37% Group 0, 23% Group 1). This is in accordance to a study by Glassmann et al. which described an improvement of up to 22.2% one year postoperatively after lumbar fusion [17]. Interestingly, the vastest decline for ODI values is recorded between t1 and t2 for the non-orthosis group, whereas the major decrease for the orthosis group was detected somewhat delayed between t2 and t3. It was only after t2 that the stabilizing back pad was removed from the orthosis, thus giving the patient greater sflexibility. It is unclear whether the detected major improvements in ODI values between t2 and t3 in the orthosis group were reliant on the initial six-week phase when movement was restricted or if an earlier removal of the lumbar pad from the orthosis would have resulted in an earlier improvement of ODI values.
Six months postoperatively, the orthosis group performed insignificantly better in terms of ODI than the non-orthosis group (Group 0: 32%, Group 1: 21%;
Strengths of this study were its prospective design and the use of multivariate outcome parameters. Further studies may investigate functional outcome parameters and include larger patient numbers for a sufficient study power as well as a longer follow-up.
Conclusion
No significant advantage for either group was found for any of the parameters measured.
Wearing an orthosis had no impact on subjective pain and could not reduce the need for analgesics either. The orthosis was also used as an aid in everyday situations even beyond the study protocol and it can therefore be regarded as a suitable aid for coping with the activities of daily living. Patients reported that they profited from wearing the orthosis by feeling more stable. Therefore, especially elderly and anxious patients can profit by an orthosis to help them gain more mobility. Specific tools and questionnaires assessing the patient comfort and soft parameters such as well-being wearing spinal orthosis should be designed for future studies.
Footnotes
Conflict of interest
None to report.