
Abstract
BACKGROUND:
Lesions of articular cartilage represent a crucial risk factor for the early development of osteoarthritis. Autologous chondrocyte implantation (ACI) is a well-established procedure in therapy of those lesions in the knee. The aim of the presented study is to detect differences in short-term radiological outcome depending on defect localization (femoral condyle vs. retropatellar) after spheroid-based ACI.
OBJECTIVE:
This study aimed to demonstrate that radiological outcome after spheroid-based ACI in the knee is independent of defect localization.
METHODS:
MRI-scans after retropatellar ACI and ACI of the medial/lateral femoral condyle, with a preoperative Outerbridge grade of III or IV were evaluated regarding MOCART 2.0.
RESULTS:
The mean defect-size was 5.0
CONCLUSIONS:
The presented data demonstrate good to excellent radiological short-term results after spheroid-based ACI. Data indicates, that at least radiological results are independent of gender, defect-size and defect-localization.
Introduction
Lesions of the articular cartilage represent a crucial risk factor for the early development of osteoarthritis, which could lead to complete destruction of the joint. Furthermore, osteoarthritis leads to pain and immobilization, and finally it represents a high burden for the health care systems.
Hyaline cartilage represents a unique structure, which is composed of water (70–80%) and extracellular matrix (ECM) with low cellularity and without any blood vessels or nerve fibres [1, 2]. This structure and its special biochemical composition enable hyaline cartilage to deform under pressure and remodels itself into its original form when pressure decreases [3]. However, hyaline cartilage nearly has no capacity to regenerate after trauma, which means that cartilage defects can lead to accelerated degradation of the joint, especially in younger people.
To prevent this and to postpone degenerative changes, different strategies are available for the treatment of cartilage lesions such as mosaic arthroplasty, microfracture, autologous matrix-induced chondrogenesis (AMIC) and autologous chondrocyte implantation (ACI). A relatively new technique represents the “minced cartilage” repair technique, a single-stage procedure, which uses minced cartilage from a less weight-bearing area of the knee. Massen et al. report satisfactory results after treatment of cartilage defects in the knee [4]. However long-term results and histological results are missing for this technique.
Matrix-based ACI (MACI) represents a third generation ACI. In contrast to first and second generation ACI, cultured cells are seeded on a scaffold, which gets implanted in the defect or come as spheroids. There is no need any more of covering the defect with f. e. periostal or collagen flaps [5, 6]. Moreover, spheroids do not require special fixation. Another advantage described, is that extracted cells keep their phenotype and do not dedifferenciate, like it is typical for chondrocytes in a foreign environment [5, 7]. Nevertheless, there is evidence, that MACI does not offer a significant superiority versus conventional ACI [8]. Bartlett et al. report about 42.9% hyaline cartilage in ACI treated defects, while MACI reached 36.4% here [9]. Taken these findings together, it can be concluded that that MACI simplifies the surgical intervention but does not deliver a significant better performance.
Various studies investigated the effectiveness of these strategies clinically, radiologically and histologically. The comparison of ACI with mosaic arthroplasty by Bentley et al. revealed excellent results in all cases [10]. Zeifang et al. compared ACI with MACI and reported no significant differences in these techniques by using the IKDC-score, Tegner-activity and the SF-36, but significant better results in the Lysholm-score for the ACI-P [8]. In 17 of the 21 patients, radiological MOCART score was performed, where ACI seemed to perform better than MACI again. Gooding et al. [11] could not detect significant differences between ACI covered with a periostal flap (ACI-P) and ACI covered with a collagen membrane (ACI-C) by performing histological safranin-O staining. A large histological evaluation of ACI was performed by McCarthy et al. Authors found good results for both techniques, with a slight superiority in the clinical outcome for ACI-C, even when the histological ICRS II score did not show a significant difference [12]. Compared to other techniques, a relatively small amount of literature deals with spheroid-based ACI.
Spheroid-based ACI showed superiority compared to microfracture in Activities of Daily Living at 24 months and Knee-related Quality of Life at 12 months [13], demonstrated excellent histological results [14] and proved safety and efficacy [15]. Niemeyer et al. examined the clinical outcome and success of ACI for cartilage defects of the patella and concluded that it leads to a high success rate with better results than the already excellent results in patients with the defects of the femoral condyle [16]. Mid-term results with a minimum follow-up of 4 years presented by Schlumberger et al. showed that ACI with in situ crosslinking matrix is a safe and reliable treatment for full-thickness cartilage defects of the knee [17].
Magnetic resonance imaging (MRI) is well established method in evaluation of chondro-regenerative therapies. Here, the MOCART-score has proven its worth and has lately been modified (“MOCART 2.0”) [18, 19].
In this study, we analysed 23 MRI-scans performed between 5 and 19 months postoperatively after spheroid-based ACI using the MOCART 2.0. Despite the fact, that load retropatellar as well as after-treatment after ACI is quite different to the femoral condyles, our hypothesis H0 was, that radiological results after spheroid-based ACI on the knee are independent of lesion localisation.
Methods
Twenty-three patients were treated with spheroid-based ACI (Spherox or Chondrospehere, Co.don, Teltow, Germany) due to focal chondral lesions retropatellar or of the medial femoral condyle, respectively the lateral femoral condyle in on case, with an Outerbridge grade of III or IV. ACI was performed as a two-stage procedure. In a first surgery, two cartilage-bone cylinders were harvested using a standardized cartilage biopsy tool with a diameter of 4 mm (Storz, Tuttlingen, Germany) from the intercondylar notch arthroscopically. After cell cultivation, the transplant comes in spheroid-form, small spheres, which contain of around 200.000 chondrocytes each. Implantation of delivered spheroids was performed via mini-arthrotomy and the use of a tourniquet with a pressure of 250 mmHg as a standard procedure following a period of approximately 8 weeks. Despite the fact, that implantation can be performed arthroscopically [20] when using the spheroids, we prefer a mini-open technique due to better transplant control in case of transplant-disclocation. Spheroids were applied after debridement of the cartilage defect to the subchondral bone trying to avoid bleeding for the subchondral bone. A special fixation of spheroids is not required. In case the defect was located retropatellar, up-standing of the patella was performed using a 2 mm k-wire as a joystick. Patients who underwent additional surgical procedures at the same time (f. e. MPFL-reconstruction, trochlea reconstruction) were excluded from the study. All patients included showed physiological leg axis, confirmed by anterior-posterior X-ray of the whole leg preoperatively. MRI scans of 23 knees after spheroid-based ACI were evaluated. Postoperative treatment followed our established standard and includes a magnetic resonance imaging (MRI)-scan between 6 and 12 months postoperatively.
MRI-imaging included the following sequences:
Proton-density weight spectral attenuated inversion recovery (PD SPAIR) were in all directions in space (axial, coronar, sagittal) T1-weighted Turbo spin echo sequence (T1 TSE) in sagittal and coronar slides
All MRI scans were performed at a magnetic field strength of 3 Tesla (Philips Ingenia 3.0 T, Philips, Amsterdam, Netherlands) in our institute for diagnostically and interventional radiology. MRI-scans were evaluated according the MOCART 2.0 criteria published by Schreiner et al. (Table 1) [19]. Statistical analysis was performed using SPSS 26 (Armonk, New York, USA). Due to non-normally distributed variables, Mann-Whitney U test was used for statistical analysis. A
Items addressed by the MOCART 2.0 score. MOCART
Descriptive patient data with mean values and standard deviations for MOCART 2.0 and its subitems of the 23 MRI-scans
Failure of ACI on the medial femoral condyle with poor defect filling and a MOCART 2.0 of 25 in a 53-year old female. MRI scans show a sagittal (left) and a coronary (right) slide.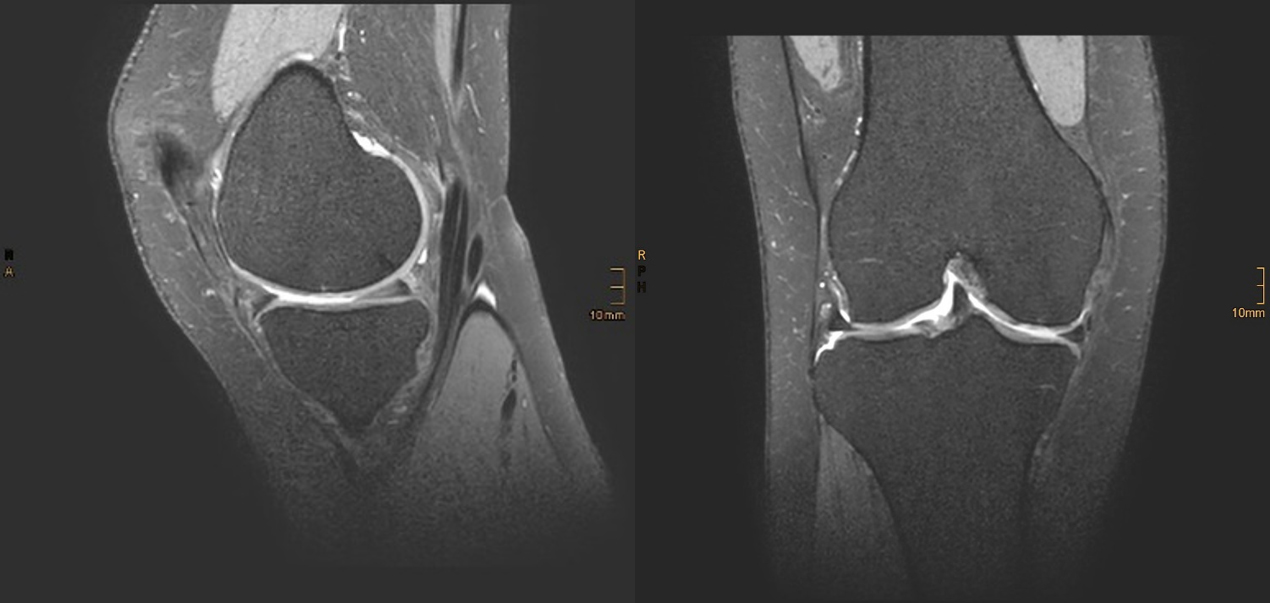
Satisfying results after spheroid-based ACI. First row: MRI-scan after ACI on the medial femoral condyle in the coronar (left) and sagittal (right) view. Second row: MRI-scan after ACI retropatellar in the axial (left) and sagittal (right) view. K-wire entrance in the patella is detectable in the sagittal view (down right).
Twenty-three knee MRI-scans of 14 males and 9 females with a mean age of 33.9 years (
Discussion
In this study, we performed retrospective evaluation of 23 MRI-scans after spheroid-based ACI on the knee. The technique demonstrated good radiological results (Fig. 2) with a mean MOCART 2.0 score of 78.5 (
-values for defect localisation (femoral condyle vs retropatellar) regarding MOCART 2.0 and its sub-items. There was no statistically significant difference regarding MOCART 2.0 or any subitem between ACI on the femoral condyle and retropatellar
MRI scans are the gold standard of non-invasive diagnostic for evaluate articular cartilage and articular cartilage repair tissue. In 2004, Marlovits et al. defined criteria for the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART)-score [25], which is established as standard in the evaluation of cartilage-repair procedures and allows an objective and standardized rating of the regenerated tissue. This score was further developed by Schreiner et al. with the introduction of MOCART 2.0 [19]. Authors argue, that MRI-imaging made distinct progress since introduction of MOCART, which made changes of the score necessary. Because of this, we decided to use MOCART 2.0. This fact may slightly limit the comparability with other studies, which used just MOCART.
Good radiological results for ACI were published by several authors [26, 27]. McCarthy et al. reported a mean MOCART of 70 12 months postoperatively for ACI with periostal flap (ACI-P) as well as for ACI with collagen membrane (ACI-C) and conclude, that MRI 12 months postoperatively can predict long-term results [26]. Beside good clinical and radiological results, Barie et al. reported revision-rates of ACI-P and MACI of around 30% in their long-term mean follow-up [27].
In our study, MOCART 2.0 results were not affected by defect size nor defect localization (medial femoral condyle and retropatellar). However, a higher patient-age as well as lesion
Some limitations of the study have to be mentioned. The study presented only focused on radiological outcome of spheroid-based ACI and MRI-scans were performed relatively early postoperatively, which is why it’s expressiveness regarding clinical and long-term results is highly limited for sure, even authors predict good clinical long-term results, in case of good MRI results one year after surgery [26]. Our results showed that the cartilage recovery in a short-term follow-up is good to excellent, so there would maybe just a little benefit of a longer follow up. Patients want to know what’s going on in a short term and how it looks like within a half- or year after surgery. Moreover, even we could show good and in some cases excellent radiological results, we do not have tissue samples to collect histopathological data. Good histological and immunhistological results were described for this technique, but in a relatively small number of specimen [14]. It is challenging to obtain the specimen for histopathological evaluation, due to limited indications for re-arthroscopy and tissue-sampling. Nevertheless, histology is commonly considered the gold-standard for the evaluation of tissue-quality.
The presented data demonstrate good to excellent radiological short-term results after spheroid-based ACI. Data indicates, that at least radiological results are independent of gender, defect-size and defect-localization.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.