
Abstract
BACKGROUND:
The effect of different thread designs and diameters on the all-on-four concept is unclear.
OBJECTIVE:
The aim of the study was to clarify the differences in stress distribution of dental implants with various thread designs and diameters based on the all-on-four concept with three dimensional (3D) finite element analysis (FEA).
METHODS:
A 3D model of a totally edentulous mandible was used to perform the FEA. Four different models (M1, M2, M3, and M4) including 3.5 and 4.3 mm diameter dental implants with active and passive threaded designs were generated. The dental implants were positioned according to the all-on-four concept. The Von Mises stresses on dental implants and maximum and minimum principal stresses (Pmax and Pmin) on bony structures were calculated under vertical, oblique and horizontal loads.
RESULTS:
For Von Mises stresses, the highest stress values were detected on the distal implants for all models. Distal implants had also the highest stress values for vertical loading. The Von Mises stresses were found to be concentrated around the implant’s neck. In all models the highest Pmax and Pmin stresses occurred in the bone surrounding the distal implant. It was noted that the active threaded implants showed the highest Pmax and Pmin stress values.
CONCLUSION:
The implant thread design and diameter might have a strong influence on the stress values in the all-on-four concept.
Introduction
Various degrees of resorption may be observed in alveolar bone due to teeth loss for a long time [1]. This resorption may cause difficulties when the implants are located closely to anatomic structures such as the maxillary sinus or nervus alveolaris inferior [2]. The treatment plan may be complicated due to the loss of posterior teeth, because of the problems in using the alveolar bone posterior to the mandibular nerve without the complicated augmentantion procedures [3]. As an alternative, Malo and colleagues have recently offered the all-on-four concept (All-on-4
The all-on-four concept is a simple and cost-effective treatment. Additionally, it provides immediate loading, which may be preferable for patients. A high success ratio and slight marginal bone resorption have been reported for the all-on-four concept (98.1 percent at five years and 94.8 percent up to 10 years) [5, 6]. High survival rates of tilted implants have been shown by clinical studies [7, 8].
Load transferring of an implant may be influenced by the variation of implant design [9]. Thread configuration is an essential factor in dental implant biomechanics. Threads help distribute stresses at the interface as well as increase initial contact, stability and implant surface [10].
Design parameters such as implant diameter affect loading transfer characteristics [11]. Studies have reported that the contact surface expands in parallel with the increase in implant diameter, which improves biomechanical behavior [12]. Increase in diameter is more effective in increasing peri-implant bone surface compared to implant length. With the increase in peri-implant bone surface area, a more homogeneous stress distribution is provided under functional loads [13].
It is important to know how the stress concentration on the implant and in the surrounding bone is affected by the thread design as well as the diameter for clinical success.
FEA provides researchers to evaluate stress distribution between implants and surrounding bone [14]. Recently FEA approaches have been used successfully in several all-on-four applications [15]. However, there has not been enough studies comparing the effect of thread design and diameter in the all-on-four concept to completely understand the mechanisms of stress distribution and load transfer from a biomechanical aspect [16].
The objective of our study was to clarify the differences in stress distribution of dental implants with various thread designs and diameters based on the all-on-four concept.
Materials and methods
The Cone Beam Computed Tomography (CBCT) scan data of a fully edentulous mandible with 16 mm vertical alveolar bone height and 8 mm bone width of a 53 year-old healthy male was selected for the creation of the 3D FEA model used in this study. Serial axial sections at every 0.5 mm level of the edentulous mandible were obtained from the NewTom 3G (Quantitative Radiology, Verona, Italy) CBCT imaging system. The CBCT images were recorded using DICOM 3.0 as a medical image file format and imported into Maxilim Software (Medicim Company, Mechelen, Belgium) version 2.2.2, a 3D medical image processing program. 3D imaging of the mandible with the stereolithographic (.stl) file format was transferred to MSC Mentat (MSC Software Corporation, CA, USA) version 2005 for preprocessing and modeling. To simplify the model reconstruction, the outer bone structure, representing the cortical bone, was designed to be 2 mm thick, and the remaining bone structure was designed to consist of cancellous bone tissue. Models were created on an orthogonal XYZ coordinate system. Mentat was used to construct the final model using 4-node isoparametric random tetrahedral elements.
In this research, a model of a 3.5 mm and 4.3 mm diameter, 11.5 mm length Nobel Active implants (active threaded implant) and Nobel Replace implants (passive threaded implant) and multi-unit abutments (Nobel Biocare, Zurich, Switzerland) were chosen. The geometric features of implants were modeled based on the engineering drawings using MSC Mentat.
Implants with different thread designs and varying width options were assigned to the atrophic mandible according to the standard all-on-four concept in four study models.
The models had two vertical and two tilted distal implants. Distal tilted implants were placed at an angle of 30
All-on-four models
All-on-four models
The designs of the models were as follows (Table 1):
All materials were assumed to be isotropic, homogeneous and linearly elastic. The elastic properties of the materials used in the models are shown in Table 2.
Mechanical properties of bony structures and dental implant material in finite element analysis
In order to simulate ideal osseointegration, it was assumed that the implant, surrounding bone and all prosthetic components were perfectly connected via contact surfaces without any relative movement.
All the final solid meshes were created by tetrahedral elements with four nodes using MSC MARC (MSC Software Corporation, Santa Ana, CA, USA). No experimental data has been reported in the literature to compare our results therefore, a convergence analysis has been performed. The results were assessed using the data of the Von Mises stress values of Model 1 for vertical load with changing number of elements and final numbers of validated elements and nodes (Fig. 1). Changes of
Element and node numbers in each model
Convergence analysis of elements and nodes.
The highest Von Mises, Pmax and Pmin stress values in the models, v: vertical; o: oblique; h: horizontal.
Models were constrained in all directions at the nodes on the mesial and distal bone surfaces. To evaluate the stress distribution of all models, the average biting force of 150 N was selected to represent masticatory forces which was obtained from the literature [17].
A wide range of values for masticatory forces has been defined in the literature [1]. A ratio of 5:2.5:1 has been reported for vertical (V), buccolingual (BL), and mesiodistal (MD) loads during mastication [18]. Therefore, in this study, a total vertical force of 150 N was applied to the entire occlusal surface of the prosthetic structure. To simulate oblique loading, a force of 75 N was applied to the framework with a 60
The Von Mises stress values on dental implants, Pmax and Pmin stresses on bony structures were predicted by means of 3D FEA. The models were compared with each other in terms of different thread designs and diameters. Von Mises stress values are described as the beginning of the deformation for dental implants; therefore, such values might be important in interpreting the stresses occurred within the implants [19].
Bone can be utilized as a brittle material from an engineering point of view. The principle stress values are appropriate when analysing the behavior of bone. The magnitude of the concentrations in bone was presented as maximum principal stress ( Pmax) (tensile stress) and minimum principal stress (Pmin) (compressive stress) with their location [19].
In this study, the M1-M2 and M3-M4 models were compared to evaluate the effects of the thread designs and the M1-M3 and M2-M4 models were compared to evaluate the effects of the diameter on Von Mises, Pmax and Pmin stresses. The highest Von Mises, Pmax and Pmin stress values are shown in Fig. 2.
Von Mises stress distribution patterns under vertical loading, a) Model 1, b) Model 2, c) Model 3, and d) Model 4.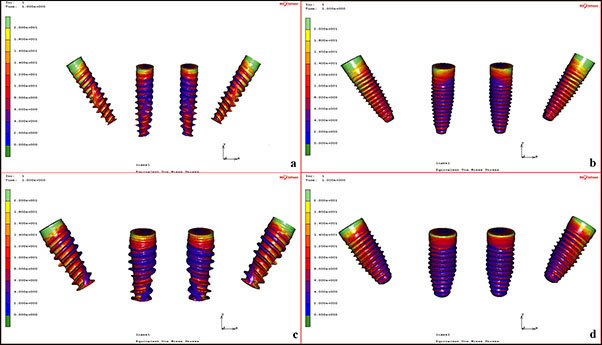
Vertical load case
Von Mises stresses on the models are shown in Fig. 3. The highest stresses were detected on the distal implants for all models. The highest stress value on the distal implant was noted on the M2 model. Comparison of M1 and M2 models revealed that M1 model had lower stress values than M2 model. Higher stress values were isolated on M3 model in comparison with M4 model. In the comparison made based on the diameters, it was determined that the stresses on distal implants decreased with the increase in diameter.
Oblique load case
When the models were compared, the highest stress values were found in distal implants due to the vertical component of the oblique load, but the remarkable point here was that the stresses in the mesial implants were increased in the models (M2 and M4) using passive threaded implants compared to the active threaded implants (M1 and M3). As a result of the comparison made with the diameter of the implants, it was observed that the stresses decreased as the diameter increased in distal implants.
Horizontal load case
When all models were evaluated, it was detected that the stresses in mesial implants were higher in passive threaded groups (M2-M4). When the models with active (M1-M3) and passive (M2-M4) threaded designs were compared based on the diameter, it was found that the stresses shifted to distal implants decreased as the diameter increased.
Evaluation of Pmax stress values
Vertical load case
As a result of comparison with Pmax stresses in vertical load case, it was determined that stresses in distal implants (M2-M4) were equal in the passive threaded groups, but mesial implants were exposed to more stress in wide diameter implants. When active threaded models (M1-M3) were compared, it was found that the stresses on distal implants were higher in wide diameter implants. In the comparative assessment of M1-M3 groups, it was noted that there was no remarkable stress change for mesial implants.
Oblique load case
High stress values have been observed in active threaded distal implants in comparison with passive threaded implants. In all groups, it was found that stress values in the bone surrounding the mesial implants decreased due to the increase in diameter. When the M1-M2 and M3-M4 groups were compared among themselves, decreasing stress values in the bone around passive threaded distal implants were noteworthy.
Horizontal load case
It was understood that the stress values around the passive threaded distal implants were lower than that of active threaded implants, and the widening diameter in mesial implants caused a decrease in the stress around the surrounding bone (Fig. 4).
Pmax stress distribution patterns under horizontal loading, a) Model 2 and b) Model 4.
Vertical load case
It has been noted that the highest stress values were located around distal implants. The comparison of the (M1 and M2, M3 and M4) models revealed that active threaded implants had higher stress values than passive threaded implants. Lower stress values have been observed around wide diameter implants in the comparative assessment of M1-M3 models (Fig. 5a and b). M2-M4 comparison showed that lower stress values were isolated around wide diameter for mesial implant and narrow diameter for distal implant.
P min stress distribution patterns: a) Model 1 vertical loading, b) Model 3 vertical loading; c) Model 1 oblique loading, d) Model 3 oblique loading, e) Model 2 horizontal loading and f) Model 4 horizontal loading.
The highest stresses were calculated around distal implants for oblique load case. In the comparison of M1, M2, M3 and M4 models Pmin stresses were noted to be higher for active threaded implants. When active threaded models (M1-M3) were compared, it was found that the stresses were lower around wide diameter implants (Fig. 5c and d). In the comparative assessment of M2-M4 groups, it was determined that the Pmin stresses for the narrow diameter implants were lower than the wide diameter implants.
Horizontal load case
Horizontal load case was similar with oblique load case. The highest Pmin stresses were detected around distal implants. When M1, M2 and M3, M4 models were compared the highest stress values were observed for active threaded implants. In the comparative assessment of active threaded models (M1-M3) lower stress values were isolated around wide diameter implants. Lower stress values have been noted for narrow diameter implants than wide diameter implants when passive thread designed groups (M2-M4) were compared (Fig. 5e and f).
Discussion
Finite element analysis (FEA) is a beneficial approach that provides precise overview of the mechanical behavior of the mandible under functional loads [20]. It is used to analyse stresses and deformations in structures of any given geometry [21]. It has advantages compared to another techniques in simulating the complex clinical conditions [22]. The experiments can be repeated, no ethical approval is needed and the study designs can be changed and modified [23].
Bone has an anisotropic nature, but it is usually modeled as being isotropic in FEA models [24]. In our study, all of the components of the FEA model were presumed to be homogeneous, isotropic and linearly elastic [25]. A 100% osseointegration was assumed around the implants [24]. The modeled mandible consisted of a spongy core surrounded by a homogeneous 2 mm cortical layer. An actual mandible has tighter bone at the lower border and less compact bone at the upper border. Therefore, limitations of the FEA should be taken into consideration [26, 27]. Also, the finite element model prediction must be compared with in vitro experiments to validate the simulated model. However, in the present study, relative comparisons were made for models instead of using absolute values. Therefore, only one convergence analysis was performed to validate our finite element models.
In our study, the biomechanical effects of implants in different thread designs and diameters used in all-on-four concept have been investigated with FEA. Four finite element models were created for the study. The Von Mises, Pmax and Pmin stresses were calculated under vertical, horizontal, and oblique load cases.
To improve clinical success, it is important to know how the stress distribution on implants as well as on the bone is changed by the shape, width and height of the thread [10]. Various finite element studies have investigated the efficacy of implant design parameters with implant thread analyses most often based on 2-dimensional simulation [10, 25]. This method was not accurate and some important information about the implant design parameters was lost [10]. In this study 3D finite element models were created and the stress values were calculated by means of 3D FEA.
The cantilever length is reduced by means of the tilting of distal implants, resulting in lower peri-implant bone stress [15]. However, the efficacy of thread designs on the stress distribution observed in dental implants and bony structures in an all-on-four situation is not clear.
The highest risk of bone resorption has been reported to occur around the neck of the implant. The cortical bone surrounding the implant neck has the highest stress values, which can be explained by the higher elastic modulus of the cortical bone compared to the cancellous bone and that the cortical bone is much stronger and more resistant against deformation [21, 22]. In this study, the Von Mises stresses were found to be concentrated around the neck of the mesial and distal implants which was more relevant in the distal implants.
There is a general opinion that as the diameter of the implant increases, the stress value decreases. This is particularly important for cortical bone, as increasing the implant diameter can reduce the amount of stress to which cortical bone in the neck surrounding the implant is subjected. Thus, the probability of success of the implant can be increased by preventing unwanted cortical bone resorption [13].
The present study also revealed that lower Von Mises stresses were calculated by increasing the diameter. It was also observed that these stress values decreased with the increase in the diameter of the distal implants.
The implant’s geometrical design is one of the most significant factors for implant success. A threaded implant design enhances the contact area and improves the implant stability. Since the size and shape of the threads might affect the stress patterns in the surrounding bone, the advantages of decreasing bone stress and mobility via improved thread designs remain to be demonstrated [28]. In our study, we evaluated the stress distribution of 3.5 and 4.3 mm diameter implants with active and passive threaded designs. Lower Von Mises values were observed in 3.5 mm diameter implants with active threaded design. Active threaded design has caused decreased Von Mises stresses on 4.3 mm diameter distal implants; whereas increased Von Mises stresses were found for 4.3 mm diameter mesial implants. Lower Von Mises stresses were found for 3.5 mm diameter mesial and distal implants with active threaded design in all conditions.
Several FEA studies have reported that the highest stress values are located around the distal implant, and this study also demonstrated that the highest stress concentrations were observed around the distal implant [15, 29].
From the bioengineering point of view, one of the important aspects in implant design is to create a geometry that minimizes peak bone stress under functional loads. The finite element method is used in dental implantology to analyse stress patterns at the implant-bone interface to compare various implant designs and clinical situations [29].
Dental implants show geometric differences in terms of thread structure, spacing, shape and depth. Threads are employed to increase the surface area of the implant. The use of different thread configurations has been suggested, since thread geometry is an important factor in the type of force transmission in clinical cases with different bone qualities [10, 12, 29]. The design of the implant threads has a direct effect on stress distribution and marginal bone resorption. Indeed, the stress areas around endosteal implants are associated with different thread designs and can lead to reduced bone stresses [22]. The present study also demonstrated the influence of the thread design on Von Mises and Pmax stress values.
The main parameter in the success of dental implants is the way stresses are transferred to the bone surrounding the implant. Vertical and transverse loads that occur during chewing affect axial forces and cause stress load on both the bone and the implant. The forces and moments to which the implants and surrounding bone are subjected depend on the type of loading, the bone-implant interface, implant and prosthesis design, and the quantity and quality of the surrounding bone [30]. In the current study, it was determined that Pmax tension values were higher in implants with active threaded design. The bone surrounding the distal implants also had higher Pmax values compared to mesial implants.
In general, compressive stress (Pmin) is more crucial than tensile (Pmax) stress and provides reliable information when evaluating bone resorption [31]. Reducing the magnitude of compressive forces and optimizing the stress distribution are critical for increasing long-term success of restorations [32]. In the present study Pmin stresses were found to be higher than Pmax stresses in all models, indicating that the bone stresses were mainly in compression. The highest Pmin stress values were noted in 3.5 mm diameter implants. Moreover active threaded design seemed to increase the Pmin stress values. Given the fact that compressive stress is an important indicator for a possible overload of bony tissues, the dental implant designs reducing compressive stress values should be considered in the treatment plan.
The stress values recorded in this research are lower than the fracture limit of the materials, and inclined implants allow us to avoid mental foramen and reduce cantilever length. It has been shown that the all-on-four concept is a feasible and conservative solution and can provide proper stress distribution in dental implants and surrounding bone. The all-on-four concepts made with appropriate implant design are considered to be an important alternative in the rehabilitation of severely resorbed mandible [33].
The present study aimed to simulate clinical conditions of all-on-four concept with different thread designs and diameters as accurately as possible. However, 3D FEA studies have some limitations in order to simplify the calculations. The finite element models were selected to be linear elastic for this study. This is found to be sufficient for investigating the effects of different thread designs and diameters on the biomechanical behavior of all-on-four concept. Linear elastic model is a simplification in which the time factor is ignored. As the present study aims to make a relative comparison of a clinical condition instead of identifying the absolute results, these assumptions are reasonable for modeling the stress patterns of dental implants and analysing their mechanical properties.
In the current study, 100% implant-bone interface was simulated but clinically partial contact between the implant and bone and osseointegration have been reported [2, 34, 35]. Another limitation was that only static loads were applied. Cylic loads, including those that occur during mastication, can result in different behavior for the prosthetic structures and bone tissue. Additionally, the boundary conditions were set to be fix at specific locations. Since the purpose of the present study was not to identify absolute stress values but to compare the biomechanical behavior of all-on-four implant concept with different thread designs and diameters, these limitations were equal for all models in this study. Therefore, these assumptions do not interfere neither with the qualitative nor the comparative results.
The findings of the current study provide a better understanding for the biomechanical behavior of the all-on-four concept and may contribute to an important point for the treatment planning of the atrophic mandible. The biomechanical effect of the thread design and diameter of dental implant for single tooth replacement has been described in the literature. This study may broaden this knowledge by finding that the implant thread design and diameter have a significant effect on the biomechanical behavior of all-on-four concept. This suggests that the biomechanical performance of the all-on-four concept would change by optimizing these parameters.
Conclusions
The current study results revealed that wide diameter implants generate more favorable stress distribution in the implant and surrounding bone when compared to narrow diameter implants. Furthermore, the active threaded design presented higher stress values than passive threaded designs. Although this study provides a wider understanding of stress distribution patterns in all-on-four concept, clinical trials with long term follow up are needed to demonstrate the prognosis of these findings in clinical practice. Furthermore, biomechanical studies focusing on different implant systems would contribute to increasing the clinical success and patient satisfaction.
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest.
Disclaimer
This study was presented as an oral presentation at the 24th International Scientific Congress of the Turkish Association of Oral and Maxillofacial Surgery. The congress was held on May 23–27 2017 in Muğla-Turkey.