
Abstract
BACKGROUND:
Thermoablation is an attractive treatment of thyroid nodules for its minimal-invasiveness. It remains unclear whether results and morbidity meet the patients’ expectations.
OBJECTIVE:
The aim of the presented study is to show data obtained after microwave thyroid ablation from a patients’ perspective.
METHODS:
Indications and preoperative diagnosis were chosen according to international guidelines. Thermoablation was achieved using a CE certified microwave system. The procedures heeded the published recommendations of the European Federation of Societies for Ultrasound in Medicine and Biology. Follow-up included ultrasound, laboratory parameters and a standardized questionnaire.
RESULTS:
Thirty patients were enrolled into the study. All patients reported an improvement of complaints following the procedure. Scar formation occurred in 3 cases (10%) with 0.5
CONCLUSION:
The presented data summarize an initial experience in selected patients and resemble excellent patient reported outcome with minimal morbidity. These preliminary data indicate the majority of patients satisfied with the procedure. Further trials will be required to endorse these findings.
Introduction
Local ablation evolved into a valuable treatment option for malignant nodules in the liver, kidney or other solid parenchymal organs. Thermoablation of benign thyroid nodules has also been proven to be safe and effective [1]. An exhaustive current review lists 17 prospective, 21 retrospective studies and 6 randomized controlled trials [2]. The European Thyroid Association has recently published a guideline for image-guided ablation of benign thyroid nodules [3]. In an international perspective, Lee et al. compared the existing recommendations and found numerous similarities and few discrepancies [4]. For the central-European German-speaking countries, a consensus statement and recommendations for the non-surgical, non-radioiodine treatment of benign thyroid nodules were published in 2020 [5], whereas a joint Austrian work group representing departments of surgery, endocrinology and nuclear medicine reviewed malignant as well as benign indications published in the literature [6].
Thermoablation of thyroid nodules is obviously a promising treatment option for benign disease, and even malignant lesions are frequently treated with increasing success [7]. Up to present knowledge, no malignant transformations are induced by thermoablation [8]. Meeting all requirements of minimal-invasive surgery, data on patient reported outcomes (PROM) are rarely reported. Quality of life (QoL) following thermoablation of papillary microcarcinoma seems to be superior to conventional surgery [9]; patient satisfaction related to QoL, and cost-effectiveness of thermoablative procedures as reasons favouring the application of local ablation for thyroid nodules are more than ever highly disputed among endocrinologists, surgeons, radiotherapists and radiologists.
We intended to analyze our experience in microwave ablation of thyroid nodules with regard to the results achieved from a patient-centered point of view. We decided to use a cross-sectional study to receive the perception of our patients in combination with objective data regarding the clinical and sonographic results. The aim of our investigation is to clarify whether the expected results of improved cosmetic outcome, successful treatment of the medical condition leading to the intervention and satisfaction of the patients with the outcome are confirmed in our patients.
Patients and methods
We designed a questionnaire which was presented to the majority of patients within the second year after the procedure. The questionnaire contains the items shown in Table 1. Due to the comparably small proportion of patients who were repeatedly examined, we refrained from an intraindividual comparison of sequential evaluations. Only the most recent record was incorporated into the analysis. The interview was conducted with patients either physically present for a regular follow-up or by phone.
Questionnaire for follow-up of patients after thyroid ablation
Questionnaire for follow-up of patients after thyroid ablation

Indications were chosen according to generally accepted international guidelines [6, 10] and patient preferences. Preoperative laboratory values were obtained within one week prior to the procedure. Exclusion criteria were thrombocyte count
Preoperative diagnosis was established using clinical examination,
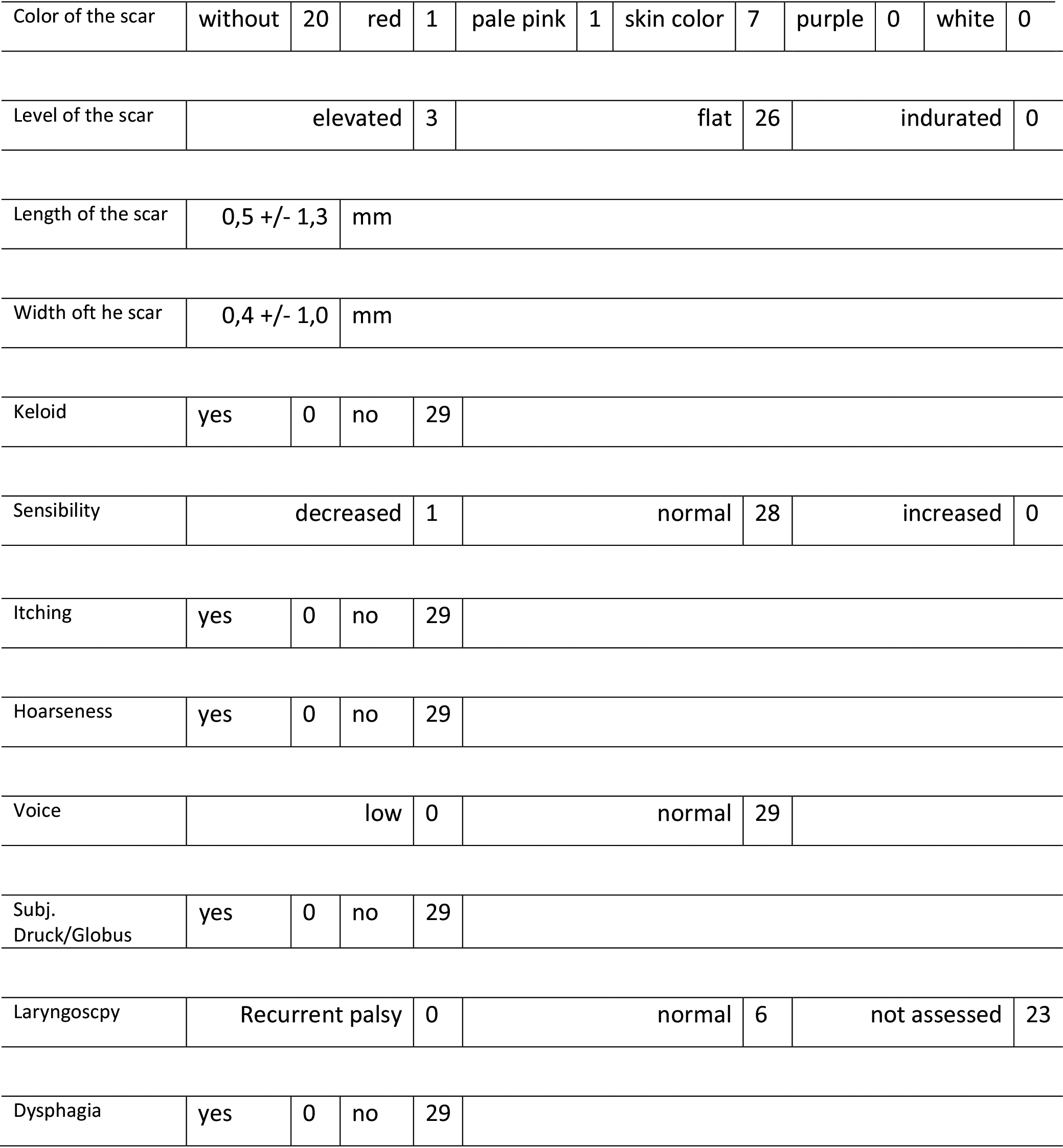
Results of standardized interviews with 29 patients after thyroid ablation
Intraoperative setting of thyroid microwave ablation. 1: Left hand with ultrasound transducer, 2: right hand with (flexible) microwave antenna.
The procedures were performed as outpatient treatments except for the first 9 patients, who postoperatively stayed overnight in the hospital. Follow-up included ultrasound, laboratory parameters and a clinical examination after 3, 6 and 12 months and annually thereafter. The standardized questionnaire was requested within two years after the procedure. The data were anonymized and the staff was blinded with regard to the identity of the patients. The results are presented as a descriptive analysis with mean
The patient population encompasses 30 patients. Gender was female in 21 and male in 9 cases. The average age was 54
In the average, 1.96
Eleven patients were physically present at the interview, 19 were interviewed during a telephone call. The interview took place 16 months after the treatment in the average. Results of the questionnaire are displayed in Table 2. As a summary, the four categories “cosmetic outcome” with five items, “neurological complaints” with two items, “vocal changes” with three items, and “pharyngeal symptoms” with two items were analyzed. The cosmetic outcome was particularly satisfying with 21 virtually invisible scars and only 2 patients reporting on reddish or pink color of the former needle entry. Scar formation with elevation of the puncture site occurred in three cases; no keloid was detected. The average size of a scar was half a mm unless no scar was present at all. Apart from one patient with decreased sensibility, none suffered from neurological complaints. In the long term, no vocal changes were present. Only 6 patients deliberately underwent postoperative laryngoscopy in spite of advice of doing so. No case of recurrent palsy was detected (0%).
Discussion
Thermal ablation is an accepted treatment for several benign indications, also autonomous nodules [12]. We found in all cases a trend towards normalized thyroid function, which means highly effective treatment. At the end of the follow-up period, none of our patients are reliant on any drugs focusing on thyroid function. Actual research shows no significant difference in treatment success comparing MWA and radioiodine therapy, whereas MWA leads to significantly less hypothyreodism [13].
MWA has some theoretical advantages in comparison to RFA, though RFA is at date the more popular and more frequently applied technique. MWA is faster, creates larger ablations areas and achieves higher temperatures. In our own results, the duration of the procedures was an average 26 minutes, while the average nodule size was large with 48.5 mm. Energy deployment was in the average 1.96 kJ per mL volume of nodular tissue, which resemble results of Korkusuz et al., who found an average of 1,5 kJ sufficient for 1 mL volume reduction [14]. An Italian group of researchers tried to discern different ultrasound features in order to predict the success of radiofrequency ablation [15]. They identified the three categories solid, cystic and spongiform to influence upon the energy required for shrinking the nodule, with slightly different amounts of energy when compared to the earlier findings. In our own experience, no ultrasound feature, but rather the functional status of the target tissue appears to be crucial for the energy input.
In light of the report of a rare but serious adverse event of ruptured nodules following MWA [16], it appears an advice to be reckoned with to control the energy deployed in each moment of the ablation process. The system we use offers the opportunity to record temperature as well as the amount of energy deployed into the tissue. As a disadvantage, the non-cooled shaft is believed to impose a risk of skin burns. None of our patients suffered from skin burns, however, whereas a skin burn was recently reported following RFA of a benign thyroid nodule [17]. In a recently published meta-analysis, no differences were found comparing RFA to MWA regarding safety and efficacy of the procedure [18]. In the absence of level 1 evidence, He et al. carried out an ambitious network meta-analysis comparing different thyroid ablation modalities [19]. They found two treatment sessions with RFA most effective, however, MWA was not included in their analysis.
Quality of life after thyroid ablation is considered comparably high, if a generic PROM (SF-36) is regarded [20]. Using a disease-specific PROM (the THYCA-QoL) among others, factors leading to inferior physical and mental conditions include neuromuscular disorders and symptoms of the throat and mouth [21]. We found apparently scarce such symptoms in our patient population, indicating minimal impairment of QoL in our cohort of patients. In comparison to conventional surgery, patient recorded outcomes of thermal ablation are frequently superior regarding pain (5% vs. 100%), rate of complications (5% vs. 14%) and post-procedural hypothyreoidism (0% vs. 23%) [22]. In a randomized controlled trial, postoperative quality of life and patient satisfaction was superior after thyroid thermal ablation in comparison to conventional thyroidectomy [23].
Conclusion
Our results confirm the impression of overall satisfaction of our patients with the treatment and the choice of this method; we were even able to complement additional data which conform to the expectations of excellent cosmetic results. Bernardi et al. report on a similar study focusing on a comparison of RFA to surgery. They found 92% of the RFA patients satisfied with the cosmetic result [24]. In this paper, not more than four items have altogether been interrogated, only one of them requesting “satisfaction with the cosmetic result”. In contrast, our own database provides information on 11 items, five of them related to the cosmetic result, confirming high patient satisfaction and confidence as well as reassurance for thyroid ablation.
So far, no sufficient data are available to enable a sound comparison of surgery to ablation for benign thyroid nodules. Only one randomized controlled trial has been published so far albeit much concern has been raised for methodological shortcomings of the study [25]. In a large meta-analysis consisting in one randomized controlled trial and six cohort studies, thyroid ablation turned out to be superior in terms of incidence of hoarseness, hypothyreoidism and postoperative pain [26]. We did not intend to compare our patients to a comparative cohort of patients undergoing surgery. Besides that, our data might suffer from a certain degree of bias, since the patients we treated were highly selected. In addition, we performed no longitudinal observation, and the time point for the interview with the patient was not standardized. Further investigation will be required to clear the ambiguity, which patients will benefit from undergoing thyroid ablation rather than surgery.
Footnotes
Conflict of interest
None to report.