
Abstract
BACKGROUND:
Although tibial shaft fractures are the third most common long bone fractures in children after the forearm and femur, nonunion of these fractures are rare in the pediatric population.
CASE REPORT:
Despite seldom seen, tibial nonunion is very complex and it is also a devastating complication of tibial fracture especially when infected. Numerous methods have been employed to treat pediatric tibial nonunion, but there is no consensus. Here, we present a case of a child with right tibial shaft fracture nonunion. We treated this patient with ipsilateral free non-vascularized fibular graft.
RESULTS:
Both the nonunion site and fibular donor site united well with good function in the injured extremity and no adverse events.
CONCLUSION:
We recommend the use of ipsilateral free non-vascularized fibular graft for the treatment of pediatric tibial shaft nonunion.
Introduction
Pediatric tibial shaft fractures represent 13% of all pediatric fractures, which will heal uneventfully with adequate treatment and nonunion occurs rarely [1]. Nonunion is disastrous for children because of the impact on the quality of life. Despite the rarity, tibial nonunion is very complex and it is also a devastating complication of tibial fracture especially when infected [2]. Numerous approaches have been proposed for the treatment of pediatric tibial nonunion including bone allografts, bone autografts, Masquelet’s induced membrane technique and Ilizarov technique [3]. In daily practice, cancellous bone graft is a popular technique but limited to bone defects less than 4 cm in length [4]. Autologous iliac grafting is the most preferred method of bone grafting in adults but the bone quantity harvested from the ilium is limited in children and also poses additional injury. Biological bone substitutes and bone allografts are alternatives although they have only osteoconduction without osteoinductive properties [5]. Masquelet and Ilizarov techniques are much more suitable for large bone defects but they are associated with a high cost and long duration of treatment. To resolve these limitations, we use ipsilateral free non-vascularized fibular graft to treat pediatric tibial shaft nonunion and we achieved a satisfactory outcome. Here, we present a case of pediatric tibial shaft nonunion treated with this technique.
Case presentation
A 2-year-old girl was brought to the hospital after sustaining an open right tibial shaft fracture following a car accident. Emergency irrigation, debridement and temporary external fixation was performed at a local hospital. Four months later, the patient was brought to our clinic for consultation. X-rays were taken and showed no callus at the fracture site so the external fixator was removed and the limb was immobilized with cast. Two months later, the patient returned for a follow-up and check X-rays showed no callus at the fracture site (Fig. 1A–B). Hence, a diagnosis of a right tibial shaft atrophic nonunion was reached.
A–B: AP and lateral radiograph showing a right-side tibial shaft atrophic nonunion. C–D: AP and lateral radiographs taken postoperatively showing good fracture reduction and fixation with enough bone graft.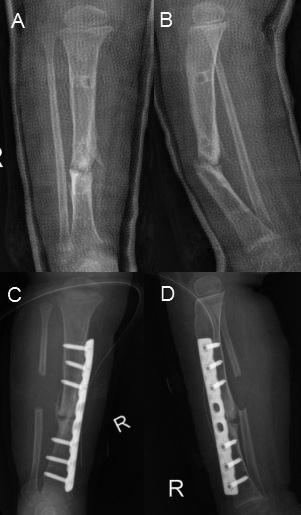
After discussing the family with the treatment options available, a decision was made to perform an ipsilateral free non-vascularized fibular graft. The procedure involves four key steps: 1) Harvesting an ipsilateral free non-vascularized fibula graft: utilizing the standard lateral approach of the leg, the incision center was at the same level of the tibial fracture center, the fibula was accessed while protecting the fibular periosteum then a 2–3 cm fibular segment was harvested using a drill and finally the harvested fibular segment was kept in gauze soaked with saline. 2) Reduction and fixation: using the standard anterior approach of the leg, the nonunion site was visualized then debrided the fibrous scar tissue and ossified tissues and reamed the medullary cavity while preserving the tibial periosteum and blood supply. Then, the fracture site was reduced and the correct length and alignment of the leg was achieved which then fixed with anatomic LCP (Locking Compression Plate). 3) Bone grafting: the fibular segment was cut into several small pieces and packed into the bone defect site. 4) The final step of the procedure is to put a drainage and close the incision. Drainage tube was removed 24 hours and stitches were removed 12 days postoperatively. Follow-up and check X-rays were done monthly.
Postoperative radiographs showed good fracture reduction and fixation with adequate bone graft (Fig. 1C–D). At 3-month follow-up, radiographs revealed that the tibial fracture site and the fibular bone defect site united with abundant callus formation across the fracture site and absence of a fracture line (Fig. 2A–B). So the plate was removed and the patient was followed up for further 2 months (Fig. 2C–D). The patient regained the normal function in the injured extremity at 3-year follow-up. Currently the child is admitted to a primary school, enjoying outdoor playing and daily routine activities with no pain and normal limb alignment at 5-year follow-up.
A–B: At the 3-month follow-up, radiography revealed tibial fracture and fibular bone defect union with abundant callus formation across the fracture site and absence of a fracture line. C–D: AP and lateral radiographs taken 2 months after the palte removal showing good fracture union.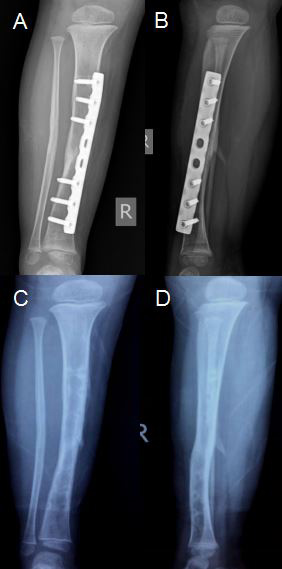
Nonunion of pediatric fractures occur rarely due to the local biological factors [6]. The overall rate of nonunion in pediatric patients is less than 2% [7]. But when a posttraumatic problem occurs, it will bring challenges to surgeons because of the complex biological context [8]. Literature shows that nonunion of pediatric fractures are commonly related to open fractures, comminuted fractures, bone defects, soft-tissue loss, infection, suboptimal immobilization or external fixation [9]. Glass GE et al. reported that Gustilo IIIB paediatric tibial fractures has delayed union rate of 22% and a nonunion rate of 13% [10].
There are numerous treatment strategies available including protected weight bearing, bone stimulators, revision of fixation and plating with bone grafting [11]. Bone grafting is widely accepted as an effective method while surgeons have to make a choice between allografts and autografts. Because the allografts have only osteoconductive capability but has no osteoinduction; bone autografts are the first choice for most surgeons. Vascularized fibular and iliac grafts are the most popular autografts, vascularized fibula grafts are mainly indicated for large bony defects and demands rich surgical experience and high requirement for vascular surgery techniques [12]. Iliac grafting is suitable for adult bone defects but in children, the bone quantity grafted from this site is limited and it also needs an incision which will leave a big scar on the iliac region. To solve this limitation, we devised a novel technique using ipsilateral free non-vascularized fibular graft. This technique harvests bone graft from the closest site of the defect thus no new scar will develop in other body parts. The harvested bone has the advantage and function of osteoinduction and osteoconduction. During the procedure, the periosteum is preserved so the fibula can regenerate. Some surgeons criticize fibular autografts due to donor site morbidities observed in previous study findings but most of the references are anatomic or adult studies [13]. Only a few studies are about pediatric population and the technique used is vascularized fibular graft [14]. Anil Agarwal et al. reported that non-vascularized fibula grafting with periosteal preservation has a lower morbidity rate and most of the cases achieve fibular regeneration as early as six months with no clinical implications [15]. This technique has been used successfully for our case with good outcome and no adverse events. Both the fracture nonunion site and the fibular donor site united and healed well. Based on our clinical experience, the technique warrants widespread use.
Conclusion
We recommend the use of ipsilateral free non-vascularized fibular graft for the treatment of pediatric tibial shaft nonunion.
Ethics statement
The Institutional Review Board of Xinjiang Medical University approved the publication of this case report and informed consent has been obtained from the patient’s parents.
Funding
This project was supported by the Jilin Science and Technology Development Project (No. 20200201484JC).
Footnotes
Conflict of interest
The authors report no conflict of interest.