
Abstract
BACKGROUND:
The incidence of conversion total hip arthroplasty (cTHA) following reduction and fixation for proximal femur fractures will increase in parallel to the aging population worldwide.
OBJECTIVE:
The goal of this study is to report the frequency of bacterial detection and the outcome of cTHA at the authors’ institution and to analyze preoperative factors that correlate with higher rates of bacterial growth and septic revision.
METHODS:
48 patients who had been converted to THA after osteosynthesis of a proximal femur fracture either by a one- or two-stage procedure were included. Septic failure rate and the frequency of bacterial detection at the time of fixation device removal were calculated. The influence of different preoperative factors was examined by the odds ratio. A receiver operating characteristic curve of c-reactive protein (CRP) for detection of bacterial growth at the time of fixation device removal was calculated.
RESULTS:
18.8% patients showed positive bacterial cultures, with Staph. epidermidis being the most frequent pathogen (33.3%). Septic failure after cTHA occurred in 4.2%. Fixation with cephalomedullary nails and complications with the internal fixation showed higher odds for bacterial growth at time of cTHA. CRP for predicting bacterial growth had an area under the curve of 0.661. Implant survival was worse when temporary spacers were used.
CONCLUSION:
Bacterial detection rate at the time of cTHA is high, whereas septic failure rates are low. Isolated evaluation of inflammatory blood markers without other diagnostic modalities for infection is not decisive and does not justify a two-stage approach with implantation of a temporary spacer.
Background
The incidence of conversion total hip arthroplasty (cTHA) following reduction and fixation for proximal femur fractures will increase in parallel to the aging population worldwide [1, 2]. Usually, osteosynthesis of proximal femur fractures is successful, but complications such as non-union, secondary avascular necrosis (AVN) of the femoral head, cutting out and secondary arthritis of the hip can compromise medium- and long-term outcomes [3, 4, 5]. In these cases, cTHA offers improvement of function and reduction of pain [4]. However, cTHA is characterized by elevated rates of intra- and postoperative complications, with periprosthetic joint infection (PJI) being one of the leading causes for revision in up to 6% [6, 7, 8, 9]. PJI is a devastating complication after THA with a high socioeconomic burden and a reported mortality rate of 25.9% after 5 years [10, 11]. As there are data pointing to rates of bacterial colonization of orthopedic internal fixation devices as high as 53% [12], performing cTHA as a two-stage procedure on principle could be considered. However, when compared to one-stage procedures this revision strategy is associated with specific disadvantages, such as increased overall operating time, greater blood loss and increased morbidity and mortality rates [13, 14]. Little information can be found in the literature indicating whether a staged approach in cTHA reduces the rate of PJI and, if so, in which patient population the two-stage procedure is favorable. The aim of this retrospective study was (I) to report the frequency of bacterial detection as well as the outcome of cTHA and (II) to describe preoperative factors that correlate with higher rates of bacterial growth and septic revision after cTHA. Furthermore (III), a comparison of one-stage and two-stage approaches for cTHA was performed.
Patients and methods
For this retrospective cohort study, all patients aged 50 years and older at the authors’ institution who had undergone removal of internal fixation devices at the proximal femur between January 2010 and December 2018 were identified (
The mean age was 72 years (50–91). There were 37 women (77.1%) and 11 men (22.9%). Concerning the preoperative health status, the ASA score was used for perioperative risk estimation: 2.1% were rated ASA 1, 47.9% ASA 2, 47.9% ASA 3 and 2.1% ASA 4. The mean number of relevant comorbidities necessitating permanent medication was 5 (1–8). The indication for conversion was secondary arthritis in 24 patients (50.0%) and failed osteosynthesis by means of non-union, AVN or cutting out in the remaining 24 patients (50.0%). Table 1 provides an overview of the indications for cTHA and the type of removed fixation device.
Removed devices and indication for cTHA
Removed devices and indication for cTHA
The mean time between osteosynthesis and removal of the fixation device was 23 months (1–221). cTHA was performed in 23 patients (47.9%) by osteosynthesis removal and THA in a one-stage procedure. The other 25 patients (52.1%) underwent a two-stage procedure either with (
Complication rate, bacterial detection rate at the time of conversion surgery and the need of revision surgery were documented.
Statistical analysis was performed using the statistical software package SPSS 25 (IBM, Armonk, NY, USA). Descriptive statistics were reported as mean and range. The odds ratio (OR) was calculated for determining the effect of preoperative factors on the occurrence of bacterial detection and revision surgery. The distribution of events between groups was compared by using the Chi-Square test or the Fisher-Exact test A Receiver Operator Characteristic (ROC) Curve was calculated for the predictive value of CRP for bacterial growth. Implant survival was calculated by Kaplan-Meier estimate and LogRank test was used to determine whether implant survival differed significantly The level of significance was set at
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of the University of Wuerzburg (protocol code 2020050503, date of approval 16.06.2020).
Bacterial detection rate
Bacterial growth from intraoperative tissue sampling was detected in 9 patients (18.8%).
Three cases (13.0%) of bacterial growth were recorded in patients undergoing one-stage cTHA. These patients were treated as a Tsukayama Type I infection and received 6 to 12 weeks antibiotic therapy as recommended by antimicrobial stewardship.
One case of bacterial growth (Corynebacterium tuberculostearicum) was recognized in a patient who had undergone two-stage cTHA without a spacer. Antibiotic therapy was not administered as contamination was suspected.
Five cases of bacterial growth were noticed at stage one of two-stage cTHA with spacer. During stage two, there was no more evidence of bacteria in these 5 cases.
Periprosthetic joint infection
Two patients (4.2%) underwent consecutive revision surgery during the first 18 months after cTHA because of PJI. In both patients, bacteria species isolated at the time of conversion and at the time of revision THA were not the same.
In the first case, a 75-year-old woman had developed a non-union after intertrochanteric fracture treated by CMN. Due to suspected infection, a two-stage procedure with temporary spacer implantation was performed. The samples taken during the CMN removal showed evidence of Staphylococcus aureus. 58 days after spacer implantation cTHA was performed showing sterile cultures. 18 months later the patient was revised for PJI showing Staphylococcus epidermidis and Streptococcus anginosus being the responsible pathogens for PJI. The patient developed a chronic PJI treated by permanent fistula as salvage procedure.
In the second case, a 76-year-old woman suffered from non-union after CMN as well. Again, a two-stage procedure with spacer implantation was performed. Specimens taken during CMN removal showed growth of Staphylococcus epidermidis. Removal of the spacer and cTHA were performed 63 days later revealing sterile cultures from intraoperative samples. 5 months later the patient was revised for PJI by debridement, lavage and exchange of mobile parts. Streptococcus agalactiae was cultured from intraoperative samples. The infection was treated successfully by the mentioned surgical intervention and antibiotics for 12 weeks.
Other orthopedic complications
One patient, suffering from postoperative dislocation (2.1%), was treated successfully by closed reduction. There were no cases of periprosthetic fractures or aseptic loosening.
Preoperative factors
Fixation device
Concerning the sort of fixation device used, all septic failures after THA occurred in patients treated with CMNs. This was also the group with the highest bacterial detection rate of 20.6% as shown in Table 2. Comparing CMNs with other fixation devices, the OR for bacterial growth was 1.6 (
Summary of bacterial species isolated from intraoperative samples for different fixation devices
Summary of bacterial species isolated from intraoperative samples for different fixation devices
CNS: Coagulase negative Staphylococci.
Table 3 demonstrates the bacteria species isolated and the growth rate for different diagnoses leading to cTHA.
Summary of bacteria species isolated from intraoperative tissue samples
Summary of bacteria species isolated from intraoperative tissue samples
CNS: Coagulase negative Staphylococci.
The OR for bacterial growth was 4.5 when comparing cases of non-union, AVN or cutting out with cases of secondary arthritis (
The mean CRP level prior to surgery was 1.4 mg/dl (0–23.9 mg/dl). Elevated levels were measured in 15 cases (31.9%, 1.1–23.9 mg/dl) of which 4 revealed bacterial growth at the time of internal fixation device removal and of which 2 were revised for PJI.
The mean ESR was 23 mm/hr (1–132 mm/hr). Elevated levels were measured in 23 cases (47.9%, 16–132 mm/hr) of which 5 revealed bacterial growth at the time of internal fixation device removal and of which 1 was revised for PJI.
The mean WBC count was 7.700/
In only 3 patients all 3 blood markers were elevated. None of them developed PJI and only 1 showed bacterial growth.
Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for bacterial growth at time of fixation device removal stratified for CRP
Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for bacterial growth at time of fixation device removal stratified for CRP
Table 4 displays the PPV for bacterial growth at the time of internal fixation device removal for different CRP levels.
However, at the standard cut-off level of 0.8 mg/dl sensitivity was 33.3%, specificity 66.7%, PPV 18.8% and NPV 81.3%, revealing a high rate of false positives. Combining all 3 blood markers did not improve the meaningfulness substantially leading to a sensitivity of 11.1%, a specificity of 94.8%, a PPV of 33.3% and a NPV of 82.2%.
The ROC-curve in Fig. 1 illustrates the poor value of CRP for predicting bacterial growth, with an area under the curve of 0.661. For predicting septic failure, calculating a ROC curve was statistically not reasonable.
Patients combining all 3 factors (CMN, complication with the internal fixation, elevated CRP) (
Odds ratio of bacterial growth and PJI for preoperative risk factors
Odds ratio of bacterial growth and PJI for preoperative risk factors
n.p.
ROC-curve of CRP for bacterial growth at time of fixation device removal.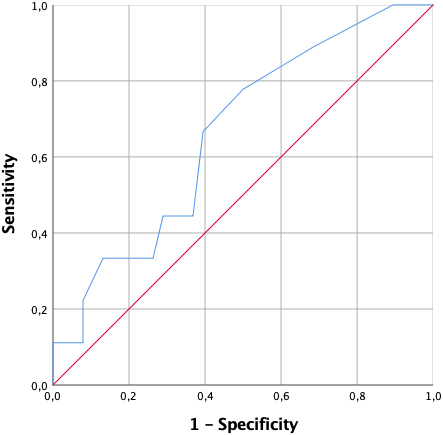
In Table 5, the OR for PJI and bacterial growth for all possible combinations of the three examined preoperative factors are shown.
Implant survival in patients treated with spacer was significantly worse than in patients treated without spacer (LogRank test,
Kaplan-Meier curves for implant survival (red 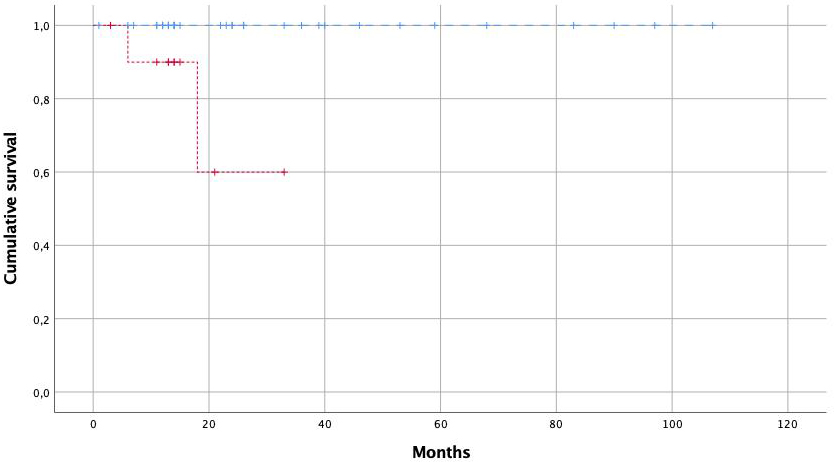
Compared to primary THA, cTHA after fractures of the proximal femur is associated with higher complication rates, with PJI being one of the most feared complications [6, 9, 16]. Smith et al., for example, recently analyzed 369 patients from the Medicare data base and confirmed higher rates of infection for cTHA after CMN compared to patients with primary THA (6.2% and 2.6%) [9]. In the current study, we observed a comparable infection rate of 4.2%. Other orthopedic complications were rare in our cohort in contrast to previously reported high rates of dislocation, periprosthetic fracture and others. This might be due to the small sample size. Another explanation might be the high expertise concerning revision hip surgery at our institution.
The aim of preoperative testing must be to identify the patients at high risk for septic failure after cTHA. Thus, the diagnostic tests used are required to have a high PPV. So far, next to clinical findings such as purulence or a sinus tract, CRP is the standard preoperative parameter indicative of infection. It is considered a minor criterion for definition of PJI by the consensus meeting of the Musculoskeletal Infection Society [17]. In the current study, even with a more than 7-fold elevated CRP, a PPV for bacterial isolation of only 50% was achieved. This insufficient ability of elevated CRP levels to predict bacterial isolation is in accordance with previously published studies. Cichos et al. determined the value of serological screening prior to cTHA [18]. They stated that an optimal cut-off level for CRP of 1.2 mg/dl would yield a PPV of only 43%. Klatte et al. calculated a PPV of only 4% at a cut-off level of 0.5 mg/dl [19]. CRP levels are most helpful when they are within the normal range, but less meaningful when they are only slightly to moderately elevated. Thus, especially elevated CRP levels alone do not seem suitable to decide whether a two-stage cTHA should be performed or not because of high rates of false-positives. Even though often recommended, combining CRP with WBC count and ESR did not improve the sensitivity and PPV of the testing substantially in this study while providing a comparable high NPV.
We were able to identify some preoperative factors correlating with higher rates of bacterial growth and PJI, namely elevated CRP levels, CMN used at time of osteosynthesis and complications with the internal fixation rather than secondary arthritis leading to cTHA. Other authors [16, 20] have shown CMN to be critical in cTHA concerning complication rates and perioperative morbidity. This might be due to the reaming of the intramedullary canal and the size of the implant. Another explanation might be the difficulty of removing a CMN during cTHA leading to significantly increased blood loss, operating time and soft tissue damage as shown by Bercik and colleagues [20]. Complications such as cutting out, AVN and non-union might in some cases be caused by bacterial infection and therefore lead to higher rates of PJI after cTHA. As discussed for CRP, none of these risk factors alone should be decisive in determining the surgical strategy. But patients in our cohort who combined all three risk factors had to be revised for PJI in nearly one third of the cases whereas patients without any of these risk factors showed neither bacterial growth nor PJI. Whether a two-stage procedure with temporary spacer would be able to reduce the rate of PJI in this group cannot be answered by our data and requires further studies.
So far, it is not clear whether PJI after conversion arthroplasty is due to bacterial colonization during osteosynthesis or due to bacterial colonization during or after conversion arthroplasty. On the one hand, cTHA is highly complex, with increased blood loss and longer operating time when compared to primary THA [21, 22, 23]. Furthermore, the patient population requiring cTHA is often highly comorbid as can be confirmed by the present study including nearly 50% patients rated ASA 3 and ASA 4. Schwarzkopf et al. and Baghoolizadeh and co-workers emphasized that cTHA should be considered much more as revision THA than as primary THA leading to more complications and poorer outcomes [7, 24]. On the other hand, there are data reporting bacterial colonization of retrieved fixation devices in 53% [12]. Dobbins et al. even found a rate of 77% positive bacterial cultures which were obtained by scraping removed fixation devices, whereby in most cases Staphylococcus epidermidis was isolated [25]. Of note, patients in these studies did not show any clinical signs of a relevant infection. In our study, Staphylococcus epidermidis was the most isolated strain as well. However, the clinical relevance of isolating these bacteria without any clinical signs of infection remains unclear. In our cohort 9 patients revealed positive bacterial cultures at the time of removal of the fixation device, but only 2 patients suffered from PJI. Furthermore these 2 patients showed different bacterial strains at the time of revision for PJI compared to the time of removal of the fixation device. Even though there might be confounders like the antibiotic therapy administered after cTHA, our results nevertheless indicate that the procedure itself might be the source of infection and not the (possibly existing) bacterial colonization of the removed fixation devices – as also previously suspected by Klatte and colleagues [26]. Taking this into consideration, a two-stage procedure might even increase the risk for PJI rather than being the “safe option”. Possibly conforming to this argumentation, both cases of PJI in our cohort occurred after a two-stage procedure with temporary spacer.
Furthermore, even if the surgeon is surprised by not expected positive bacterial cultures at the time of one-stage cTHA, the situation can be dealt with sufficiently as a Tsukayama type I infection, with the promising option of antibiotic treatment [27]. Additionally, considering that two-stage procedures with a spacer have a reported 90-day-mortality of up to 4%, the indication should be reserved for cases of clinically evident peri-implant infections [28].
Two aspects for the treatment strategy of cTHA need to be balanced: The socioeconomic burden, morbidity and mortality of spacer implantation and the likelihood and difficulties of infection determination and eradication after internal fixation of proximal femur fractures. Certainly, there are circumstances, such as acute, clinically obvious infections in which spacer treatment is reasonable. However, based on our results, the indication for spacer treatment because of assumed low-grade infection does not seem to be justified.
Besides the retrospective design the small sample size is the strongest limitation of this study mostly leading to missing statistical significance when comparing groups. Multicenter studies are required for gaining sufficient sample sizes. Furthermore, selection bias may have occurred as the indication for the variable treatment strategies including one-stage as well as two-stage cTHA with and without spacer implantation was not standardized. Although we present data with a mean follow-up of 28 months, 14.6% of the included patients could not be followed for at least one year, thereby hampering compelling conclusions.
Conclusion
Bacterial presence at cTHA is high, whereas septic failure rates are low. Isolated evaluation of inflammatory blood markers without other signs of infection does not justify a two-stage approach with implantation of a temporary spacer. Missing elevation of inflammatory markers on the other hand is highly predictive of sterile intraoperative tissue samples. However, in patients additionally displaying implant failure after intramedullary nailing, such as cutting out or non-union, a two-stage procedure can be considered as rates of bacterial presence and PJI are high in this subgroup. Still, it remains uncertain whether spacer implantation can reduce the risk of PJI in these cases.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This research did not receive any specific funding. The publication was supported by the Open Access Publication Fund of the University of Wuerzburg.