Intraoperative lung-protective ventilation adjusting tidal volume to a plateau pressure restriction in elderly patients: A randomized controlled clinical trial
Available accessResearch articleFirst published online March, 2023
Intraoperative lung-protective ventilation adjusting tidal volume to a plateau pressure restriction in elderly patients: A randomized controlled clinical trial
Lung-protective ventilation (LPV) strategies have been considered as best practice in the care of critically patients.
OBJECTIVE:
This study aimed to investigate the effects individualized perioperative LPV with a positive end-expiratory pressure (PEEP) and low tidal volumes () based on a target airway plateau pressure (Pplat) in patients during and after an operation compared with conventional ventilation in elderly patients during abdominal surgery.
METHODS:
Sixty-one elderly patients with American Society of Anesthesiologists (ASA) I to III undergoing open abdominal surgery received either conventional ventilation (8 ml/kg; CV group) or LPV ( was adjusted to a target Pplat [ 20 cm HO]) in the volume-controlled mode with PEEP (9 cm HO; LPV group) ventilation.
RESULTS:
Patients in the LPV group showed significantly lower pH values (7.30 0.07 vs. 7.38 0.05, 0.001) and respiratory indexes than that of CV group (0.806 0.339 vs. 0.919 0.300, 0.043) at the end of surgery. Compared with the CV group, the dynamic lung compliance (33.39 3.163 vs. 30.15 2.572, 0.001) was significantly higher, and the body temperature remained significantly more favorable in the LPV group (35.9 0.3 vs. 35.1 0.4, 0.001). Patients in the LPV group had significantly faster postoperative recovery than that of the CV group ( 0.001).
CONCLUSIONS:
The study showed that LPV could be beneficial for ventilation, core body temperature, and postoperative recovery in elderly patients with healthy lungs.
Lung-protective ventilation (LPV) strategies have been considered as best practice in the care of critically patients. The benefits of strategies with low tidal volume () and positive end-expiratory pressure (PEEP) were associated with improved clinical outcomes and reduced health utilization [1]. However, some observational studies has reported contradictory results, suggesting that the use of higher PEEP levels mainly inducing airway distention rather than improved alveolar ventilation in patients with healthy lungs [2, 3]. Therefore, the calculations of based on predicted body weight (PBW) undoubtedly highlights the different status of the lungs as an unreasonable factor for the optimization of protective mechanical ventilation (MV) [4].
Previous studies have shown that MV with lower driving pressure (DP) is crucial for benefits of the three main components of LPV, including , plateau pressure (Pplat), and PEEP in patients with acute respiratory distress syndrome (ARDS) (DP is the difference between the Pplat and PEEP) [5, 6]. However, considering the different variables and their values of , Pplat, and PEEP and the LPV theory of high Pplat with high PEEP or low with high Pplat in normal lungs during surgery, introducing a dynamic control setting, such as the relationship between PEEP and , may be more feasible, direct, and easy to observe [7, 8].
We hypothesized that a limited Pplat could be useful for guiding low selection together with PEEP as a lung protection ventilation technique that prevents alveolar hypoventilation. To test our hypothesis, we investigated the specific effect of a prophylactic LPV with a continuous PEEP and an individualized on the target level of Pplat and determined whether these parameters could be beneficial for elderly patients during abdominal surgery compared with CV of 8 ml/kg of PBW without PEEP.
Methods
Study design
This was a single-center, randomized clinical trial performed at the Third Affiliated Hospital of Anhui Medical University, China. Patients were enrolled from November 2015 to October 2017. The study was approved by the Ethics Committee of the Third Affiliated Hospital of Anhui Medical University for Human Studies (ethical committee number HFYY 2015016) in September 2015, and written informed consent was obtained from all patients. The study was registered in the Chinese Clinical Trial Registry (no. ChiCTR 1800014578). The study protocol complied with the 1975 Declaration of Helsinki.
Patient and public involvement
Patients were randomly assigned to study group or control group by automatic number. People who had access to the randomization information were not involved with any experimental trial procedure. Patients in this trial were not involved in the design, recruitment, and conduction of the study. Once allocated to a group, the surveillance data of each patient was collected and collated, and personal data collected during the study was kept confidential and stored securely at the study site in a locked cabinet accessible only to the data analyst members. The results of this study were not disseminated directly to study participants.
Participants
Patients who met the following criteria were included: (I) older than 65 years; (II) of either sex; (III) with physical status I to III according to the American Society of Anesthesiologists; (IV) with normal preoperative pulmonary function; (V) scheduled for elective open abdominal surgery with an expected duration of general anesthesia between 1.5 and 3.0 hours. Patients who met the following criteria were excluded: (I) with a history of asthma or chronic obstructive lung diseases; (II) with bronchial infection in three weeks; (III) with sleep apnea syndrome; (IV) with a body mass index (BMI) 35 kg/m; (V) with a history of benzodiazepine use; (VI) with intracranial hypertension; (VII) lack of cooperative or cognitive learning; (VIII) with uncontrolled severe hypertension and cardiovascular diseases; (IV) with liver or kidney dysfunction; history of second- or third-degree heart block or ischemic heart diseases; (X) who were unable to maintain an appropriate peripheral oxygen saturation by pulse oximetry (SpO), those presenting with anemia (hemoglobin 9 g/dL), or distorted anatomy of the tracheobronchial tree on chest radiographs.
Study protocol
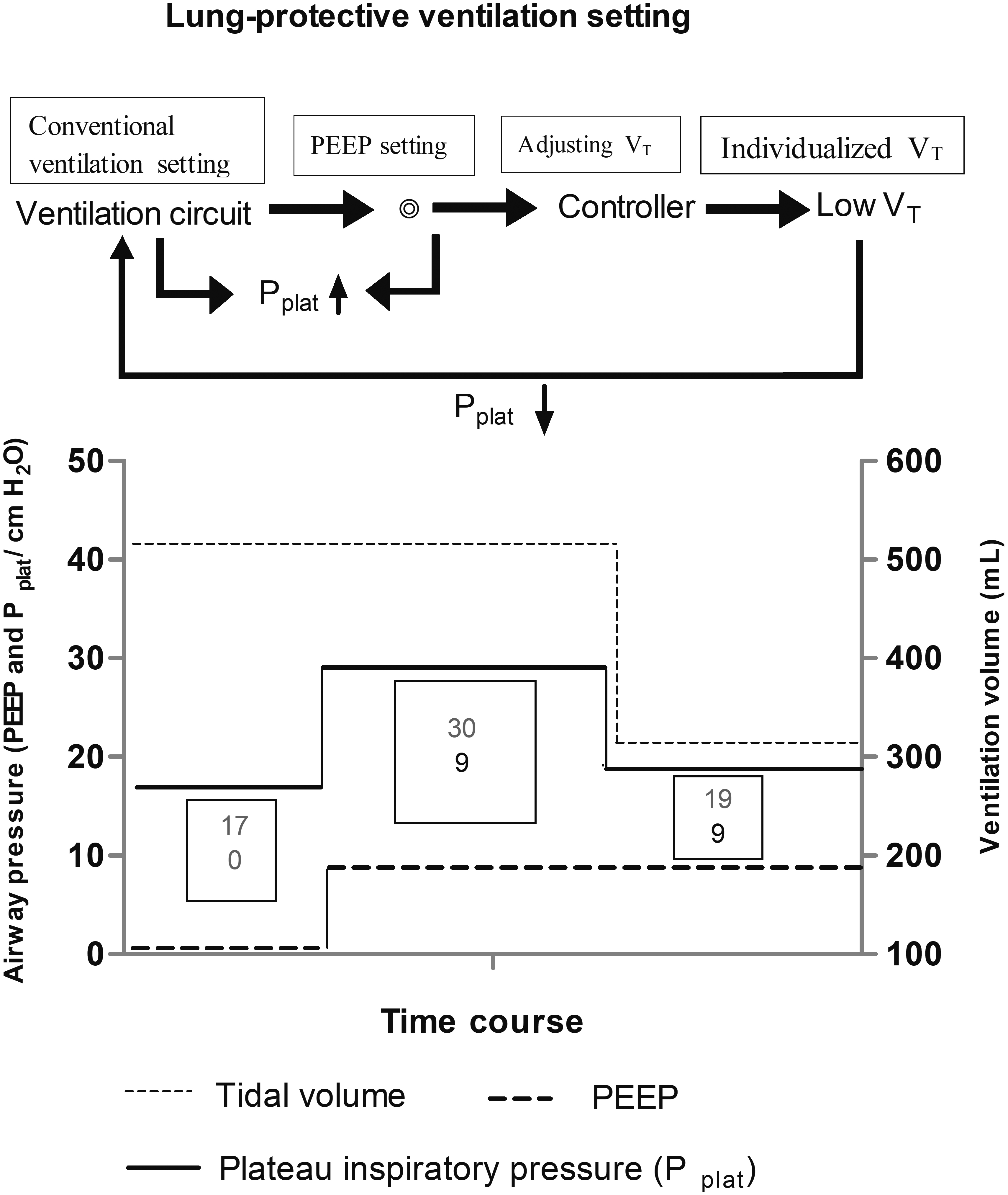
Patient randomization was accomplished through our Division of Biostatistics using a computerized random number generator. Group assignment was concealed in a sealed envelope until surgery began. All patients were anesthetized by an anesthetist responsible for the intraoperative patient care who did not participate in the investigation. An anesthetist resident collected the intraoperative data and was blinded to the study, and this process continued until the end. All patients were fully informed about the study and blinded to their groups. Patients were confirmed with inclusion or exclusion criteria and randomly divided into two groups: the conventional MV with of 8 ml/kg and no PEEP (CV group), and LPV with adjusting levels and 9 cm HO levels of PEEP (LPV group). However, the proper PEEP level was set as a variable based on a prior study in anesthetized patients [2]. For an initial period of five minutes after the start of surgery, PEEP was applied using the ventilator settings described below. Before starting the PEEP setting, arterial blood gases were measured. Concerning the LPV, the was determined in the following manner. The MV was started with an initial of 8 ml/kg with no PEEP for five minutes, and at this point, the airway Pplat remained relatively stable. Then, we set the PEEP at 9 cm HO, and the Pplat was elevated to a higher level than the previous PEEP setting. Based on this situation, we only needed to adjust the to obtain a decreased Pplat. adjustment was initiated five minutes after stabilized PEEP, and the was incrementally reduced with a manual adjusting knob approximately every two minutes until a targeted Pplat less than 20 cm HO was maintained as an expected criterion for individualized levels of LPV. However, LPV was established without repeated recruitment maneuvers, and stable levels of Pplat and were maintained during the study period. Figure 1 show the protocol procedure and incremental PEEP, Pplat, and decremental phases. However, the respiratory rate was regulated at any time according to arterial carbon dioxide partial pressure (PaCO), which was limited to a maximum of 8 kPa (60 mm Hg), again assuring pH values between 7.25 and 7.45 [9]. Additionally, the was readjusted according to the above method if the respiratory rate was modified for excessive PaCO and once Pplat changed.
Schematic representation of the study of the plateau pressure (Pplat), positive end-expiratory pressure (PEEP), and tidal volume () measurements. The pressure was increased stepwise from a PEEP of 0 cm HO and Pplat of 17 cm HO (further reported as PEEP/Pplat 0/17 cm HO) to 9/30 cm HO. Afterward, adjusting by reducing tidal volumes, Pplat was decreased stepwise from 30 cm HO to 20 cm HO, the and Pplat regulating were completed. At 9 cm HO of PEEP and Pplat 20 cm HO, an individualized mode was established.
Anesthesia, ventilation, and monitoring
All patients were brought to the operating room without premedication. Peripheral intravenous access was established with an infusion of 37C solution to maintain a positive daily fluid balance and an adequate urine output. After three minutes of administration of pure oxygen, general anesthesia was induced as a sequential anesthetic to facilitate tracheal intubation with an appropriate size tube, using F 28–30 in females and F 30–32 in males. Anesthesia was maintained with a target-controlled anesthetic infusion (TCI) (Sims Graseby Ltd., Watford, UK) and sevoflurane at 1%. A 4 mg bolus of cisatracurium was administered every 30 to 45 minutes according to clinical need.
The lungs were ventilated by adjusting the Datex Ohmeda Aspire 7100 Anesthesia Machine (GE Healthcare, Helsinki, Finland) in a volume-controlled ventilation mode with an inspired oxygen fraction (FiO) of 60%, and the ventilator delivered a square waveform flow with an inspiratory/expiratory (I/E) ratio of 1:2 and no PEEP. Ventilation was started without PEEP and Pplat between 14 and 20 cm HO. The respiratory rate was set at 12 breaths/min, and was maintained at 8 ml/kg. Following stabilization of the hemodynamic parameters after general anesthesia, the ventilation strategies were changed according to the group allocation described in Section 2.4.
Heart rate (HR), invasive systolic, diastolic, and mean arterial blood pressure (MAP), and SpO were measured by the Datex Ohmeda S/5 monitor (Datex-Ohmeda Division, Instrumentarium Corp., Helsinki, Finland) during the entire anesthesia period. A Narcotrend monitor (Narcotrend index: NI) was attached to each patient for continuous measurement to obtain the appropriate anesthesia depth, and the partial pressure of CO at the end of expiration (PetCO) was measured by introducing a capnography side stream sampler attached at the elbow between the endotracheal tube and the anesthesia circuit (D-Fend, E-CAiO-OO, GE Healthcare, Finland Oy Helsinki, Finland). The core body temperature (, C) was monitored continuously via a unilateral earhole using a novel temperature measuring instrument (Braun Ltd., IRT, Germany). Additionally, an indwelling bladder catheter was inserted, and the location of the endotracheal tube was further identified by fiberoptic bronchoscopy. The ambient temperature of the operating room was maintained at approximately 24C, which did not involve the other appropriate intraoperative warming method for each patient.
However, in the LPV group, the protocol was only started if patients were hemodynamically stable, characterized by two necessary conditions: a good intraoperative hemodynamic state (MAP 70 mmHg) and optimized oxygen saturation (SpO 95%). In the case of interruption because of hemodynamics or oxygen saturation concerns, the LPV was re-established after five minutes of stabilization. Intraoperative hypotension ( 20% decrease in baseline blood pressure) was treated with 10 mg intravenous ephedrine or 40 g phenylephrine, while bradycardia was treated with 0.5 mg intravenous atropine and/or aided lung expansion with positive pressure mask ventilation, applied whenever signals of hypoxemia plus abundant airway secretions were presented.
In both groups, following peritoneal cavity cleaning, the patients were administered 1 mg/kg of tramadol and 8 mg of ondansetron; the administration of sevoflurane was stopped, and the maintenance of anesthesia was supplemented by TCI with propofol, and remifentanil titrated according to clinical need. After incision closure, the administration of remifentanil and propofol was stopped. In the LPV group, at 10 minutes before the end of surgery, ventilation was switched to CV ( of 8 ml/kg without PEEP).
Perioperative measurements
MAP, HR, and NI were recorded at five time points: T1, 5 minutes after intubation; T2, just before the commencement of surgery following the stabilization of hemodynamic parameters; T3, 1 hour after the beginning of surgery; T4, 10 minutes before the end of surgery; T5, immediately after extubation. Intraoperative blood loss, liquid input, urine output, and MV and surgery duration were also recorded.
Intraoperative Pplat and were monitored continuously and recorded at T1, T2, and T4. These values were used to calculate the overall percentage of the decreases in and Pplat.
SpO, PetCO, and (C) were recorded at T2 and T4. At this time, arterial blood gas was analyzed at T2 and T4, and arterial oxygen partial pressure (PaO) and pH were determined using an ABI-30 analyzer (Radiometer, Copenhagen, DEN).
The dynamic lung compliance (CLdyn) of the respiratory system was calculated using the following standard formula: CLdyn /peak airway pressure (Paw) – PEEP [10]; oxygen index (OI) PaO/FiO; respiratory index (RI) P (A-a) O/PaO ([PB – PHO FiO – PaCO] – PaO/PaO [11]. The alveolar dead space/ ratio (/) 1.14 (PaCO – PetCO)/PaCO – 0.005 [12]. Here, P (A-a) O indicated the alveolar-arterial gradient; PB, atmospheric pressure; PHO, saturated vapor pressure; FiO, inhaled oxygen concentration (%); PaCO, arterial carbon dioxide partial pressure; , alveolar dead space; , tidal volume; PetCO, partial pressure of end-expiratory CO.
The start of spontaneous breathing was observed by the fluctuation of the breathing bag on the anesthesia machine without automated driving, and the return of spontaneous breathing was facilitated by allowing a full recovery of the upper airway reflexes and return of sufficient spontaneous breathing rate 8 breaths/min, spontaneous 6 ml/kg, or oxygen saturation (SpO 93% at FiO 100%), and the tracheal tubes were extubated. Additionally, patient responses to language and orientation, including naming, repetition, listening, place, and time, provided a rough evaluation of the recovery of conscious state or cognitive function.
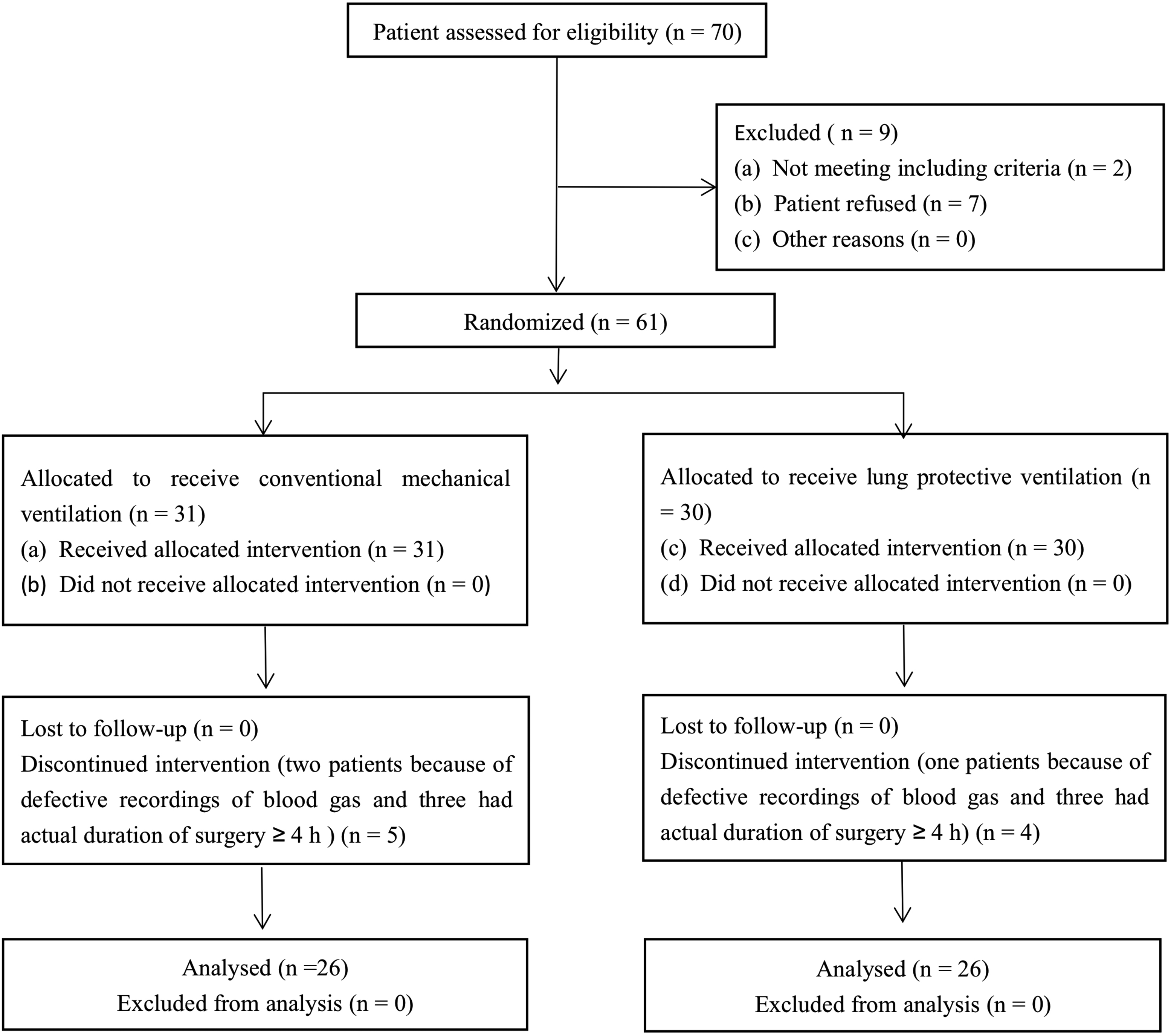
Flow diagram of patient recruitment.
Statistical analysis
A power calculation was performed based on the respiratory index. A pilot study involving six patients at our center indicated that we needed to study a minimum of 25 individuals in each group to detect a 20% difference in the mean RI before and after ventilation was switched to lung-protective mode at both 0.95 (SD 0.28) and 0.80 (SD 0.34) at a power of 95% and a two-sided significance level of 0.05. To compensate for the possibility of dropout, we added 20% more patients for a final sample size of 61 patients.
All data collected in this study were analyzed using SPSS 22.0 software (IBM Inc., Chicago, IL, USA). Normally distributed measurement data were expressed as mean standard deviation (SD), while non-normally distributed measurement data were expressed as median (interquartil range), and the comparisons were examined by Student- test. The Mann-Whitney U test was employed for intergroup comparisons, and the Wilcoxon signed-rank test was used for comparisons between different time points within the same group. The categorical data were expressed as n(%), and the differences between the two groups were examined by chi-square analysis or Fisher’s exact test. 0.05 was considered statistically significant.
Results
We screened 70 patients and included 61 patients. Finally, 26 patients in each group were included in the analysis (Fig. 2). Baseline characteristics are presented in Table 1. Intraoperative data are shown in Table 2, and there was no difference between these two groups.
Baseline characteristics of patients included
Characteristics
CV group ( 26)
LPV group ( 26)
-value
Age, years
72.89 5.21
73.77 4.89
0.531
Sex, male/female
11/15
13/13
0.578
Weight, kg
64.35 9.39
64 23 10.79
0.967
Height, cm
168.65 6.92
170.23 7.06
0.420
BMI, kg/m
22.69 1.62
22.42 2.04
0.601
ASA class
I
2 (7.69%)
3 (11.54%)
0.638
II
19 (73.08%)
18 (69.23%)
0.760
III
5 (19.23%)
5 (19.23%)
1.000
Coexisting condition
History of smoking
7 (26.92%)
9 (34.62%)
0.548
History of alcohol intake
8 (30.76%)
8 (30.77%)
1.000
History of cerebrovascular accident
4 (15.38%)
3 (11.54%)
0.685
History of cardiovascular accident
5 (19.23%)
5 (19.23%)
1.000
Procedures
Radical resection of gastrointestinal tumor
8 (30.76%)
9 (34.62%)
0.768
Left or right hepatic lobectomy
6 (23.08%)
7 (26.92%)
0.749
Bilateral hernia repair
12 (46.15%)
10 (38.46%)
0.575
Notes: Values are given as mean (standard deviation) or number of patients (%). CV group, conventional mechanical ventilation with 8 mL/kg tidal volume (VT) and 0 cm HO positive end-expiratory pressure (PEEP); LPV group, lung-protective ventilation with adjusting VT to a target peak airway pressure with 9 cmHO PEEP. BMI, body mass index; ASA class, American Society Anesthesiologists’ physical status.
Intraoperative data including duration of ventilation or surgery, blood loss, liquid input, and urine output
Variables
CV group ( 26)
LPV group ( 26)
-value
Duration of mechanical ventilation, min
136.56
34.88
133.12
36.42
0.493
Duration of surgery, min
113.0
35.66
117.31
38.09
0.343
Amount of bleeding, mL
254.66
192.74
258.81
191.36
0.936
Colloidal solution, mL
454.80
222.75
480.35
223.77
0.666
Crystalloid solution, mL
1090.43
465.83
993.42
317.78
0.352
Transfusion of red blood cells, mL
267.44
99.87
280.82
53.37
0.709
Packed fresh frozen plasma, n
(30.77%)
(34.62%)
1.000
Urine output, mL
807.65
191.74
827.39
166.46
0.618
Notes: Values are given as mean (standard deviation) or number of patients (%). CV group, conventional mechanical ventilation with 8 mL/kg tidal volume (VT) and 0 cm HO positive end-expiratory pressure (PEEP); LPV group, lung-protective ventilation with adjusting VT to a target peak airway pressure with 9 cmHO PEEP.
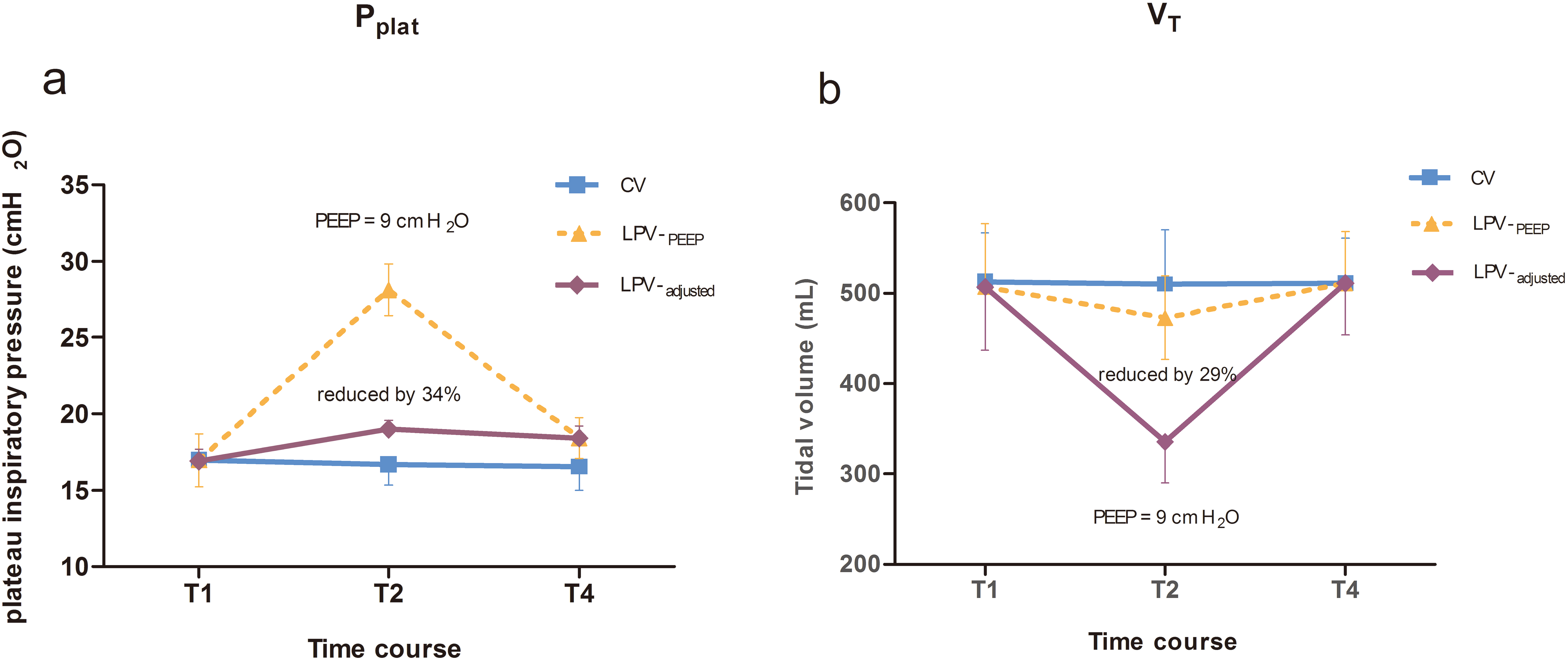
Due to the different MV settings in these two groups, Pplat and were significant different as well. When the PEEP setting reached 9 cm HO, Pplat was significantly increased. However, compared with the CV group with a similar level of Pplat, after LPV was performed as described, Pplat significantly decreased by 34% ( 0.001; 95% confidence interval [CI] 10 to 11) (Fig. 3a) during ventilation and significantly decreased by 29% ( 0.001; 95% CI 121 to 156) (Fig. 3b).
Schematic spirograms for plateau pressure (Pplat) and tidal volumes () between the two groups at three time points (T1, T2, and T4). The conventional ventilation (CV) group (open squares, grey lines). Immediately after 9 cm HO positive end-expiratory pressure (PEEP) setting in the lung-protective ventilation (LPV) group (LPV-, open triangles, dashed lines). After adjusting the tidal volume to limited Pplat in the LPV group (LPV-, closed rhombus, solid lines). Comparison before and after adjusting at 9 cm HO PEEP, the Pplat level in the LPV group significantly decreased from 28.12 1.68 cm HO to 18.42 1.36 cm HO ( reduced by 34%); the level decreased from 472.50 46.50 ml to 335.39 45.08 ml ( reduced by 29%).
Intergroup analysis showed statistically significantly lower MAP values at T4 and T5 and higher HRs at T2, T3, and T5 in the LPV group, whereas similar hemodynamic values were shown in both groups at the beginning of surgery (87.588.06 vs. 89.429.16, 0.444; 73.547.29 vs. 72.737.72, 0.700). However, there was no difference of trend on lower MAP and higher HRs between the two groups, and similar changes in anesthesia depth were observed (42.893.99 vs. 41.465.07, 0.266). Additionally, intergroup comparisons revealed that SpO values were significantly higher in the LPV group at two hours after ventilation, while there were similar values for the two groups at the beginning of surgery (96.081.72 vs. 98.460.81, 0.000; 96.921.26 vs. 96.583.32, 0.622).
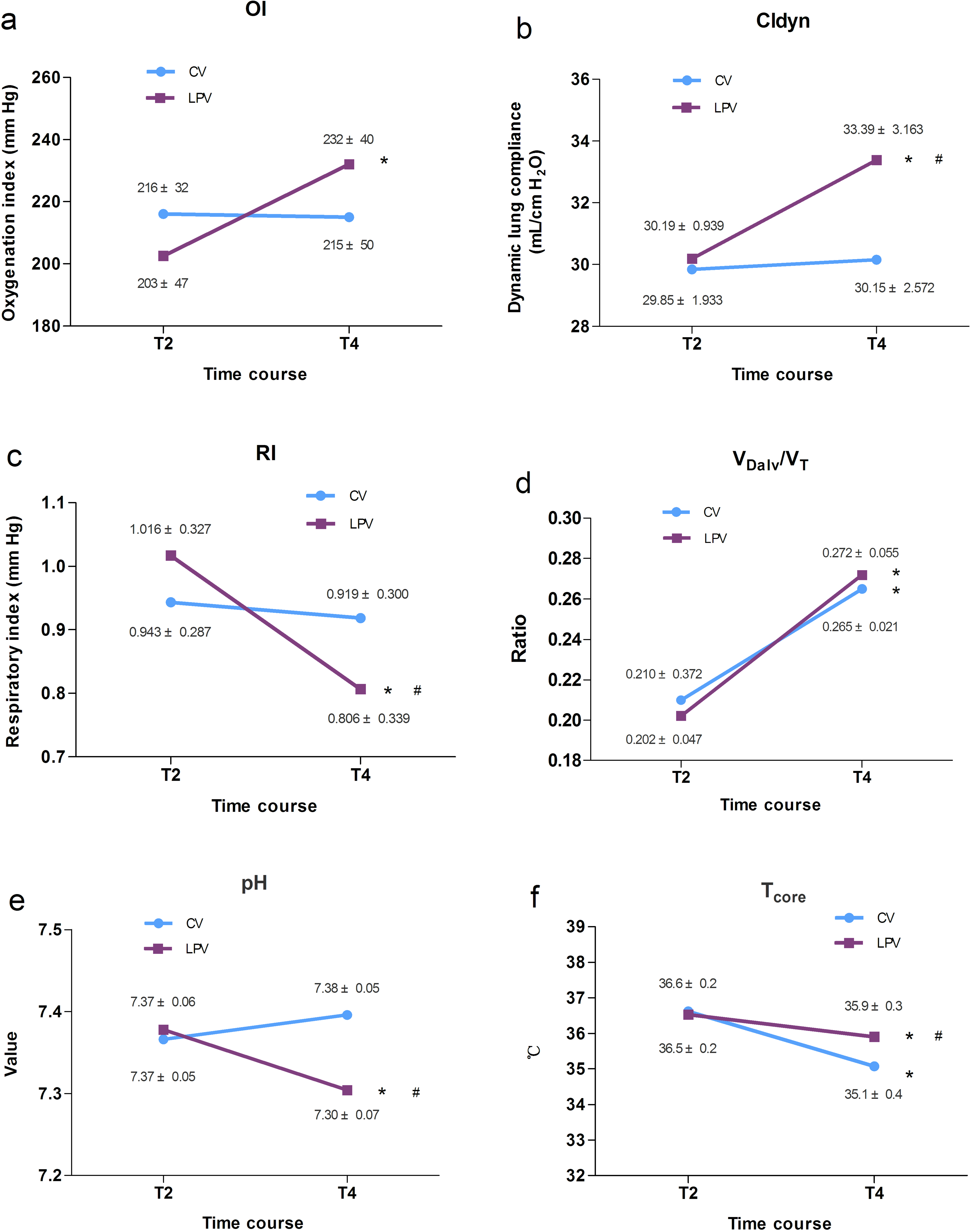
At the end of surgery, The LPV group had significant reductions in RI, pH values and body temperature over time ( 0.027, 0.001, and 0.001, respectively), while OI, CLdyn and / significantly increased ( 0.017, 0.001, and 0.001, respectively). The CV group had a significant increase in / over time ( 0.001), while body temperature significantly decreased ( 0.001). The paired-sample comparison showed significantly higher CLdyn and body temperature (both 0.001) and significantly lower RI and pH values ( 0.043, and 0.001, respectively) in the LPV group than that in the CV group at the end of surgery. The parameters before and after surgery and intergroup comparisons for each item are shown in Fig. 4a–f.
Changes in oxygen index (OI), dynamic lung compliance (CLdyn), respiratory index (RI) levels, alveolar dead space/tidal volume (/) ratio, pH values, and in patients receiving conventional ventilation (CV group) or lung-protective ventilation (LPV group) at T2, just before the commencement of surgery following stabilization of hemodynamic parameters after intubation; T4, 10 minutes before the end of surgery * vs. T2, 0.05; # vs. CV group, 0.05.
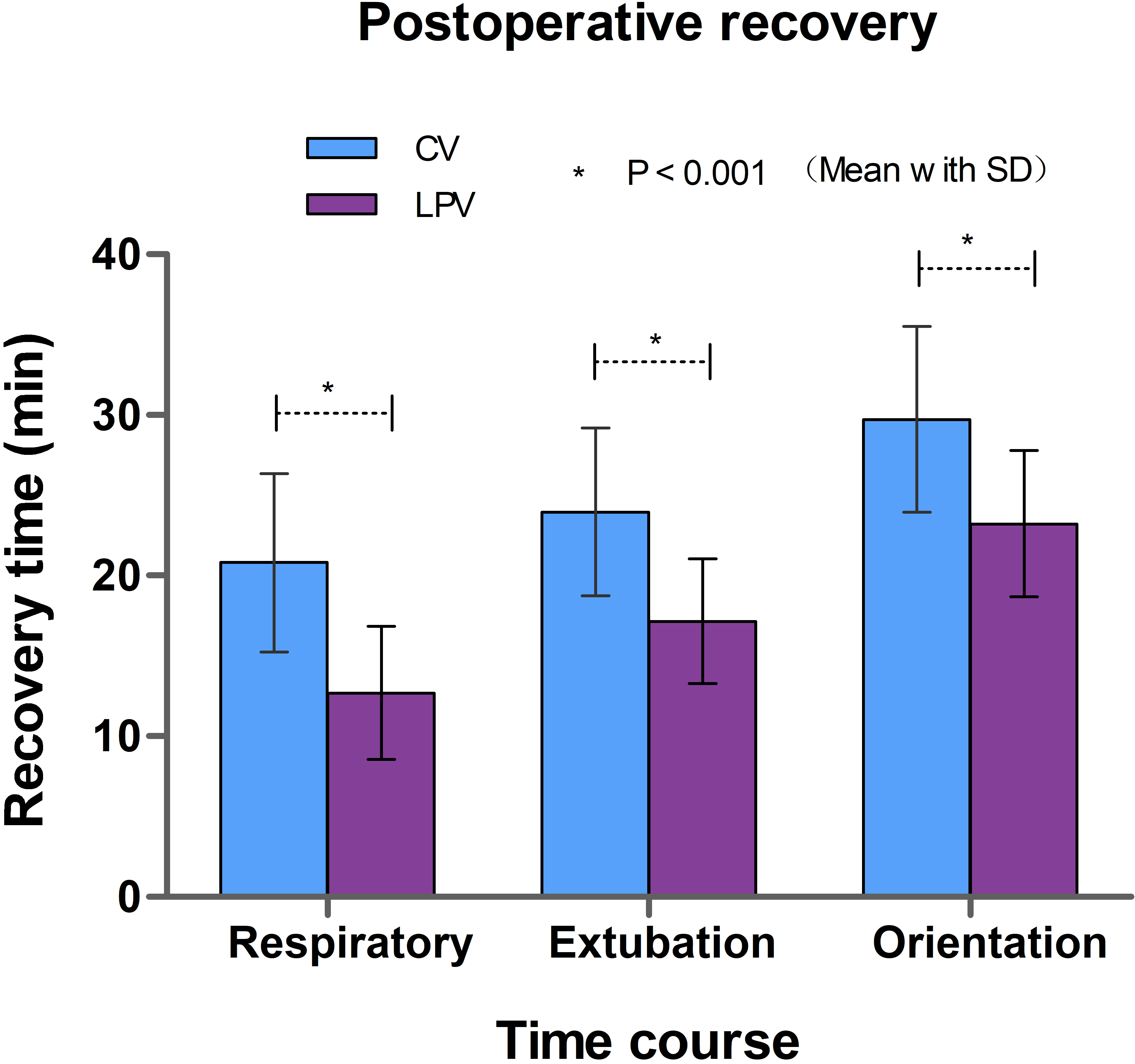
Postoperative recovery was assessed through the emergence time from anesthesia. The time starts from discontinuation of anesthetic administration to spontaneous breathing, tracheal extubation, and orientation in patients receiving conventional ventilation (CV) or lung-protective ventilation (LPV).
The emergence time in the LPV group was significantly faster after the discontinuation of anesthetics, including return time to spontaneous breathing (13 4 min), extubation (16 4 min), and spatial orientation (23 6 min), which were significantly differed from the those in the CV group (21 6 min, 23 6 min, and 30 6 min, all 0.001), respectively (Fig. 5).
Discussion
LPV with low has been widely studied in recent years, especially the use of low calculated based on PBW with optimal PEEP levels. However, there are few studies exploring relationship between selection and PEEP, and even fewer studies on the combination of , PEEP, and Pplat with lung protection. This study was designed to evaluate the effects of LPV with PEEP at 9 cm HO and adjusting to the targeted level of Pplat compared with conventional of 8 mL/kg PBW ventilation. First, LPV adjusting to a limited level of Pplat was feasible after setting a moderate level PEEP. The 29% decrease in was adjusted as a low with 9 cm HO of PEEP and reduced Pplat by 34%. Second, the LPV was beneficial for intraoperative ventilation, as evidenced from the relatively higher CLdyn and OI over time without inducing clinically relevant hemodynamic changes. Third, general observations in elderly patients during open abdominal surgery revealed that the LPV has a significant difference in pH values and body temperatures over time and postoperative early rapid recovery from anesthesia compared with the effects of ventilation with calculated based on PBW without PEEP.
To the best of our knowledge, this study is the first randomized controlled clinical study in which intraoperative MV with a moderate level PEEP and adjusted based on the targeted level of Pplat has been used as an LPV strategy. Although the effects of LPV were determined by analyzing the pH values in our study, assuming that the positive effects of recruitment can be derived from the balance between the alveolar partial pressure of CO and arterial partial pressure of CO and that the LPV had a lower pH value than expected, these findings might be induced by hypoventilation, since all enrolled patients had normal lung function and were managed with a FiO of 0.6. pH is a noncommon monitoring index analyzing the blood acid-base balance and oxygenation during MV, and could be used to reflect the exchange function of alveolar gas and can also accurately reflect the ventilation of the lungs. There was unequivocal evidence that low ventilation will affect the amount of exhaled CO from the respiratory system, which was a crucial determinant of rapid change in arterial blood pH values [13]. However, the distinct differences observed in body temperature over time at identical states of anesthesia before and after LPV supported the idea of a gain in the number of open alveoli by PEEP itself. It maintained the body temperature by good matching of ventilation and perfusion (V/Q), either by appropriate Pplat or better lung compliance associated with efficient gas exchange, or the potential benefit from limited Pplat resulting in moderate respiratory acidosis was associated with an increase in cardiac output [14, 15].
In our study, the open lung approach referred to a strategy to utilize recruitment effects with a moderate PEEP level to maintain the number of open alveoli and lung ventilation, while preventing overdistension by combination with low and low Pplat [16, 17, 18]. On one hand, the PEEP, which removed atelectasis but avoided overdistension while opening lung areas that incorporate low , could be defined as appropriate PEEP [3]. On the other hand, the interaction between assignment and low Pplat was important [19]. These differences emerged, although Pplat was similar in the two groups. These pressures reached 20 cm HO with LPV when providing low to avoid overdistension while optimizing lung mechanics at minimal dead space ventilation by PEEP in all patients. The variable effects for the low Pplat in LPV are related to regulating suitable airway pressure leading to a filling of the lungs with a higher proportion of , thereby inducing minimal atelectasis and an increase in lung compliance and causing a decrease in airway and [20, 21, 22].
Compared with young and middle-aged patients, elderly patients pose particular challenges to adequate MV in addition to surgical constraints, primarily by restricted lung mechanics due to increased small airway dead space and impaired gas exchange [23]. Cognitive impairment could be a problem in elderly patients from the early postoperative period after general anesthesia, for which rapid recovery from anesthesia might offer advantages in these patients [24]. Although we did not determine intrathoracic pressure and pulmonary capillary wedge pressure, the increase in gas exchange during ventilation with limited Pplat and the application of PEEP might indicate that the matched V/Q, at least in part and have been caused by respiratory acidosis to moderate regional blood flow.
There were also several limitations in our study. First, this study included a diverse group of practitioners and procedures, and the findings were likely to be relevant to an equally diverse range of procedures. Second, the time spent on both ventilation groups was limited to less than three hours, and the long-term effects of the proposed strategy were not known. Third, limited Pplat resulted in a decrease in minute ventilation and pH values (moderate permissive respiratory acidosis), which could not eliminate the long-term effects on systemic hemodynamics and tissue perfusion in elderly patients. However, our exploratory sensitivity analysis using a pH value is rare in daily clinical practice. Consequently, further studies involving larger sample sizes, other measurement indexes, such as intrapulmonary shunt rate and systemic inflammatory responses, and whether pH value or were potentially influenced by these variability factors should be explored. An additional group of patients ventilated with adjusting to target the Pplat value to change the I/E ratio or respiratory frequency with PEEP were required for evaluating the effects of LPV for individualized patients.
Conclusions
A moderate PEEP and a target Pplat as low as possible were identified as reference indicators for “passive adaptive” individualized VT and could achieve adequate ventilation and oxygenation. It is helpful to select ventilator strategy for some patients receiving MV during a surgical procedure.
Footnotes
Conflict of interest
None to report.
Funding
Clinical study of positive end-expiratory pressure in small tidal volume mechanical ventilation mediating the effect of airway pressure limitation on pulmonary resuscitation (No. Hwk2018zd014).
References
1.
FutierEConstantinJMPaugam-BurtzCPascalJEurinMNeuschwanderAMarretEBeaussierMGuttonCLefrantJYAllaouchicheBVerzilliDLeoneMDe JongABazinJEPereiraBJaberS. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med.2013; 369(5): 428-437.
2.
De JongMACLadhaKSMaloMFStaehr-RyeAKBittnerEAKurthTEikermannM. Differential effects of intraoperative positive end-expiratory pressure (PEEP) on respiratory outcome in major abdominal surgery versus craniotomy. Ann Surg.2016; 264(2): 362-369.
3.
BlankmanPShonoAHermansBJWesseliusTHasanDGommersD. Detection of optimal PEEP for equal distribution of tidal volume by volumetric capnography and electrical impedance tomography during decreasing levels of PEEP in post cardiac-surgery patients. Br J Anaesth.2016; 116(6): 862-869.
4.
BlumJMMaileMParkPKMorrisMJewellEDechertRRosenbergAL. A description of intraoperative ventilator management in patients with acute lung injury and the use of lung protective ventilation strategies. Anesthesiology.2011; 115(1): 75-82.
5.
AmatoMBMeadeMOSlutskyASBrochardLCostaELSchoenfeldDAStewartTEBrielMTalmorDMercatARichardJCCarvalhoCRBrowerRG. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med.2015; 372(8): 747-755.
6.
VillarJMartin-RodriquezCDominquez-BerrotAMFemandezLFerrandoC, et al. A quantile analysis of plateau and driving pressure: Effects on mortality in patients with acute respiratory distress syndrome receiving lung-protective ventilation. Crit Care Med.2017; 45(5): 843-850.
7.
HemmesSNGama de AbreuMPelosiPSchultzMJ. High versus low positive end-expiratory pressure during general anaesthesia for open abdominal surgery (PROVHIL trial): A multicentre randomised controlled trial. Lancet.2014; 384(9942): 495-503.
8.
LadhaKVidal MeloMFMcLeanDJWandererJPGrabitzSDKurthTEikermannM. Intraoperative protective mechanical ventilation and risk of postoperative respiratory complications: Hospital based registry study. BMJ.2015; 351: h3646.
9.
FerrandoCSuarez-SipmannFGutierrezATusmanGCarbonellJGarciaMPiquerasLCompanDFloresSSoroMLlombartABeldaFJ. Adjusting tidal volume to stress index in an open lung condition optimizes ventilation and prevents overdistension in an experimental model of lung injury and reduced chest wall compliance. Crit Care.2015; 19(1): 1-12.
10.
LinMZhaoXWangHChenLLiS. Respiratory dynamics and dead space to tidal volume ratio volume-controlled versus pressure-controlled ventilation during prolonged gynecological laparoscopic surgery. Surgical Endocopy.2017; 31(9): 3605-3613.
11.
QiangYLiangGYuL. Human amniotic mesenchymal stem cells alleviate lung injury induced by ischemia and reperfusion after cardiopulmonary bypass in dogs. Laboratory Investigation.2016; 96(5): 537-546.
12.
HardmanJGAitkenheadAR. Estimating alveolar dead space from the arterial to end-tidal CO2 gradent: A modeling analysis. Anesthes Analg.2003; 97(6): 1846-1851.
13.
BoutilierRGSheltonG. The statistical treatment of hydrogen ion concentration and pH. J Exp Biol.1980; 84: 35-339.
14.
LaffeyJGJankovRPEngelbertsDTanswellAKPostMLindsayTMullenJBRomaschinAStephensDMckerlieCKavanaghBP. Effects of therapeutic hypercapnia on mesenteric ischemia-reperfusion injury. Am J Respir Crit Care Med.2003; 168: 1383-1390.
15.
HeringRKreyerSPutensenC. Effects of lung protective mechanical ventilation associated with permissive respiratory acidosis on regional extra-pulmonary blood flow in experimental ARDS. BMC Anesthesiol.2017; 17(1): 149. doi: 10.1186/s12871-017-0439-7.
16.
WithSKreysingMSpaethJSchumannS. Intraoperative compliance profiles and regional lung ventilation improve with increasing positive end-expiratory pressure. Acta Anaesthesiol Scand.2016; 60(9): 1241-1250.
17.
HagerDNKrishnanJAHaydenDLBrowerRG. Tidal volume reduction in patients with acute lung injury when plateau pressure are not high. Am J Respir Crit Care Med.2005; 72(10): 1241-1245.
18.
PiXCuiYWangCGuoLSunBShiJLinZZhaoNWangWFuSLiE. Low tidal volume with PEEP and recruitment expedite the recovery of pulmonary function. Int J Clin Exp Pathol.2015; 8(11): 14305-14314.
19.
VillarJMartin-RodriquezCDominquez-BerrotAMFemandezLFerrandoCSolerJADiaz-LamasAMGonzalez-HiquerasENogalesLAmbrosACamiedoDHernandezMMartinezDBlancoJBeldaJParrillaDSuarez-SopmannFTaranconCMora-OrdonezJMBlanchLPerez-MendezLFernandezRLKacmarekRM. A quantile analysis of plateau and driving pressure: Effects on mortality in patients with acute respiratory distress syndrome receiving lung-protective ventilation. Crit Care Med.2017; 45(5): 843-850.
20.
PeterssonJAxMFreyJSanchez-CrespoALindahlSGMureM. Positive end-expiratory pressure redistributes regional blood flow and ventilation differently in supine and prone humans. Anesthesiology.2010; 113(6): 1361-1369.
21.
AmbriskoTDSchrameJHopsterKKastnerSMoensY. Assessment of distribution of ventilation and regional lung compliance by electrical impedance tomography in anaesthetized horses undergoing alveolar recruitment. Veterinary Anaesthesia and Analgesia.2017; 44(2): 264-272.
22.
MaischSReissmannHFuellekrugBWeismannDRutkowskiTTusmanGBohmSH. Compliance and dead space fraction indicate an optimal level of positive end-expiratory pressure after recruitment in anesthetized patients. Anesth Analg.2008; 106(1): 175-181.
23.
CuiYPiXWangCLiuSGongYWangYZhangFShiJLinZZhangXLiE. Effects of different ventilation strategies on exhaled nitric oxide in geriatric abdominal surgery. J Breath Res.2015; 9(1): 016006.
24.
ParikhSSChungF. Postoperative delirium in the elderly. Anesth Analg.1995; 80(1): 1223-1232.