
Abstract
BACKGROUND:
During neurological rehabilitation training for patients with lower limb dysfunction, active rehabilitation training based on interactive force recognition can effectively improve participation and efficiency in rehabilitation training.
OBJECTIVE:
This study proposes an active training strategy for lower-limb rehabilitation robots based on a spring damping model.
METHODS:
The active training strategy included a kinetic model of the human-machine system, calculated and verified using a pull-pressure force sensor We used a dynamic model of the human-machine system and tensile force sensors to identify the human-machine interaction forces exerted by the patient Finally, the spring damping model is used to convert the active interaction force into the offset angle of each joint, obtaining the active interaction force followed by the active movement of the lower limbs
RESULTS:
The experimental results showed that the rehabilitation robot could follow the active interaction force of the subject to provide assistance, thus generating the following movement and effectively helping patients improve joint mobility.
CONCLUSION:
The active flexibility training control strategy based on the virtual spring damping model proposed in this study is feasible, and motion is stable for patients with lower limb dysfunction after stroke Finally, the proposed active training method can be implemented in future work in other rehabilitation equipment and combined virtual reality technology to improve rehabilitation training experience and increase patient participation.
Keywords
Introduction
Spinal cord injury (SCI) and stroke are the two main types of central nervous system injuries that usually result in motor disorders, such as paralysis and hemiparesis, cognitive dysfunction, and psychological problems. SCI is mainly caused by various types of accidents, whereas stroke is caused by an interruption of blood flow to the brain or an obstruction within a blood vessel supplying blood to the brain [1, 2, 3]. Rehabilitation is a primary treatment for patients with SCI and stroke, aiming to provoke motor plasticity and actuate these patients to relearn using their limbs. According to rehabilitation theory, the patient’s sensory feedback is associated with changes in the cerebral cortex providing functional movement recovery, thus minimizing functional deficits and the corresponding risk of injury [4, 5, 6]. However, traditional rehabilitation is labor-intensive and requires several therapists to assist patients with training manually, especially in lower-limb rehabilitation. This places a huge economic burden on the healthcare systems of countries [7].
Over the past decades, several studies have demonstrated that rehabilitation robots have great potential to improve diagnostic and physiotherapy outcomes [8, 9, 10, 11, 12, 13, 14]. These robots combine rehabilitation medicine with robotics and are mainly used for daily assistance and rehabilitation of people with functional impairment, including completing muscle strength training, joint mobility training, proprioceptive exercise training programs, and balance function training. Compared to traditional rehabilitation methods, rehabilitation robots can become more effective by providing repetitive, accurate and controlled movement therapy. Active training of rehabilitation robots is mainly aimed at patients in the middle and later stages of rehabilitation. After a certain period of passive training, the patient’s muscle strength and neuromotor function areas of the brain were restored to a certain extent The patient could perform a certain degree of micromotion according to his consciousness. During this period, the rehabilitation robot recognized the movement intentions of the patient’s limbs for active rehabilitation [9]. Active training maximizes patient participation and is more effective than passive training. However, achieving active training is challenging. Because these robots interact with humans during therapeutic movement, they require a high degree of security and reliability. Therefore, rehabilitation robots should identify the patient’s activities to reach only predefined training objectives, a method known as the Assist-as-Needed Paradigm [15] Rehabilitation robots helping patients with active training generally need to address the following aspects:
Accurate and reliable identification of motor intention during humanrobot interactions; Control of the robot for on-demand assistance based on the acquired human-machine interaction force; Ensuring the stability of the robot system operation during humanrobot interaction.
Numerous researchers have investigated the aspects mentioned above. Some studies have shown that bioelectric signals intuitively reflect the body’s movement intentions. For example, a patient’s muscle state can be reflected more intuitively by surface EMG signals, and the situation in the relevant motor areas of the cerebral cortex can be reflected intuitively by EEG signals [16, 17, 18, 19, 20]. Yanshan University designed a seated/horizontal exoskeleton lower limb rehabilitation robot based on rehabilitation training methods for patients with different muscle strengths [21, 22, 23] and established a human-machine dynamics model to analyze the driving force required for each joint in a variable workspace. Moreover, the human-machine kinetic model was developed to analyze the driving forces required to move each joint in a variable workspace. The developed model was combined with surface EMG signals to achieve human-machine interaction to complete passive training, active-assisted training, and active resistance training. However, the EMG signals are susceptible to interference and noise, and measurement inconsistencies exist.
In addition to bioelectric signal analysis, the robot’s kinetic model and sensor measurements can be used to identify movement intentions, which are more intuitive and easy to understand. The force and position data of the training movements are used to model and control the mechanical leg in the therapy mode to simulate the training trajectory. However, this model does not reflect the real movement characteristics of the human body or a human kinetics-based model. Thus, it cannot be effectively applied to patients with different conditions [24]. The Harbin Institute of Technology has developed a mathematical model of the FES bicycle training system based on the corresponding crank angle and speed of the bicycle and the state of the muscle groups during joint flexion. Furthermore, a humanmachine dynamics model was developed based on Lagrange’s equation and joint moments for simulation purposes, which can achieve lower limb rehabilitation for SCI patients. However, the end-traction lower limb rehabilitation robot may have relative human-robot displacement; therefore, the training effect is not ideal; the force point is at the ankle joint, which indirectly drives the hip and knee joints and easily causes muscle spasms.
In conclusion, the existing lower-limb rehabilitation training equipment at home and abroad cannot effectively identify the human-robot interaction force and does not provide a reasonable active training strategy based on the human-robot interaction force.
System overview of the lower limb rehabilitation robot. (a) human-machine coupling system general view. (b) Description of pressure sensor locations.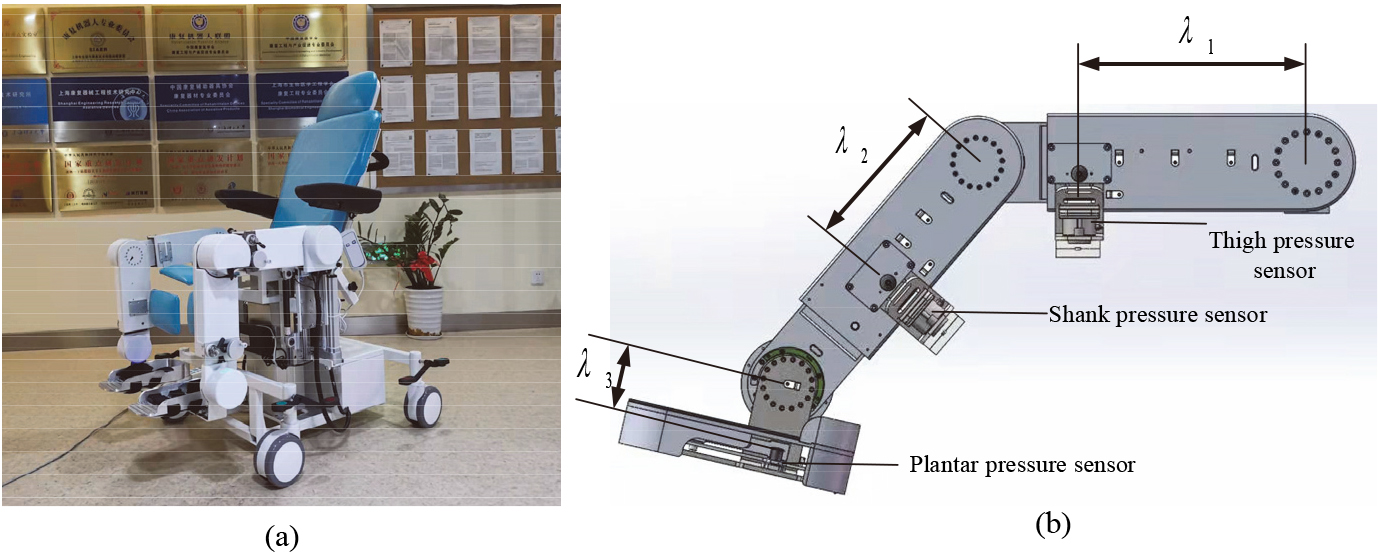
In this study, an innovative mechanism is proposed for humanmachine interaction force recognition. System overview of the lower limb rehabilitation robot as shown in Fig. 1, with pressure sensors on the thigh, shank, and plantar. The distance between the thigh pressure sensor and center of rotation of hip joint is
Active flexibility training control scheme.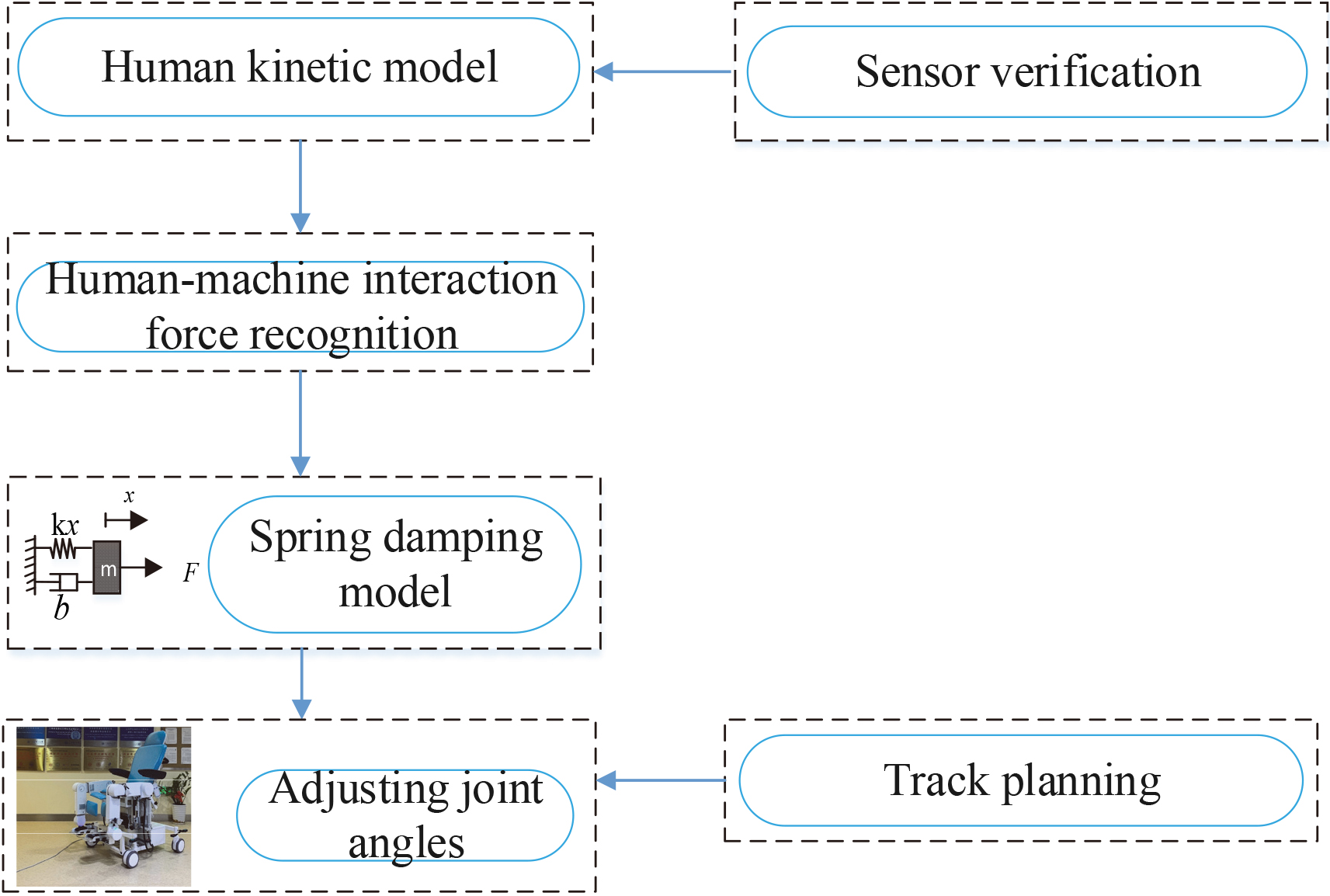
Human kinetic modeling is the study of the human body as the object of kinetic analysis to obtain the physical quantities of position, velocity, and acceleration used to describe the relationship between the movement of the human body and the physical forces acting on it [25, 26]. Human motion modeling and analysis are essential for human health monitoring, medical diagnoses, prostheses and orthoses design, rehabilitation robots, and energy supply to wearable devices [27]. The human anatomy and daily activity trajectory show that the human lower limb mostly completes the joint movements in the sagittal plane. In contrast, the movement is smaller in the horizontal and coronal planes. Therefore, the dynamic analysis in the human body can be reduced to the human lower limb through the joint connection of a three-link mechanism. The Lagrangian function relies on the relationship between the kinetic and potential energy to describe the dynamic state of the entire physical system, which can simplify the complex mathematical model. Therefore, this study uses the Lagrangian method to establish the dynamic model of the human body.
Three-link model of the human lower limb.
The three-link model of the human lower limb is shown in Fig. 3. Each joint coordinate is a combination of Cartesian and generalized coordinates, where the generalized angle is the angle between the links and the Y-axis, and the coordinate origin O1 is set at the center of rotation of the hip joint. The center of rotation of the hip joint, knee, ankle joint locates at points A, B, and C, respectively, D is the end of the foot;
Deriving Eq. (1), the velocity at D is given by Eq. (3) as follows:
The Lagrangian operator
That is, the Lagrangian equation is as follows:
Where
The human-machine interaction force is mainly identified by the pressure sensors with the human kinematic model. The location of the sensors in the mechanism is shown in Fig. 1b.
After obtaining the human-machine interaction force, the rehabilitation robot should assist the patient in performing active rehabilitation training according to the size of the interaction force and the patient’s physical condition on demand. This task requires the system to operate stably. To address this problem, this study uses a virtual spring-damping model, as shown in Fig. 4, where m is the virtual model mass, k is the elasticity coefficient,
Spring-damping model.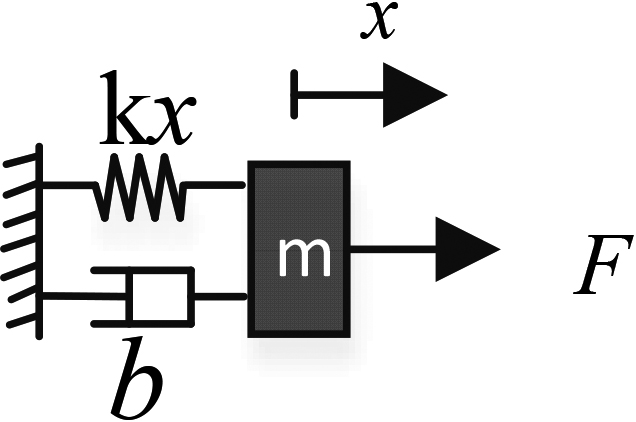
This model allows establishing the relationship between the human and machine interaction forces and the joint deflection angle. Moreover, the spring-damping model can be analyzed dynamically using Newton’s second law of motion, as follows:
The Laplace transform is applied to convert Eq. (13) into the frequency domain for analysis as follows:
The transfer function of the spring-damping model is obtained by rectification as:
If the denominator term of the transfer function is set to zero, the characteristic equation of the spring-damped model system is obtained as follows:
The damping ratio is introduced as
The characteristic roots of the characteristic equation are as follows:
In addition, the spring-damping model allows not only the relationship between force and position to be derived but also the stability of the system to be optimized by adjusting the
During the rehabilitation training process, the patient is the object being rehabilitated, as well as the operator and controller of the rehabilitation robot, that is, the human and the machine, form a closed-loop system. The active training process often requires the rehabilitation robot to assist with demand, that is, the robot recognizes the motor intent based on the patient’s interaction force and assists the patient in completing the desired movement. The active supple training control strategy proposed in this study is shown in Fig. 5. The method considers each robot motion joint as a virtual spring-damping model. Moreover, the human-machine interaction force of each joint was accurately identified in the previous part of this study using a kinetic model and a tensile force sensor. The interaction force is used as an input to the spring-damping model and is controlled by adjusting the parameters of the model to compensate for the assistance or increase the damping. Then, the displacement output of the model is calculated. The rehabilitation robot uses the displacement output of the model as trajectory correction to plan its trajectory so that the rehabilitation robot can “follow” the body’s movement smoothly.
The rehabilitation robot controller uses a microprocessor and requires the discretization of the kinematic equations of the spring damping model. Here is an example of a single joint. Assume that the acceleration of the model at moment
Active flexibility training control strategy based on the spring-damping model.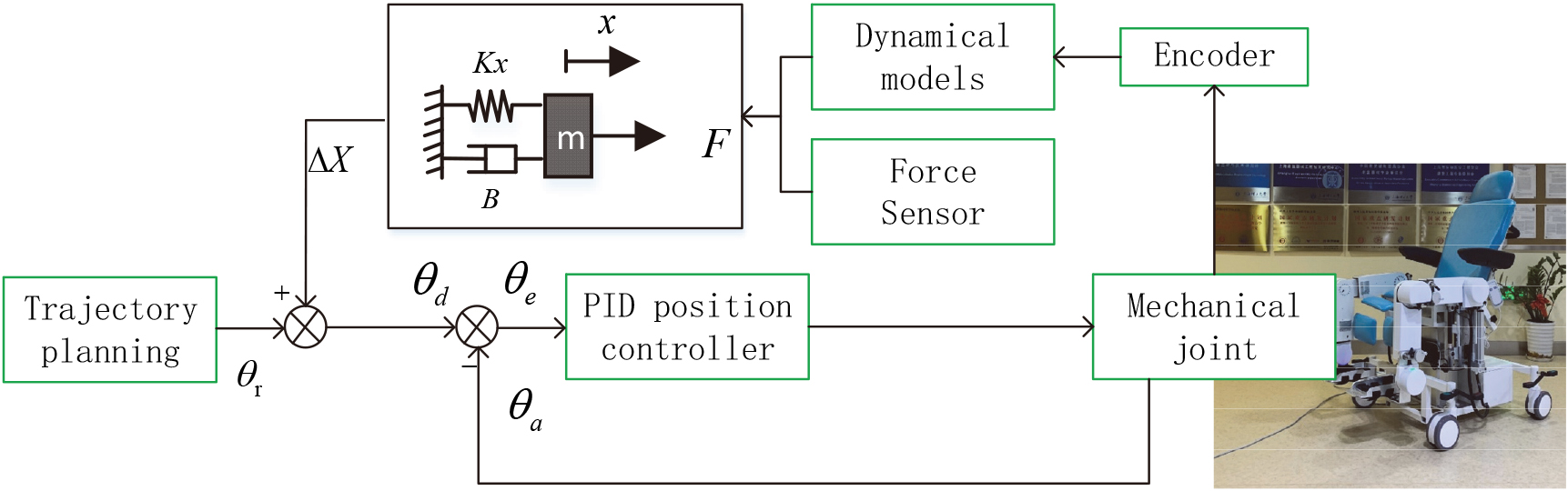
Human kinetic model verification experiment protocol
Before validating the human dynamics model, we must obtain the body dimensions and inertia parameters. This study refers to the national standard GB-T 17245-2004 Human Inertia Parameters for Adults, published by the National Standardization Administration of China [28]. The human body inertia parameters include body mass, the position of the center of mass, and rotational inertia. According to the standard, the mass, length, and position of the center of mass of each body segment can be obtained from the binary regression parameters of the height and weight of the test subject.
Coefficients of binary regression equations of mass and center of mass on body weight (W, kg) and height (H, mm) for Chinese men and women by body segment
Coefficients of binary regression equations of mass and center of mass on body weight (W, kg) and height (H, mm) for Chinese men and women by body segment
Note: (1) The regression equation is
(2) The center of mass position,
Five subjects (two females and three males) were recruited for verification of the human lower limb kinetic model. The individual segment centers of the mass locations and masses were obtained, as shown in Table 1. The length of each body segment of the human lower limb was obtained by measurement The detailed parameters are listed in Table 2.
Parameters of subjects’ lower limbs
Trajectories were planned for the hip, knee, and ankle joints of the robot to assist the subjects in passive training. During rehabilitation training, the subject was asked to maintain the muscles relaxed, that is, the interaction force was zero. The angles, angular velocities, and angular accelerations of each joint were planned as follows:
Hip, knee, and ankle angles, angular velocity, angular acceleration planning curve.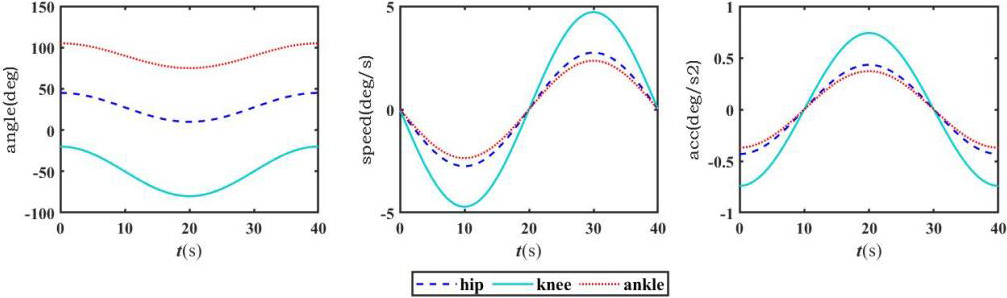
Figure 6 shows hip, knee, and ankle angles, angular velocity, angular acceleration planning curve. Equations (21)–(23) are substituted into Eqs (8)–(10) to calculate the theoretical value of each joint torque
Theoretical forces on tensile pressure sensors.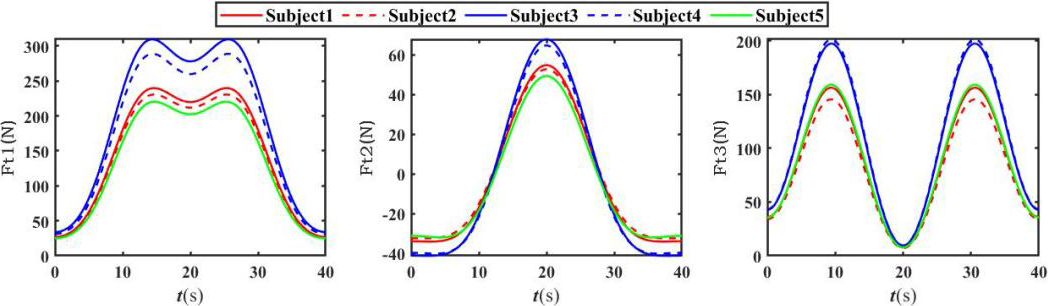
The error between the theoretical and actual force on tensile pressure transducers.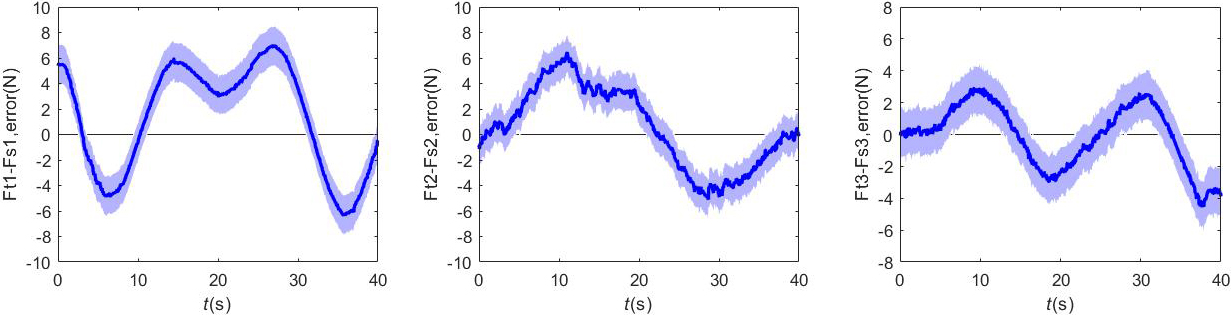
In order to verify the stability and effectiveness of the active compliance training control strategy of the lower limb rehabilitation robot, five subjects (two females and three males, same as 3.1 Human kinetic model verification experiment protocol) were recruited for an active rehabilitation training trial. The device posture was adjusted to the supine position prior to training. The experimental platform is shown in Fig. 9. Each subject was asked to deliver an arbitrary interaction force during the experiment. During the experiment, hip and knee joint angle data, and force sensor data were collected. Finally, analyse the relationship between joint angles and human-machine interaction forces during training.
The results are displayed in Figs 10 and 11. The figures show the relation between the amount of subject active force and the positions of the hip and knee joints. As shown, the rehabilitation robot can follow the changes in the subject’s primary force and provide the corresponding assisted force regardless of the changes in the active force in the lower limb, such that the joint angle follows the active force magnitude. The range of motion of the hip and knee joints during the experiment was 0–60
Active flexibility training experiments.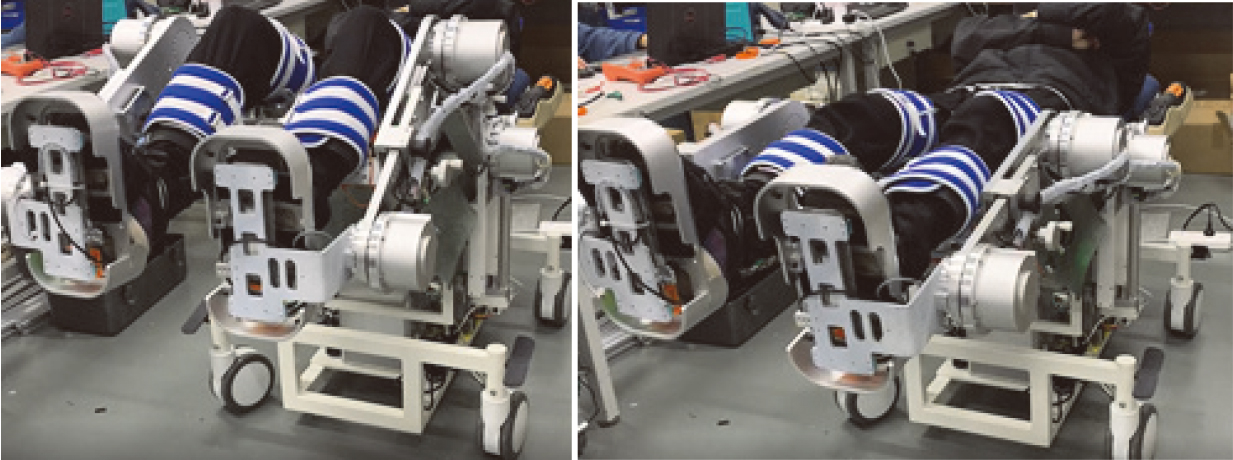
Hip joint force-angle curve.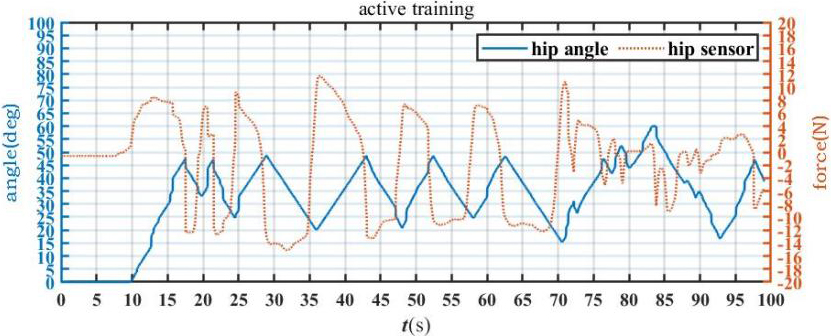
Knee joint force-angle curve.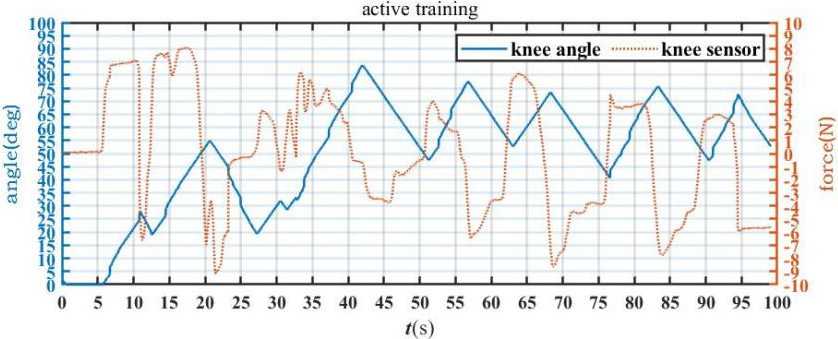
In this study, a human kinetic model was developed and validated using a tensile force sensor. A method for identifying human-machine interaction forces was proposed using a kinetic model and sensor, which avoids the complex calculations associated with coupled human-machine modeling and the instability associated with the bioelectrical signal acquisition. After identifying the human-machine interaction forces, an active compliance control strategy for the lower-limb rehabilitation robot was proposed using a spring-damped model. The spring-damped model kinematic system is a typical second-order dynamic system. This method makes full use of the stability analysis of typical second-order dynamic systems to determine the model parameters. The results of Human kinetic model verification experiment show that HMI force recognition method is stable and reliable. The results of active flexibility training experiment show that the rehabilitation robot can follow the active interaction force of the subject to provide assistance, thus generating the following movement. This can effectively help patients improve their joint mobility. The parameters of the spring damping model can be dynamically adjusted according to the recovery condition of the patient. The parameters can be adjusted to change the level of assistance or resistance of the robot joints, thereby adapting to the different abilities of the patient or rehabilitation stages of the same patient. This study provides a feasible solution for the active training of other types of neurorehabilitation robots. Considering this, assisted training based on EMG control and virtual reality interaction is an important area for subsequent research [29].
Conclusion
This paper proposes an active rehabilitation training control method. The experimental results showed that the method could achieve active compliance training with a stable system. In future studies, we can extend the proposed active training method to other rehabilitation equipment and combine virtual reality technology to improve the rehabilitation training experience and increase patient participation.
Footnotes
Conflict of interest
No conflict of interest exists in the submission of this manuscript. All authors approved the manuscript and its submission to the journal for publication.
Funding
This work was supported by the National Natural Science Foundation of China (Grant no. 62073224).