
Abstract
BACKGROUND:
Despite advances in the treatment of sepsis over time, this condition remains both a serious threat and a cause of death among critical patients.
OBJECTIVE:
This study aimed to explore the role of the nuclear factor kappa B (NF-
METHOD:
A total of 32 Sprague Dawley rats were randomized into a sham operation group and three groups with sepsis, which were tested at one of the following time-points: 3, 6, or 12 h. Each group included eight rats. Sepsis models were created via cecal ligation and puncture procedures. All the study rats had the following cardiac parameters and serum levels measured at either 3, 6, or 12 h after the operation (according to their assigned group): heart rate, left ventricular systolic pressure (LVSP), maximum rate of left ventricular pressure rise (
RESULTS:
Compared with the sham operation group, the rats in the sepsis subgroups exhibited significantly lower values for all the cardiac parameters measured, including the heart rate (sham operation group
CONCLUSION:
Sepsis can lead to myocardial injury and cardiac dysfunction. This may be related to the activation of the NF-
Keywords
Background
Sepsis is a life-threatening organ dysfunction that results from a host’s disordered response to an infection [1]. Despite advances in the treatment of sepsis over time, this condition remains both a serious threat and a cause of death among critical patients. This condition involves multiple organ dysfunction and accounts for 6% of inpatients and 15% of hospital deaths [2]. Epidemiological studies have shown that the prevalence of septic cardiomyopathy (SCM) in general population varies from 10% to 70%. The two main factors that may explain this considerable difference in reported prevalence are a lack of consensus on the diagnostic criteria for SCM and the diversity of techniques used to evaluate cardiac function [3]. The prevalence of SCM increases as the severity of the sepsis increases [4, 5]. Septic cardiomyopathy is characterized by left ventricular dilatation and a reduced left ventricular ejection fraction, with a return to normal cardiac function within 7–10 days [6]. As a reversible myocardial dysfunction in patients with sepsis, SCM has gradually gained more attention. For this reason, research into the pathogenesis, prevention, and treatment of this disease is clinically important and has the potential to improve the prognosis of patients with sepsis and to lower their overall mortality rate.
The pathogenesis of SCM is extremely complicated and is still not entirely understood. The occurrence of the disease is associated with several factors, including the body’s immune response, cytokine production, mitochondrial dysfunction, oxidative stress injury, the presence of exosomes in cardiomyocytes, cell apoptosis, and gene regulation [7, 8, 9]. Inflammatory cytokines in particular may play a major role in the pathogenesis of SCM. At the time of sepsis onset, lipopolysaccharides (LPSs) are delivered to the surface of a variety of immune cells, such as monocyte macrophages, and bind to the CD14/TLRs-MD2 complex on the membrane, activating nuclear factor kappa B (NF-
Due to the complexity and heterogeneity of systemic immune response in sepsis, it is important to develop appropriate animal models and optimize research conditions to reveal the biological mechanism of sepsis. Cecal ligation and puncture (CLP) is a standard animal model of sepsis [12], which is usually used to study the pathogenesis and treatment target of sepsis. It is a simple and reliable method to control the puncture count in the CLP mouse model, which can achieve a consistent survival rate. The contents of the cecum continue to diffuse into the abdominal cavity, causing bacteria to enter the blood, eventually leading to systemic inflammatory response syndrome and multiple organ dysfunction syndrome. Therefore, the CLP mouse model can partially represent the progress of pathophysiological phenomena similar to human, such as the changes in the early stage of inflammation, and show cytokine dynamics similar to clinical sepsis [13, 14]. However, CLP model can only reproduce the immune, hemodynamic and metabolic stages of clinical sepsis to a certain extent. Whether it can simulate human sepsis is still unknown. Compared with the diagnostic criteria of human sepsis, the basic parameters and indicators of CLP model still lack comprehensive understanding [15].
In this study, sepsis rat models were created using the cecal ligation and puncture (CLP) method to explore the role of NF-
Method and materials
Preparing the animals and the sepsis model for the experiment
A total of 32 healthy adult male Sprague Dawley rats (specific pathogen-free grade), each with a body weight of 350–420 g, were provided by the animal laboratory of Xuanwu Hospital, Capital Medical University, Beijing, China. The rats had been raised in a standard pathogen-free animal room, with 12 h alternate light/dark cycles before the experiment; water and standard rodent feed were provided without restriction. Before the experiment, the animals were acclimated to the environment where the study was conducted for one week. Based on recommendations derived from international expert consensus on preclinical sepsis research, the CLP sepsis model was used for this study [16, 17].
Before the surgery, the animals were anesthetized using an intraperitoneal administration of 20% urethane (5 mL/kg). The effect of urethane is reversible when used in the concentration range of 10–300 mmol/L [18]. The lower quadrants of the abdomen were shaved using a trimmer, and the area was disinfected with alcohol prep pads. Next, a longitudinal skin midline incision was made with a scalpel under aseptic conditions, avoiding any penetration of the peritoneal cavity. After the initial incision, small scissors were used to increase the length of the incision to 3–4 cm and to enter the peritoneal cavity. The cecum was located, isolated, and exteriorized using blunt anatomical forceps. The ligation was achieved with surgical sutures at the point that marked the beginning of the distal third of the cecum. Before cecal perforation, the cecal contents were pushed gently toward the distal cecum. The cecum was perforated by three through-and-through punctures with a sterile 20-mL syringe needle in a mesenteric-to-antimesenteric direction, midway between the ligation point and the tip of the cecum. After needle removal, a drop of stool was extruded from the mesenteric puncture and the reverse mesenteric puncture to ensure patency. The cecum was then returned to the abdominal cavity. Next, the incision was sterilized again with iodophor, and the abdominal wall incision was sutured layer by layer. The animals were administered 5 mL of normal saline subcutaneously after the procedure as a means of preventive fluid replacement.
Experimental grouping
All the rats were fasted overnight for 12 h before the experiment, although they had free access to water. They were randomized into four groups, each of which contained eight animals, as described in the following paragraphs.
The sham surgery group ( Subgroups examining the response to sepsis at 3 (
The anesthetized rats were fixed in a supine position; a polyethylene catheter, connected to a BL-420F biological signal acquisition system (Chengdu TME Technology Co. Ltd., Chengdu, China), was inserted through the common carotid artery into the left ventricle. The following indices were recorded once the rats’ condition had been stabilized: heart rate (HR), left ventricular systolic pressure (LVSP), and the maximum rate of left ventricular pressure rise (
Collecting the serum specimens and measuring cardiac troponin I, tumor necrosis factor alpha, interleukin 1 beta, and interleukin 6
The rats in all the groups were subjected to blood sampling (5 mL) via the arterial line after their cardiac function measurements had been completed at the assigned time point (3, 6, or 12 h after CLP), and the blood samples were stored at
Preparation of the collected myocardial tissue for histopathological examination and western blot analysis to determine the expression of toll-like receptor 4 and nuclear factor kappa B
After the serum samples had been collected from the rats in the study, their chests were opened and their left ventricular myocardium was collected. A small part of the myocardium was stored in liquid nitrogen for subsequent western blot analysis to determine the levels of toll-like receptor 4 (TLR4) and NF-
Statistical methods
The measurement data were expressed as mean
Results
General condition of the rats in each group
The rats in the sham operation group were essentially healthy following recovery from anesthesia, with slow movement and acceptable reactions. They were capable of eating and drinking at will, showed an absence of obvious abnormality in their second stool samples, and the color and luster of their fur were normal. The rats in the sepsis groups exhibited mental fatigue, a significant decrease in activity, a reduced reaction capacity, rigors, opaque discharge around the eyes, and noticeably darker urine following recovery from anesthesia. Observation by laparotomy, following the death of the sepsis rats, found pale and bloody peritoneal exudate, a fecal odor, intestinal wall congestion, and dark purple edema (and purple-black necrosis in severe cases) in the ligated segment of the cecum. The above findings were most obvious in the 12-h group.
Mortality of the rats in each group
All the rats in the sham operation group survived (mortality
Hemodynamic results of the rats in each group
The HR of the rats in the three sepsis groups was much lower than those in the sham operation group (sham operation group
HR (times/min) and LVSP (mmHg) of rats in each group
HR (times/min) and LVSP (mmHg) of rats in each group
Note:
The LVSP values of the rats in the three sepsis groups were much lower than those in the sham operation group (sham operation group
The
Note:
The mean serum TNF-
Test results of rat serum samples in each group
Test results of rat serum samples in each group
Note:
Results of the histopathology sections of rat myocardium in each group. A: Sham operation group, B: Sepsis 3-h group, C: Sepsis 6-h group, D: Sepsis 12-h group.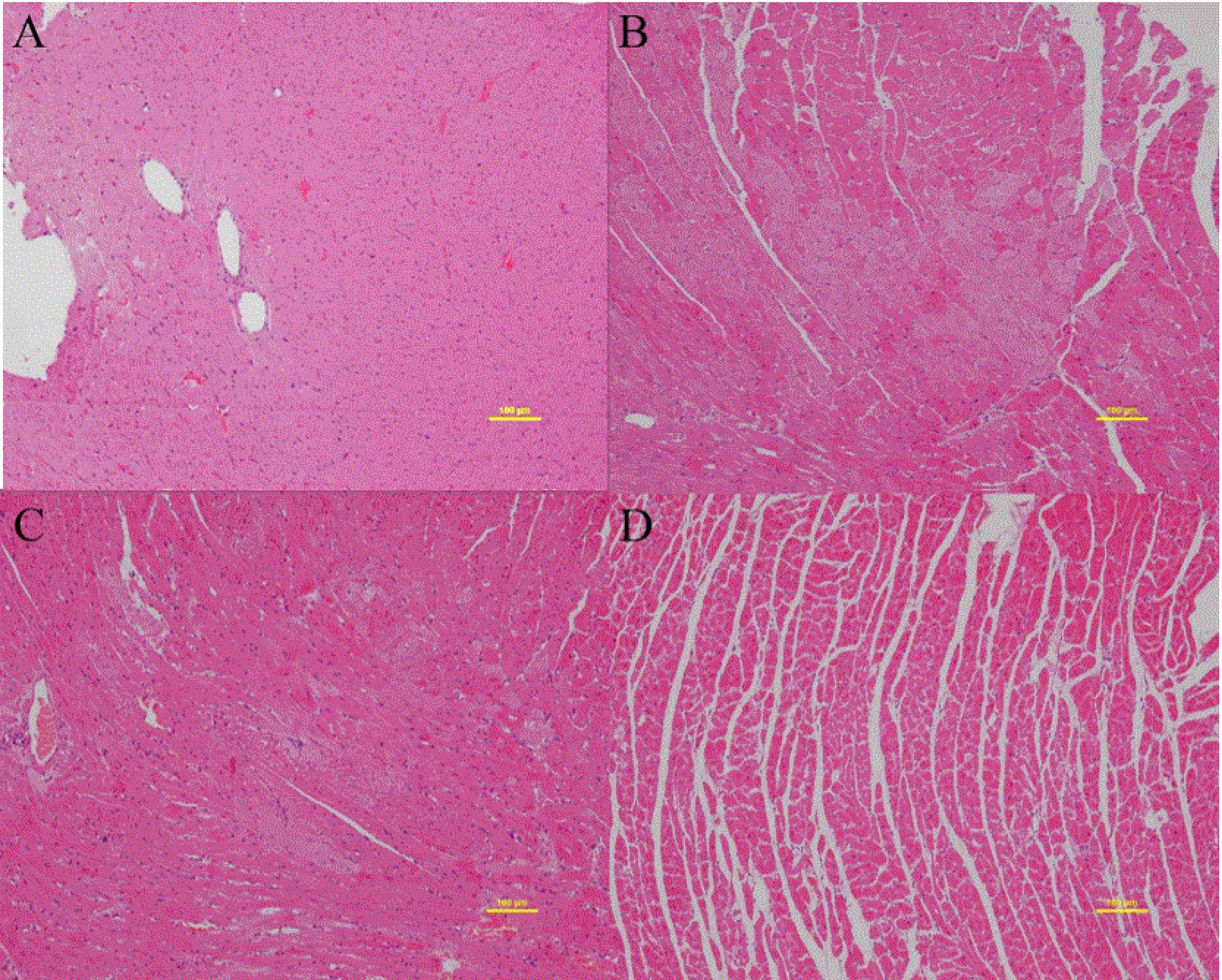
Compared with the sham operation group, the sepsis groups exhibited granular degeneration of the myocardial fibers, edema, and faded staining. These pathological changes were more pronounced at each subsequent time point, and some of the specimens from the 12-h group demonstrated myocyte necrosis and the disintegration and fracture of muscle fibers (see Fig. 1).
Western blot analysis results of toll-like receptor 4 and nuclear factor kappa B expression in the myocardium for each group
Expression of proteins of TLR4 and NF-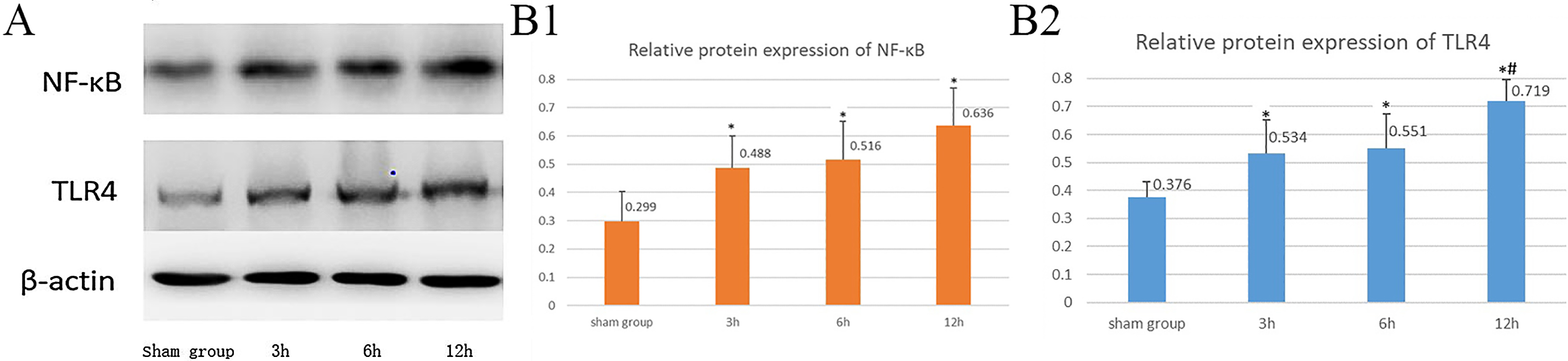
As shown in Fig. 2, the western blot analysis reflected a weak expression of both TLR4 and NF-
The animals in all the sepsis groups exhibited significantly higher levels of TLR4 and NF-
In the sepsis groups, the relative expression of TLR4 and NF-
Complications associated with sepsis include multiple organ dysfunction that can involve the heart, lungs, and kidneys [14]. Studies have shown SCM to be independently associated with early mortality and morbidity in cases of cardiovascular disease following discharge [15]. Septic cardiomyopathy is characterized by myocardial systolic/diastolic dysfunction, cardiac enlargement, reduced ejection fraction, poor systolic response to volume loading, and a reduced peak systolic pressure/end-systolic volume ratio [16]. Approximately 50% of patients with SCM suffer from diastolic cardiac dysfunction, which is closely linked with high mortality rates [17].
In the current study, the hemodynamic parameters of the rats in each group were measured using left ventricular catheterization. The LVSP and
The cTnI is a specific marker of myocardial injury and is secreted into the blood immediately after the myocardial cell membrane is damaged [15, 19]. Existing studies reveal that the release of cTnI during sepsis is highly associated with left ventricular dysfunction and a poor prognosis [20, 21, 22]. Sepsis-induced cardiac dysfunction and a reduced cardiac output lead to reduced tissue perfusion, thereby increasing the risk of death. Abraham et al. [15] suggest that 67% of septic patients in intensive care units experienced an elevated cTnI level within days of hospitalization, indicating myocardial injury. This was closely related to early mortality and postdischarge cardiovascular events. In the current study, all sepsis groups recorded an elevated cTnI, beginning in the 3-h group and peaking in the 12-h group, suggesting that myocardial cell damage occurred in the early stage of sepsis. As the sepsis progressed with time, the damage gradually worsened, and the cardiac diastolic and systolic functions decreased. Thus, an elevated cTnI level during sepsis serves as an important indicator that patients are at high risk of experiencing cardiovascular complications.
Histological examination can verify the presence of LPS-mediated myocardial injury. In the present study, the myocardial specimens of some rats in the 3-h sepsis group were observed to have granular degeneration of the myocardial fibers, edema, faded staining, inflammatory-cell infiltration, and other pathological changes on histopathological examination, which became more pronounced over time. Some myocardial specimens from rats in the 12-h group showed severe degeneration of the muscle fibers, edema, an increase in muscle fibril gaps, and the necrosis and disintegration of individual muscle cells, with a large amount of inflammatory-cell infiltration at the focal necrosis site. This is consistent with existing study findings [23].
Cascades of inflammatory factors play a key role in the onset and development of sepsis. As a bacterial product, LPS can stimulate monocytes, neutrophils, endothelial cells, and cardiomyocytes to initiate the inflammatory process and to produce proinflammatory cytokines. The stimulation of proinflammatory cytokine production by LPS is also one of the major underlying mechanisms of SCM [23, 24]. For example, it can lead to TNF-
Although inflammatory cytokines play an important role in sepsis-related myocardial damage, studies indicate that the prognosis of the disease cannot be improved by interventions involving one specific factor alone [15]. However, the myocardial damage caused by sepsis may be effectively relieved by intervening in the initial stages of inflammatory cascades. This can be achieved by targeting the initial event that generated inflammatory cytokines and caused signal transduction pathways to make changes in the cells. Toll-like receptors are commonly linked to the increased production of proinflammatory cytokines, and TLR4 is a type-I transmembrane protein and an LPS receptor that is responsible for signal transmission; it plays an important role in the initiation of the inflammatory response to sepsis [26]. Nuclear factor kappa B, a transcription factor, is crucial to various conditions, such as the autoimmune and inflammatory responses and atherosclerosis. In a resting state, NF-
In this study, HR, LVSP,
The observation phase point of this study is 3 h–12 h. Prolonged observation time can better reflect the pathophysiological process of septic cardiomyopathy. If the change of cardiac function is monitored by transthoracic echocardiography, it can more comprehensively reflect the condition of cardiac function in sepsis. In the future, it is necessary to further observe the effects of TLR4 inhibitors or clinical treatments that may have related effects, and further clarify NF-
Conclusion
The current research status of septic cardiomyopathy is described in the introduction. The mechanism of septic cardiomyopathy is not yet fully understood. Previous studies have suggested that the occurrence of septic cardiomyopathy is associated with a variety of factors. In this study, we further investigated the relationship between TLR4-activated NF-
In conclusion, the findings of this study indicate that first, evidence of cardiac dysfunction and myocardial injury is evident in rat models with CLP-established sepsis at 3 h following surgery, and second, the TLR4 and NF-
Ethics approval and consent to participate
The study was conducted with approval from the Ethics Committee of Xuanwu Hospital Capital Medical University (LYS [2019] No. 078). The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
This work was supported by Beijing Municipal Administration of Hospitals Incubating Program (No. PX2019028).
Author contributions
Conception and design of the research: XRX, JQ; Acquisition of data: LPL, YWG; Analysis and interpretation of the data: LPL, JW; Statistical analysis: LPL, XRX; Obtaining financing: XRX; Writing of the manuscript: XRX, YLL; Critical revision of the manuscript for intellectual content: YLL, JW. All authors read and approved the final draft.
Footnotes
Acknowledgments
The authors would like to thank the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.