
Abstract
BACKGROUND:
Metagenomic next-generation sequencing (mNGS) is a new method that combines high-throughput sequencing and bioinformatics analysis. However, it has not become as popular due to the limited testing equipment and high costs and lack of family awareness with not much relevant intensive care unit (ICU) research data.
OBJECTIVE:
To explore the clinical use and value of metagenomics next-generation sequencing (mNGS) in patients with sepsis in the ICU.
METHODS:
We conducted a retrospective analysis of 102 patients with sepsis admitted to the ICU of Peking University International Hospital from January 2018 to January 2022. Based on whether mNGS was performed, the identified patients were divided into the observation group (
RESULTS:
The testing cycle of mNGS was shorter than that of the conventional culture (30.79
CONCLUSION:
mNGS is useful in the detection of sepsis-causing pathogens in the ICU with the advantages of short testing time and high positive rate. There was no difference in the 28-day outcome between the two groups, which may be related to other confounding factors such as small sample size. Additional studies with extended sample size are needed.
Introduction
With a growing aging population and the increasing incidence of chronic diseases and immunodeficiency diseases, sepsis is a major public health problem worldwide. The morbidity rate of sepsis is over 18 million per year, with a persistent rising tendency annually. The mortality rate of sepsis is as high as 30%, accounting for 20% of deaths worldwide [1]. Sepsis has become the major cause of hospitalization and death in the intensive care unit (ICU) setting [2]. Sepsis refers to a systemic inflammatory response syndrome caused by the invasion of pathogenic microorganisms including bacteria, fungus, viruses, parasites, etc. It manifests as abnormal pathological, physiological, and biochemical functions [3]. Common sites of infection include the lungs, blood, abdominal cavity, central nervous system, urinary tract, skin, and soft tissue. The condition of ICU patients with severe infection is complex, and multiple pathogens or multi-site infections can occur simultaneously leading to a strong inflammatory response and rapid disease progression. It is essential to determine the site of infection at the earliest, identify the characteristics of pathogenic microorganisms and provide appropriate initial anti-infective intervention to achieve successful treatment [4]. One of the most concerning and intractable problems for ICU clinicians is accessing early evidence of pathogenic microorganisms and providing precise anti-infective treatment. Conventional methods of detection mainly include routine blood tests, C-reactive protein (CRP), staining microscopy, conventional culture, and polymerase chain reaction (PCR). However, defects in sensitivity, specificity and periodicity exist in these methods to varying degrees. Moreover, these methods are susceptible to antibiotics, due to which they cannot effectively assist clinicians in the early stage, resulting in failure or delay of initial treatment. It has been reported that unreasonable initial anti-infective treatment is an important risk factor for 30-day all-cause mortality [5], which also leads to antibiotics abuse and microbial resistance, increases the risk of adverse reactions of combined drug use, and foists a heavy economic burden on patients. Therefore, it is crucial to detect pathogens with high specificity, high throughput, and rapid speed. Metagenomic next-generation sequencing (mNGS) is a new method that combines high-throughput sequencing and bioinformatics analysis, which has a high value in the diagnosis and treatment of ICU patients with severe infection [6, 7, 8]. It can not only improve the diagnostic accuracy and guide individualized treatment, but also play an important role in monitoring drug resistance and studying the dynamics of microbial communities. However, it has not become as popular due to the limited testing equipment and high costs and lack of family awareness with not much relevant ICU research data. In this study, we sought to investigate the utility of mNGS in the diagnosis and treatment of sepsis in the ICU.
Materials and methods
General information
We identified a total of 120 patients with sepsis admitted to the ICU of Peking University International Hospital from January 2018 to January 2022. Based on the exclusion criteria, 5 patients with incomplete clinical data, 8 patients with malignant tumors, and 5 patients lost to follow-up were excluded. There were 102 patients with sepsis who were finally included in the study. Among the 102 patients, there were 57 males and 55 females, with age ranging from 22 to 79 years.
Type of infection: There were 15 patients with conventional or perioperative intracranial infection after craniocerebral surgery, with a score of 3–9 points on the Glasgow Coma Scale (GCS), 20 patients with bloodstream infections from various sources, 34 patients with community-acquired or hospital-acquired severe pneumonia, while 21 patients had complicated abdominal infection, 8 patients had urinary tract infections, and lastly, 4 patients had skin and soft tissue infections.
Methods and observation indicators
Inclusion and exclusion criteria
Inclusion criteria: 1) Patients who met the Sepsis-3 diagnostic criteria jointly published by the Society of Critical Care Medicine (SCCM) and the European Society of Critical Care Medicine (ESICM); 2) The source of infection was not clear when admitted to the ICU; 3) Blood culture and mNGS were done simultaneously.
Exclusion criteria: 1) Blood culture and mNGS were not done simultaneously; 2) Sepsis following cardiopulmonary resuscitation; 3) Sepsis in end-stage chronic diseases; 4) Sepsis in malignant tumor; 5) Incomplete clinical data; 6) Prognosis within 28 days was not known.
At present, due to equipment and cost problems in the ICU, mNGS cannot be accepted by family members as a first-line detection method. Most patients refuse to be tested, or accept mNGS detection when the early treatment effect is not ideal. Therefore, the number of sepsis patients who can be tested by mNGS at the same time with other conventional detection methods in the early stage of ICU admission is small, resulting in a low sample size of the experimental group. The sample size of the control group was randomly selected from the patients who met the inclusion criteria according to the data of the experimental group.
This study was approved by the Research and Clinical Trials Ethics Committee of the Peking University International Hospital (No. 2022-KY-0004-01).
Sample collection
mNGS and conventional culture samples were collected within 2 hours after sepsis was diagnosed in the ICU. mNGS blood samples were submitted for testing immediately while conforming to the requirements of genetic testing labs (such as using an exclusive specimen collection tube, following aseptic procedures, and avoiding hemolysis). If samples could not be sent immediately, the samples were stored in a
Observation indicators
Based on whether mNGS was performed or not, the included patients were divided into the observation group (
Statistical analysis
SPSS version 23.0 software was used for data analysis. Continuous variables conforming to normal distribution were represented as mean
Results
Observation group: In terms of gender composition, there were 28 males (54.9%), age was 60 years, APACHE II score was 21. Control group: In terms of gender composition, there were 29 males (56.9%), age was 58 years, APACHE II score was 21. There were no significant differences in general data and type of infection between the two groups (
Clinical characteristics and distribution of infection sites
Clinical characteristics and distribution of infection sites
The reporting time of mNGS was 30.79
Comparison of positive rate and testing time between mNGS and bacterial culture
Consistency evaluation of two test results
Significance of the two detection methods with respect to the type of etiology: mNGS covered all microorganisms such as bacteria, viruses, and fungi, with obvious superiority in viral infections. Among the 51 patients in the observation group, there were 42 patients whose mNGS test results were positive. Among these, bacterial infection accounted for 73.8%, mainly including Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Staphylococcus. At the same time, mNGS also show a good advantage in the detection of bacterial resistance genes. A total of 16 cases of pathogenic bacteria containing drug resistance genes (including 6 strains of Acinetobacter baumannii, 5 strains of Enterobacteriaceae, 3 strains of Staphylococcus aureus and 2 strains of Enterococcus faecium) were reported. The detected drug resistance genotypes included, amongst others, blaOXA-23, blaOXA-51, blaCTX-M, blaKPC, blaZ, mecA, mecR1. Viral infection accounted for 19%, and included human herpesvirus IV (EBV), cytomegalovirus (CMV), and porcine herpesvirus type I. Fungal infections accounted for 7.2%, including Candida albicans (Candida albicans, Candida glabrata, and Candida tropicalis) and Rhizopus microspora. It must be noted that conventional culture cannot effectively identify viruses (Fig. 1).
The positive detection rate of mNGS and culture for different pathogens.
The positive detection rate of mNGS and culture in different specimen types.
mNGS showed a good positive rate in all types of specimens, especially in urine and pus samples with a positive rate of up to 100%. The sensitivity of mNGS in sterile body fluids such as blood and cerebrospinal fluid was significantly higher than that of conventional culture (
The time of optimal antibiotics regimens, the length of ICU stay, and 28-day outcome of the two groups were compared. The time of optimal antibiotics regimens was 48 h in the observation group and 100 h in the control group, showing a statistically significant difference (
Comparison of antibiotic optimization time, ICU hospitalization time and 28-day mortality between observation group and control group
Observation and control group of 28 days survival curve (2).
Comparison of duration stay in ICU and 28-day mortality between negative group and positive group.
Among the 102 patients with sepsis, 28 cases had negative etiological results, including 8 cases in the observation group (5 cases of mixed bacteria and 3 cases of negative mNGS results), 20 cases in the control group had negative culture results, and the remaining 74 cases had positive etiological results. The length of ICU stay and 28-day mortality were compared in patients with negative and positive results. We found that the length of ICU stay was 16.93
Sepsis has become one of the independent risk factors for ICU death, and one of the challenges in treatment in the ICU. Along with adequate fluid resuscitation and organ support, early identification of the pathogens and active and appropriate antibiotics (correct initial treatment
As a novel method for pathogen diagnosis, mNGS has unique advantages in the identification, classification, and detection of drug-resistant mutations and identification of novel pathogens [12]. By extracting nucleic acids from samples obtained from the site of infection, it combines high-throughput sequencing and bioinformatics analysis to realize rapid whole genome (DNA or RNA) sequencing. mNGS can accurately identify bacteria, fungus, viruses, parasites and other atypical pathogens by comparing the sample with the pathogen genome database and analysis [13]. The advantages of mNGS include a short detection cycle, high positive rate, and high specificity. The use of mNGS in infectious diseases has been gradually increasing, especially in rare diseases and infectious diseases with difficulties in definite diagnosis, such as viruses, mycobacterium tuberculosis, anaerobic bacteria, and fungi [14], providing the etiological basis for more targeted drug treatment in patients with severe infections. Because of the unbiased characteristics, mNGS not only covers the genome of microorganisms, but also covers the plasmids carrying drug resistance/virulence genes. While identifying drug-resistant bacteria, the analysis of drug resistance genes can guide the diagnosis and treatment of some patients [15]. However, due to the limited testing equipment, relatively high cost and payment methods, mNGS has not yet become a first-line clinical testing method although the consensus clearly recommends it [16], and is rarely studied in ICU-related research. Therefore, in this study we analyzed and discussed the positive rate of mNGS in different samples and pathogenic microorganisms, and its influence on treatment and prognosis in ICU patients with sepsis.
A total of 102 patients with sepsis were included in this study. Among them, both mNGS and conventional culture were used in 51 patients in the observation group, and only conventional culture was used in 51 patients in the control group. The detection cycle of mNGS was significantly shorter than that of conventional culture (
Eisenmenger syndrome with brain abscess, MDR-AB infection after pituitary cyst surgery and porcine herpesvirus type iencephalitis.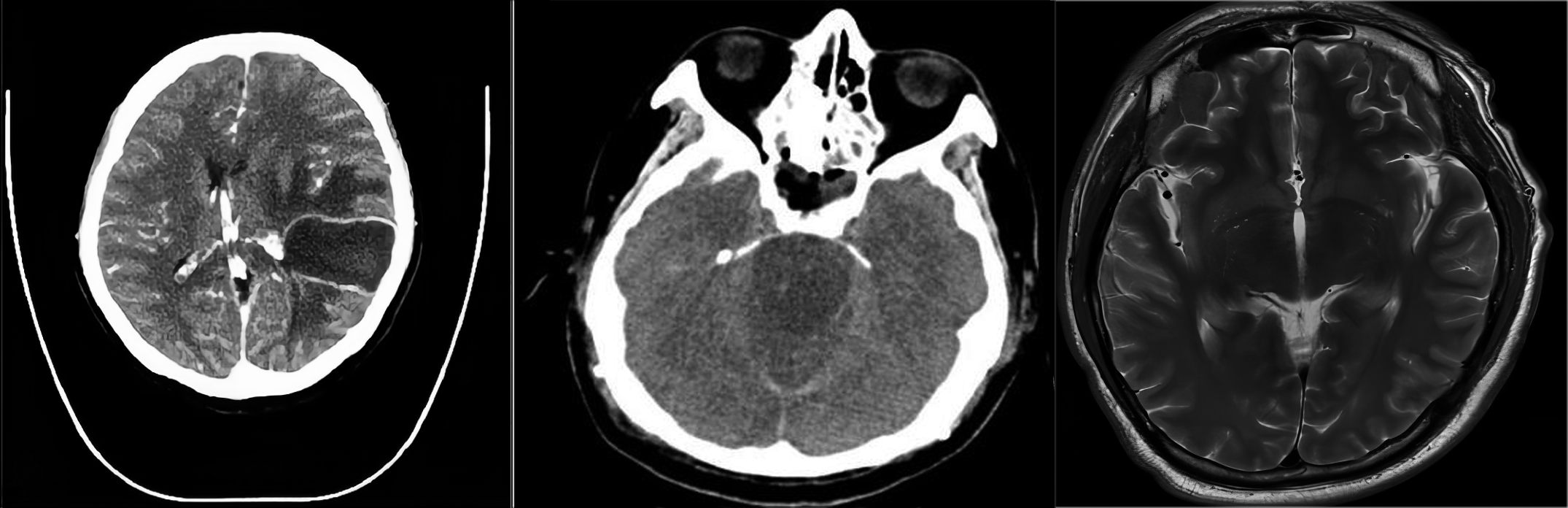
Results showed that the major cause of sepsis in ICU patients in our hospital was severe pneumonia (accounting for about 34%), followed by abdominal infection (accounting for about 21%), and bloodstream infection ranked third (accounting for 18%). On receipt of the positive results, antibiotics were adjusted in time and optimized in both groups. The optimal treatment time was 48 h in the observation group and 100 h in the control group, respectively, with a statistically significant difference (
At present, the rapid development of medical technology and equipment is of great help to clinicians [26], especially in the ICU of major hospitals, with the most advanced and comprehensive diagnosis and treatment equipment, to provide the most accurate diagnosis and treatment monitoring for critically ill patients, as far as possible to help save the lives of patients. although there is a great demand for mNGS monitoring technology in clinical practice, due to reasons such as capital, staffing and technology, there are few mNGS detection equipment in domestic general hospitals. most of them are completed in cooperation with third-party testing institutions with mature and reliable technology and qualification audit, so as to ensure the scientificity of the testing process and the accuracy of the testing results, and eliminate the treatment risk and damage caused by measurement error and uncertainty to patients [27, 28, 29]. The premise of effective application of mNGS detection methods is to select appropriate patients, use appropriate specimens and make reasonable interpretation [30]. It is suggested that it can be used as a first-line detection method in patients with immunodeficiency, severe patients and suspected explosive infectious diseases. At the same time, it is recommended as a supplementary means when the clinical treatment effect is poor and the pathogen infection is unknown. It is recommended to use specimens to select suspected infection sites with high pathogenic microbial load and relatively small impact on non-pathogenic microorganisms, such as alveolar lavage fluid. In addition, the interpretation of mNGS results is very important for us [31]. First, we can refer to the number of sequences of the pathogenic bacteria, but at the same time, we should consider the coverage, specificity and conservation of the sequence on the genome. For pathogenic bacteria that are difficult to detect, even if the number of sequences is low, they can be judged as positive, such as viruses and Brucella. For environmental bacteria and symbiotic bacteria with high sequence numbers, since mNGS cannot distinguish colonization or infection, it is necessary to first exclude conditional pathogenic bacteria by combining pathogens, samples and clinical characteristics.which requires comprehensive judgment or multidisciplinary discussion (ICU, laboratory, pharmacy, infection department). It should be noted that mNGS cannot be used as the only evidence for clinical decision-making. It is also necessary to avoid the failure of clinical treatment due to the wrong interpretation of the results.
As an increasingly sophisticated molecular diagnostic method, mNGS has been widely used in the diagnosis, treatment, and monitoring of infectious diseases in a big way. It has been reported that mNGS can establish a sepsis diagnosis model by integrating host and microbial characteristics, predict the incidence of sepsis, and greatly advance the diagnosis time [32, 33, 34]. At present, mNGS has not been widely accepted by patients and their families due to the limitation of testing equipment and relatively high cost, resulting in the lack of large-sample studies on the use of mNGS in ICU patients and its influence on clinical prognosis [35]. However, it is believed that with mNGS detection technology continuously evolving, in particular, the addition of artificial intelligence technology in the future will help to further improve the efficiency and accuracy of gene detection, while reducing the cost of detection from the side, greater awareness among patients about this technique, it is highly probable that mNGS may become a routine detection method [36]. We recommend that patients with sepsis in the ICU undergo a combination of investigations using mNGS, conventional cultures, other molecular biology, and serological tests to arrive at accurate diagnosis of infectious diseases and obtain better clinical benefits.
With the promotion of mNGS technology, its application value will not only be limited to the diagnosis and personalized precision medicine of patients with severe infection and tumor in hospital, but also be gradually applied to pre-hospital diagnosis and even early prevention and health care [37, 38]. For example, genetic testing is used to understand the genetic susceptibility of individuals to certain diseases, such as cancer and some chronic diseases, so as to carry out targeted health management and reduce the risk of illness. It can help people realize early knowledge, early prevention and early treatment of diseases, and has a certain predictive effect on the development trend of diseases.
In short, mNGS will run through the entire stage of human health management from prevention to treatment, and will also receive the attention of clinicians and more people.
Competing interests
The authors declare that they have no competing interests.
Funding
No external funding was received to conduct this study.
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of the Peking University International Hospital. Written informed consent was obtained from all participants (Approval no. 2022-KY-0004-01).
Footnotes
Acknowledgments
The authors are particularly grateful to everyone who helped them with the article.