
Abstract
BACKGROUND:
During an outbreak such as COVID-19, hospital staff needs to be in close contact with all types of patients visiting the hospital and the risk of cross-infection is extremely high. Payment and medication pickup is a mandatory part of a patient’s hospital visit, with direct contact between healthcare workers and patients, and long waiting times in the hospital area, which can easily lead to the spread of disease infection.
OBJECTIVE:
This paper designed the prototype of a contactless smart medicine cabinet based on RFID technology and optimized the patient consultation and medication pickup process to address these problems.
METHODS:
We conducted a 50-day field observation of patients for consultation and medication pickup at the First Hospital in H city, Jiangsu Province, China, and randomly timed 1600 sets of data from Surgery (ophthalmology) and Internal patients, then we designed the prototype of a contactless smart medicine cabinet based on RFID technology, optimized the patient consultation and medication pickup process, comparing the traditional and intelligent models using AnyLogic.
RESULTS:
The results show that this contactless medicine cabinet was able to reduce the time taken by patients in consultation and medicine pickup by 18.74 minutes, increasing the overall efficiency of the consultation by 32.20%. The simulation revealed that this contactless intelligent medication pickup model was able to reduce the time taken by patients in consultation and medicine pickup, increasing the overall efficiency of the consultation, effectively reducing the frequency of contact between healthcare workers and patients, and reducing the risk of disease infection.
CONCLUSION:
The proposed technical model provides a new idea to solve the problems of long queues, low efficiency and high risk of infection for patients to consult and get medicine during epidemics. Especially within hospitals it has important theoretical and practical implications for epidemic prevention and control as well as future hospital management.
Introduction
The year 2020 saw a major global outbreak of the COVID-19 epidemic. In the early stages of the epidemic, patients flocked to hospitals due to a lack of awareness of the disease, combined with a high number of infections and a shortage of medical resources, a situation that led to outbreaks gathering in hospitals from time to time. With the gradual advancement of prevention and control measures, the epidemic was effectively controlled. However, nowadays, health care workers have to deal with different patients every day in the hospital, and the risk of cross-infection with various diseases for them is extremely high. Particularly, during the severe period of the epidemic, some hospitals were turned into designated hospitals for the treatment of COVID-19, and the demand for medical treatment for residents within the coverage of the designated hospitals was compressed. After the epidemic subsided, the demand for medical care from this segment of the population was released, causing overcrowding in hospitals Although measures such as taking temperature and scanning health codes before entering the hospital can prevent new cases of COVID-19 from entering the hospital to a certain extent, there is still a risk of cross-contamination of diseases due to the overcrowding inside the hospital.
Picking up medication is a necessary part of a patient’s visit to the hospital after treatment. The general flow of medical treatment is that the patient makes an appointment at the hospital, goes to the designated consultation room, is seen by a professional physician, the physician completes the diagnosis and issues a prescription, and the patient pays for the medication. Patients need to queue up to pay for their prescriptions, queue up for their names to appear on the electronic screen in the pharmacy, and then go to the corresponding window to pick up their medications. The whole process takes a lot of time and the queuing process is crowded, with direct contact between patients and patients, and between health care workers and patients. In particular, some patients only need to be prescribed medication but still need to go through the whole process, which can take a lot of time to queue up for medication even without queuing for a consultation. The traditional way of picking up medication for a consultation creates a congregation of people, consuming a lot of time and energy for both healthcare professionals and patients, with a greater risk of cross-contamination of diseases.
Long queues, cumbersome business processes and direct contact between doctors and patients are the main problems in hospital visits, especially in the process of picking up medicines. During the consultation session, doctors need to interact with patients face-to-face. However, in the payment and medication pickup process, information technology can be used to improve the efficiency of the existing business process and achieve quick and contactless medication pickup, which will reduce the waiting time in queues and direct contact between doctors and patients. Information technology has promoted the development of medical health. Advanced medical equipment and technology have provided patients with more accurate and safe treatment plans, and improved the overall management level of hospitals in equipment, drugs, professionals and other aspects [1]. It is very important to ensure the safety of medication for patients during the COVID-19 epidemic. Exploring the relevant methods of drug supply and drug service management in hospitals during the COVID-19 epidemic can provide some experiences for epidemic prevention and control [2]. This study proposes a contactless intelligent medication pickup management model based on RFID technology to address the current problems of patients in the process of medication pickup in hospitals, and designs the smart medicine cabinet, which can effectively optimize the process of patients’ medication pickup and save patients’ waiting time in queues, also reduce crowding and the risk of spreading disease infection. It has important theoretical and practical significance for the prevention and control of epidemics and the improvement of hospital medicine management.
Literature review
Pharmacy pickup is one of the key aspects of drug supply management in hospitals. Inadequate inventory, distribution errors, delays in procurement and dispensing, and poor storage management are common problems in drug management. Wijegunasekara analyzed the drug supply situation in Sri Lanka health care facilities and proposed strategies for it [3], and Kumar adopted the fuzzy AHP method to study the time and cost of public drug distribution in India from the aspects of warehouse design management, supplier selection and others, which provided a reference for pharmaceutical supply chain [4]. Bam et al. used system dynamics to study inventory management and demand forecasting for a tuberculosis drug and proposed three Pareto safety stock management strategies [5], Purwaningsih et al. used ABC and VEN analysis methods to classify diabetes drugs in Insan Permata Hospital, to make rational drug planning and reduce drug shortage [6], while Kees et al. used a mixed-sum integer linear programming model to study the drug procurement and distribution problem in the hospital supply chain [7]. Drug distribution errors can lead to serious consequences, Schwartz and Kravitz conducted a study on clinical pharmacist intervention programs to minimize drug-related errors in clinical medicine [8]. Clinical drug demand is somewhat stochastic and requires certain human and material resources to achieve, Jurado et al. used an opportunity constraint model predictive control approach to meet clinical demand for drugs with limited resources [9], and Abu Zwaida et al. used the deep reinforcement learning model to study the problem of hospital drug inventory management, to solve the drug supply shortage, reduce the cost of drug filling and maximize the profit of hospital supply chain [10]. Lean management has been used more often in inventory supply chain management, and Regattieri et al. implemented lean management of the drug supply chain in the Policlinico Sant’Orsola, the largest hospital in Bologna, Italy [11]. The COVID-19 pandemic has caused a shortage of medical products, prompting countries around the world to urgently authorize the use of essential medical products such as ventilators, personal protection (facemasks) and diagnostic tests made by non-medical companies [12]. The Internet hospital drug delivery platform model is adopted in Jordan during COVID-19, Hammour et al. analyzed the running condition of the platform, which has facilitated patients’ access to prescription drugs during COVID-19 [13]. Current research at the drug supply management level is more likely to look at the problem itself, examining the causes of the problem and proposing appropriate solutions from policy, methodological and strategic perspectives.
RFID, sensors and other core technologies of the Internet of Things have provided new ideas for medication management. Liu et al. proposed a drug distribution management scheme based on the Internet of Things, using RFID electronic tags to record drug information, which can effectively improve the safety of drug distribution and reduce the cost of drug distribution management [14]. Huang and Parida et al. proposed an RFID-based medication management system capable of tracking various types of medications to solve the problem of counterfeit medications and medical errors [15, 16], and Li and Wang proposed a drug anti-counterfeiting traceability scheme based on RFID and blockchain technology, to realize the whole process of drug information traceability from production to sales and circulation [17]. Rayan and Zubair proposed an IoT-Integrated Blockchain pharmaceutical supply chain framework, to strengthen pharmaceutical supply chain management and reduce the occurrence of counterfeit drugs [18], and Jones et al. developed a Ziplock system based on RFID technology to track patients’ medication use, to reduce the occurrence of medication errors or dosage errors [19]. Wu et al. designed an inpatient care medication management system capable of automatically identifying patients and tracking their medication use through RFID tags, making medication safety more reliable [20]. Barcodes have limitations in adverse drug event management due to their small data capacity, and Houliston designed an anesthetic drug identification system based on RFID technology [21]. Adverse drug reactions are a key concern in the process of drug use and management, Jara et al. and Nakhla et al. proposed an IoT-based drug screening system and prevention system [22, 23], while Pérez et al. developed a hybrid intravenous drug administration traceability program based on RFID [24] to reduce the occurrence of adverse drug events in hospitals and improve the safety of patient’s medication use. During patient treatment, medication use requires focused monitoring, and Gupta et al. designed an IoT-based medication monitoring model to monitor the use of available medications in real time [25], while Huang et al. integrated miniaturized spiral antennas, RFID tags and medication libraries to monitor medication doses in real-time [26]. BAINI and ARAMBAWALA evaluated the impact of RFID technology on the safety and traceability of inpatient medication use [27], while Anif et al. proposed an RFID-based hospital medication tracking model-HoMeTrack to track medication use based on prescriptions and patient medical records to reduce medication errors [28]. In addition to the problems of counterfeit drugs, adverse drug reactions and medication errors, the business model of the pharmaceutical supply chain, information transmission mechanism, data collection and tracking are also important directions of concern for related scholars. Liu and Jia used the e3-value methodology to create a value-based business model of the pharmaceutical supply chain based on IoT [29], Yan and Huang proposed an IoT-based supply chain information transmission model for the pharmaceutical industry to solve the traditional pharmaceutical supply chain information transmission lag problem [30]. Meanwhile, Coustasse et al. further clarified the important role of RFID in tracking and managing the entire pharmaceutical supply chain [31], while Jones et al. integrated RFID into hospital pharmacy ERP systems to achieve inventory management of important drugs and vital medical supplies for surgical items [32]. The actual performance of RFID tags of different frequencies in the pharmaceutical supply chain can also vary, Catarinucci et al. evaluated the performance of several commercial UHF RFID tags [33], while the sensing middleware, communication authentication protocols of RFID and the integrated use of technologies such as Bluetooth and barcodes throughout the pharmaceutical supply chain [34, 35, 36, 37] are also key to achieving device management, medication tracking and patient monitoring.
Artificial Intelligence is revolutionizing the healthcare industry, with a wide range of applications in medical devices, drug management and other aspects, but it also raises ethical, privacy and regulatory issues [38]. Telemedicine and artificial intelligence can improve medication adherence, optimize drug therapy regimens, and help medical staff to guide patients to achieve optimal health [39]. Zhao et al. proposed a contactless artificial intelligence framework to detect patients’ errors in the process of drug self-administration and improve drug safety for patients [40]. At the same time, artificial intelligence technology can upgrade the quality management level of drug manufacturers, improve the potential safety problems of drug production effectively, and reduce the safety risks of drugs [41]. Chefchaouni et al. compared and analyzed the differences in human, technical and environmental risks between robotic and manual preparation of anticancer drug modes, to evaluate the role of robots in reducing the risk of drug preparation [42]. Blockchain technology is playing an important role, and has been widely used in the field of pharmaceutical management. The blockchain-based drug supply chain management system enables the monitoring and tracking of drugs at all stages [43], effectively solving the problem of counterfeit drugs and forming an intelligent healthcare ecosystem [44]. The drug tracing and supervision blockchain system-Drugledger proposed by Huang et al. ensures the authenticity and privacy of drug tracing data [45], Kumar and Tripathi use blockchain and encrypted QR (quick response) codes to trace medicines from manufacturer to consumer to address the problem of counterfeit medicines [46]. Smart cabinets have also been used in real-life, Li et al. designed a smart drug management system based on RFID, which consists of a smart monitoring cabinet and microcomputer system, to inventory, query and locate drugs [47], while del Carmen León-Araujo et al. evaluated the effectiveness of smart cabinets using RFID technology to improve cardiac thoracic surgery inventory management and work efficiency and to achieve traceability of medical materials such as drugs [48].
In summary, a series of studies have been carried out in the field of pharmaceutical management, but most of them focus on the entire pharmaceutical supply chain or pharmaceutical management within healthcare, and less on the issue of medication pick-up. In this paper, the main research content is the queuing of medication pick-up in hospitals in the context of the COVID-19 epidemic, combined with RFID technology and smart cabinets, and the previous research results provide the corresponding theoretical and methodological basis for our research work.
Technology and methods
Technology
Radio frequency identification (RFID) technology is the key technology to realizing contactless smart medication pickup management. RFID system mainly consists of RFID tags, an RFID reader and an antenna, its basic principle is by the RFID reader sends a radio frequency signal to activate RFID electronic tag and send out the tag information, RFID reader receives by electronic tag, sends over a modulation signal and transmits to Backstage system for processing, backstage system control RFID reader to complete the corresponding read-write operation, realize to the stationary or mobile to be recognized items automatic recognition [49, 50].
Why choose RFID technology for the prototype design of contactless smart drug cabinets? The main reasons are that: (1) The contactless data communication principle of RFID technology can well meet the technical requirements of smart drug cabinets, and patients can communicate with the drug cabinets by using RFID cards, realizing automatic contactless drug taking and reducing the risk of infection. (2) RFID technology has a very mature application in logistics, warehousing, asset management and other fields, as well as in medical equipment management, drug management and other aspects, forming a relatively rich application scenario, providing a theoretical and method basis for the technology prototype design of smart drug cabinet. (3) RFID electronic tags have low cost, large storage capacity, strong environmental adaptability and repeatability, which can be better adapted to the scene of patients taking medicine in a hospital.
According to the research needs, we choose a 13.56 MHz high-frequency passive electronic tag, this kind of tag has the advantages of small size, long life, read-write fast speed, low cost, various forms of packaging, etc., can be erased many times and has the strong environmental adaptability. In the field of drug management, especially contactless smart medication pickup management, it has obvious application advantages.
Methods
This paper uses a simulation modeling approach to research the problem of patient access to consultation and medication pick up in hospitals. First, we combined the actual situation of patients’ consultation and medication pickup in hospitals, sorted out the consultation and medication pickup business process and constructed a traditional medication pickup model. Second, we designed a smart medicine cabinet based on RFID technology and optimized the patient’s medication pickup business process, and designed a smart medication pickup model based on the prototype of the smart medicine cabinet. Finally, we combined 1600 sets of observations in the target hospital to assign values to the traditional and smart medication pickup models and conducted a simulation study to compare and analyze the time spent on medication pickup by patients in different departments, to further validate the important role of the RFID-based contactless smart medication pickup model in reducing the waiting time of patients in queues for medication pickup and reducing the frequency of contact between healthcare professionals and patients.
Data source
Data collection
In this paper, the first hospital in H City, Jiangsu Province, China, was selected for actual data observation. To improve the reliability of the data, we conducted on-site observations for nearly 50 days in November-December 2021 and randomly timed 1600 sets of data from the waiting for a consultation to the payment and medication pickup for patients attending the surgery (ophthalmology) and internal medicine department. The general outpatient department of ophthalmology was selected for Surgery, and the general outpatient clinics of three small departments that cardiovascular medicine, gastroenterology and endocrinology, were selected for Internal medicine, with comparable volumes of data observed for both departments. The three internal medicine departments that cardiovascular medicine, gastroenterology and endocrinology, had 600 sets of waiting-consultation data, the Surgery (ophthalmology) waiting-consultation data had 600 sets, the payment data had 200 sets, and the medication pickup data had 200 sets each. As the time spent by patients in the waiting-consultation session fluctuated greatly, while the time spent on payment and medication pickup was relatively stable, we chose to observe a large volume of patients in the waiting-consultation sessions of surgery (ophthalmology) and internal medicine department to reduce the impact on the conclusions.
The outpatient clinic hours at Hospital No. 1 in H city are 7:45 a.m. to 11:30 a.m. and 13:30 p.m. to 17:00 p.m., the available appointment slots are 8:00 a.m. to 9:00 a.m., 9:00 a.m. to 10:00 a.m., 10:00 a.m. to 11:00 a.m., 13:30 p.m. to 14:30 p.m., 14:30 p.m. to 15:30 p.m., and 15:30 p.m. to 16:30 p.m., all observations data in this paper are available daily from 7:45 a.m.–11:00 a.m. and 13:30 p.m.–16:30 p.m., coinciding with hospital outpatient hours.
Distinguish between weekdays and weekends, morning and afternoon, the data were divided into three internal medicine departments: cardiovascular medicine, gastroenterology and endocrinology, with 150 groups in the morning and 150 groups in the afternoon on weekdays, and 150 groups in the morning and 150 groups in the afternoon on weekends, making a total of 600 groups. Surgery (ophthalmology) waiting-consultation data is 150 groups in the morning and 150 groups in the afternoon on weekdays, 150 groups in the morning and 150 groups in the afternoon on weekends, for a total of 600 groups. There was no significant difference in the time spent in the payment and medication pickup sessions between weekdays and weekends, and no distinction was made between weekdays and weekends, with 200 separate sets of data observed, for a total of 400 groups. We collation of the data and grouped them as shown in Table 1.
Data collection distribution
Data collection distribution
The various parameter settings in the Traditional consultation and medication pickup model are shown in Table 2.
Parameter setting in the traditional model
Parameter setting in the traditional model
The various parameter settings in the Intelligent consultation and medication pickup model are shown in Table 3.
Parameter setting in the intelligent model
Assuming that the source of patients is not affected by both models, the model is set to arrive at five patients per minute for consultation before and after optimization. The time function for Internal consultation delay was set to triangular (6, 6.5, 7), with the three times in brackets being the average consultation times delay for cardiovascular medicine, gastroenterology and endocrinology respectively. The time function for Surgery (ophthalmology) consultation delay was set to triangular (7, 8, 9), with the three times in brackets respectively the average consultation time delay rounded down, the average, and the average rounded up, the Internal and Surgical (ophthalmology) consultation times unaffected by this two models. The payment delay time of the traditional model is set as the sum of the average payment time and the average queuing time, which is 16 minutes after the measurement of the observed data. The intelligent model adopts manual guidance and reasonable guidance to divert the flow, which could ensure that the flow of people paying at the self-service and manual windows is comparable, and the optimized payment delay time can be set to half of the original. The delay time for medication pickup in the traditional model is set to the average medication pickup delay time of patients, which is 4 minutes after the measurement of the observed data. The delay time for medication pickup after adopting the smart cabinet must be less than the average medication pickup delay time before the optimization, and the medication pickup delay time function is set to uniform (1, 4).
Basic requirements of the experiment
(1) Hardware configuration
CPU: Intel core I5-2520M@2.5G Hz Memory: 16G DDR3 1333MHz
Hard disk: 240G SSD
Motherboard: Intel QM67 VGA Card: Intel HD Graphic 3000 64M
(2) Software configuration
System: Windows 7 Ultimate
Simulation: AnyLogic 8.3 Professional Edition (Evaluation)
Drug smart cabinet design
Smart medicine cabinet model.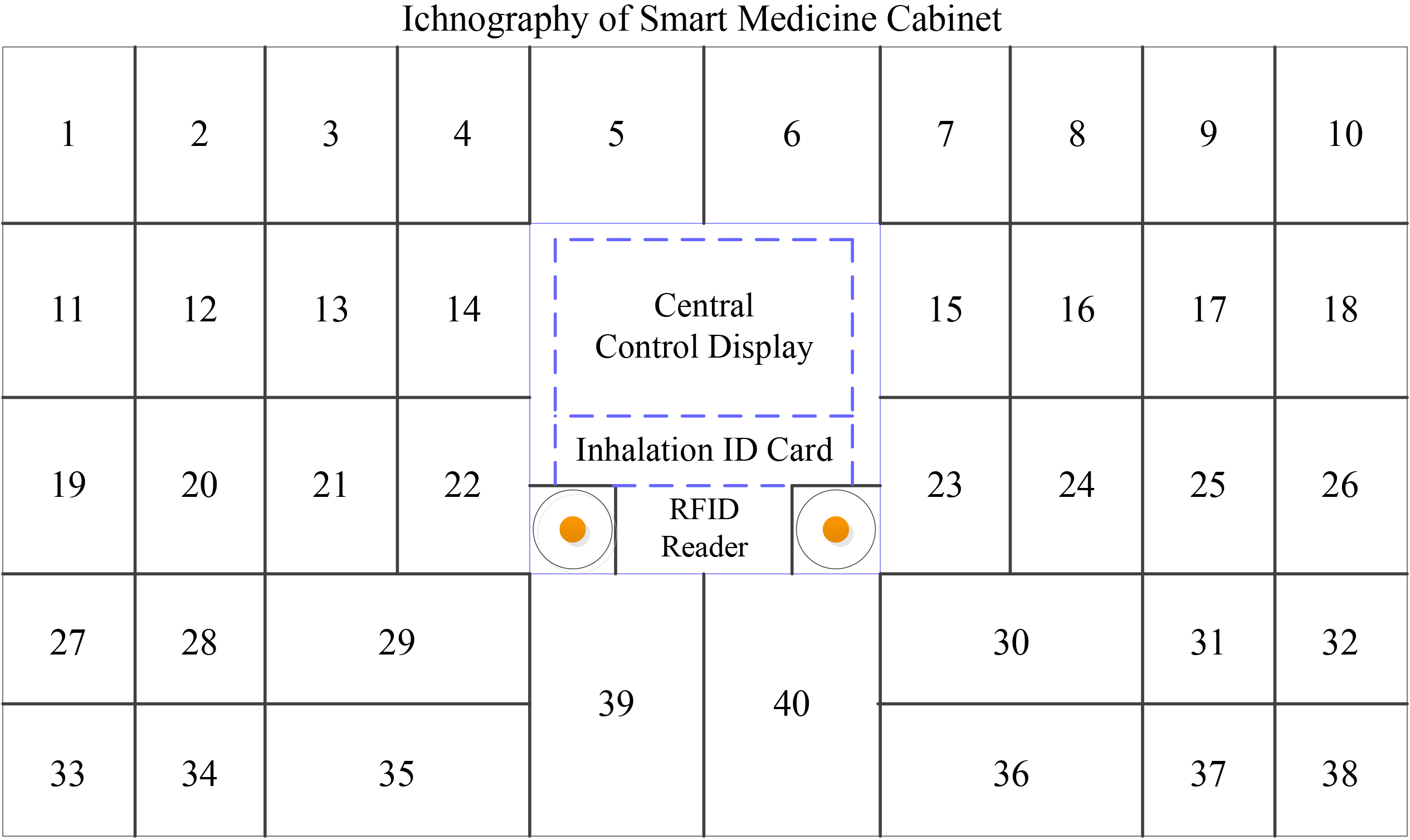
The interface of the smart medicine cabinet is shown in Fig. 1, with a central LCD panel in the middle, Circles are RFID readers and medicine cabinets of different sizes distributed around. After the doctor completes the consultation and treatment for the patient, issues a prescription order for the medicine for the patient who does not need to be hospitalized, and the required medicine information is automatically uploaded to the hospital information system. After the pharmacy receives the dispensing order, the pharmacist will allocate the required drugs in advance and store them in the corresponding drug cabinets. At the same time, the drug information and the coding information of the drug cabinets are automatically uploaded into the hospital information system.
The patient’s personal information, drug information and the corresponding medicine cabinet information are automatically written into the ID card with a built-in RFID tag, while the patient completed payment (manual or electronic self-service payment). The patient holds the ID card to the medicine cabinet, inserts the ID card, the built-in RFID reader of the medicine cabinet reads the ID card information, and the central control screen displays the patient information and medicine information and takes out the medicine after verification. The smart medicine cabinet inserts the card and is designed as an inhalation type, which automatically completes the ID card recycling while reading the card and taking the medicine.
Traditional medication pickup model
(1) Traditional Business model of medication pickup
There are various kinds of departments in the hospital, but the patient consultation process is the same. For ease of analysis, we have divided the hospital departments into Surgical departments and Internal departments, and distinguished between two modes of traditional and intelligent medicine pick-up. The basic business process is patient lift entry, queue for consultation, then queue for payment, queue for medication pickup, and then sequential departure.
Traditional business model of medication pickup.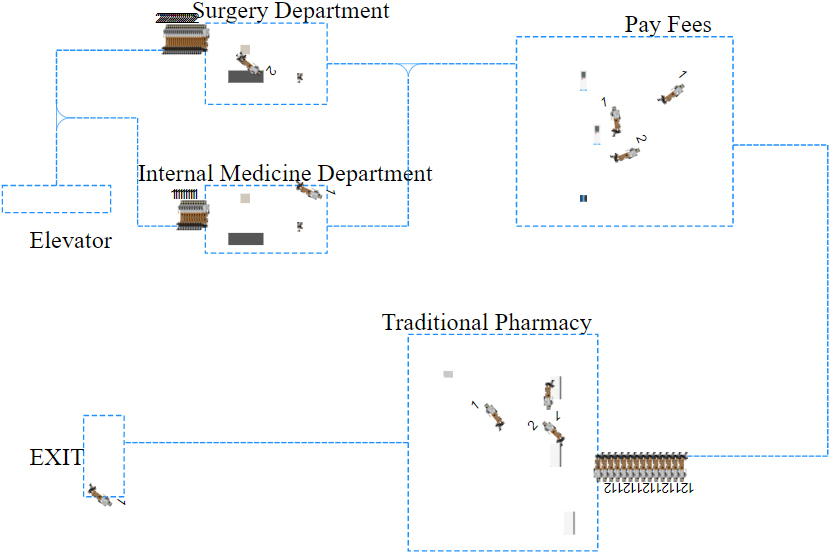
As shown in Fig. 2, patients will enter the room by lift and go to the Internal department or the Surgical department respectively according to their needs. For patients who do not need to be hospitalized, the doctor will issue a drug prescription slip. After completing the consultation, the patient will queue up payment with the drug prescription slip. After completing the payment, the patient will go to the pharmacy with the drug prescription slip and payment slip, where the pharmacist will dispense the drugs according to the prescription slip and the patient will queue up to get the drugs and leave in order after checking.
(2) Traditional business flow chart of medication pickup
Traditional business flowchart.
As shown in Fig. 3, Source1 is the starting point of the traditional consultation and medication pickup process, where patients register and take the lift to the PatientsShunt1 triage table. According to their real personal needs, patients who are registered for internal medicine (labeled 1) queue up in InternalQueue1 for diagnosis and treatment, and patients who are registered for surgery (labeled 2) queue up in OpticalQueue1 for diagnosis and treatment. Only one patient at a time is allowed to be seen by IDoctor1 and ODoctor1, they are in the OpticalQueue1 department and the InternalQueue1 department respectively. After the patient has been seen in the department, the doctor will issue a prescription for medicines for patients who do not need to be hospitalized, the patient will take the prescription MoveTo1 to the payment office and queue for WatingPay1. After payment, MoveTo11 to the pharmacy, give the prescription slip to the pharmacist and queue at the pharmacy window for WatingTake1 to get medication, and then leave the hospital LeftHospital1. The process of medication pickup ends with a Sink.
(1) Intelligent business model of medication pickup
Intelligent business model of medication pickup.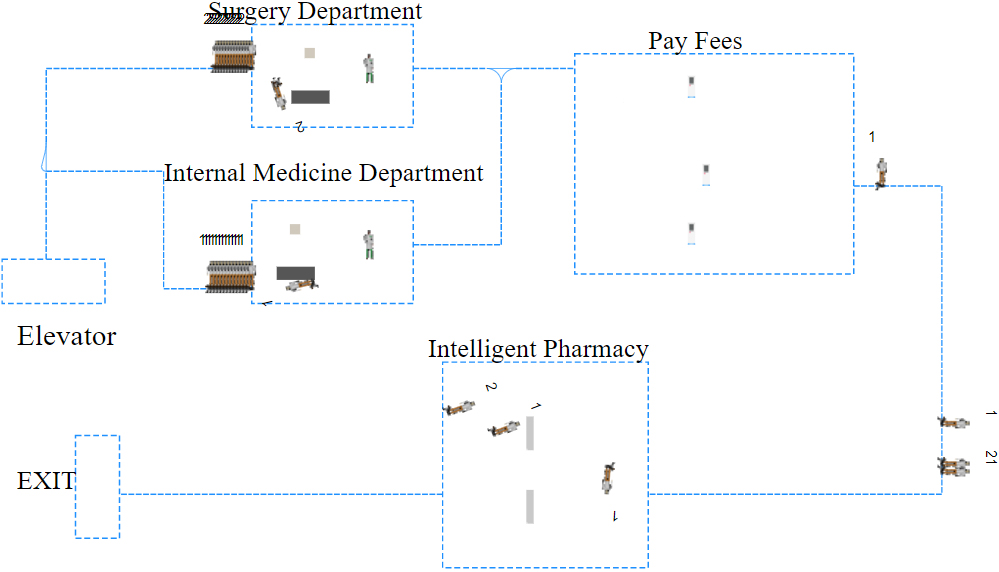
As shown in Fig. 4, the process is the same as that of traditional medicine pickup. Patients go to the internal medicine department or the surgical department respectively, and for patients who only need medicine treatment, the doctor issues a prescription for a medicine according to the disease, and the information on the medicine required is automatically uploaded to the hospital information system and sent to the pharmacy. The pharmacist dispenses the medicine according to the prescription list and places the medicine in the smart medicine cabinet after completing the dispensing, the medicine information and the coding information of the medicine cabinet are automatically uploaded to the hospital information system. Patients take the prescription list and queue up at the payment office to pay the bill or pay from the self-service payment machine. Upon completion of payment, the system will write the patient’s personal information, the corresponding medicine and the medicine cabinet information into the ID card with a built-in RFID electronic tag. After the patient holds the ID card and inserts it into the smart medicine cabinet, the built-in RFID reader of the smart medicine cabinet reads the ID card information and displays the patient’s name and medicine information on the central control display, verifies that the medicine information is correct, the patient will get the medicine and leaves in order.
(2) Intelligent business flow chart of medication pickup
Intelligent business flow chart.
As shown in Fig. 5, Source2 is the starting point of the intelligent medication pickup model process. After completing registration, patients take the lift to the PatientsShunt2 triage table. Depending on the actual need, patients registered for Internal medicine (marked as 1) queue up in InternalQueue2 for diagnosis and treatment, and patients registered for surgery (marked as 2) queue up in OpticalQueue2 for diagnosis and treatment. There are doctors IDoctor1, IDoctor2, IDoctor3 and ODoctor1, ODoctor2, ODoctor3, and ODotcor4 in the internal medicine department and the surgery (ophthalmology) department respectively. A maximum of three patients can enter the internal medicine department and a maximum of four patients can enter the surgical (ophthalmology) department at a time. Once the consultation is completed, the doctor will issue a prescription for medicines for patients who do not require hospital treatment and the prescription will be automatically uploaded to the pharmacy via the hospital information system. Patients hold the drug prescription slip MoveTo2 to the payment office or self-service machine to pay WatingPay2, after payment, they will get an ID card with a built-in RFID electronic tag, the card contains the patient’s personal information, drugs and drug cabinet information. While the patient is paying, the pharmacy has already prepared and placed the medicines required in the smart medicine cabinet. The patient gets the ID card after payment and goes directly to the area where the smart medicine cabinet is located, then the smart cabinet’s built-in RFID reader reads the ID card information and displays the patient’s personal information and medicine information on the central control panel. The patient takes out the medicine in the corresponding smart cabinet and checks with the prescription, after no error, it is confirmed to TakeMedicine, and leaving the hospital LeftHospital2, the process of medication pickup is finished with a Sink.
Traditional model of consultation and medication pickup
Traditional operation model
Traditional operation 3D interface.
The traditional medication pickup model is run to form the interface shown in Fig. 6 running interface shows that the traditional medication pickup model requires long queues for payment and pickup. During an epidemic, people gather and there is direct contact between health care workers and patients, which can easily lead to the spread of disease and infection. At the same time, the queues are time-consuming and labor-intensive, reducing the efficiency of the health care staff.
Time for traditional consultation and medication pickup mode
Time for traditional consultation and medication pickup mode
We divided the hospital departments into the internal medicine department and the surgery department. Patients registered for the internal medicine department (marked 1), 1.1 for the first patient in the internal medicine department, 1.2 for the second patient in the internal medicine department, and so on. For patients registered for the surgery department (marked 2), 2.1 represents the first patient in the surgery department, 2.2 represents the second patient in the surgery department, and so on. To compare the difference in queuing time and efficiency between the traditional and the intelligent consultation and medication pickup models, we assume that 30 patients are selected and form the data table shown in Table 4.
Intelligent operation model
Intelligent operation 3D interface.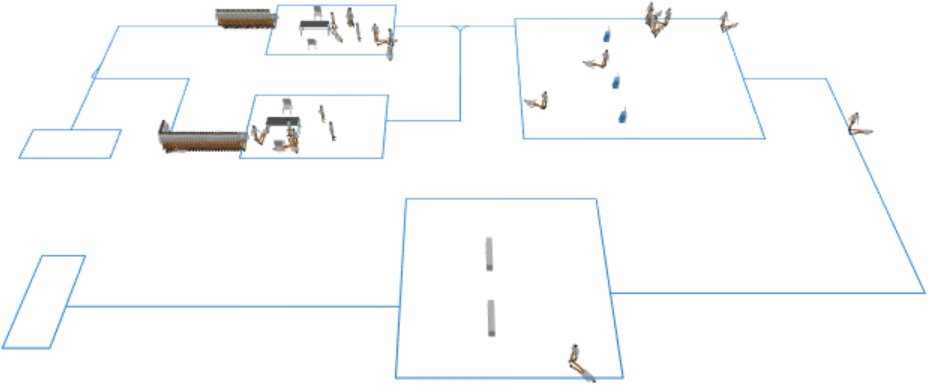
After the intelligent consultation and medication pickup model is run, it forms the interface shown in Fig. 7, the 3D running interface can be seen that the intelligent consultation and medication pickup model is contactless throughout the consultation, payment and medication pickup, except for the queuing process during the consultation, which reduces queuing and gathering of people. This procedure improves the efficiency of hospital consultation, reduces the contact between doctors, nurses and patients, and reduces the risk of disease transmission and infection.
Time for intelligent consultation and medication pickup mode
Time for intelligent consultation and medication pickup mode
To address the problems of traditional consultation and medication pickup and the actual needs of epidemic prevention and control, we designed an intelligent consultation and medication pickup model. It is assumed that 30 patients are selected for consultation, after the simulation model is run, patients registered for the internal medicine department (marked 1), e.g. the first Internal medicine patient ID 1.1, the consultation and medication pickup time is 17.45 minutes, the second Internal medicine patient ID 1.2, the consultation and medication pickup time is 18.00 minutes, and so on. Patients registered for the surgery (ophthalmology) department (marked 2), for example, the first Surgical patient ID 2.1 will take 18.23 minutes to get the medicine; the second surgical patient ID 2.2 will take 17.93 minutes to get the medicine, and so on. The data for the 30 patient consultations and medication pickup corresponding to the traditional model was formed into the data table shown in Table 5.
Synthetic analysis of the internal medicine department
Efficiency analysis of the internal medicine department.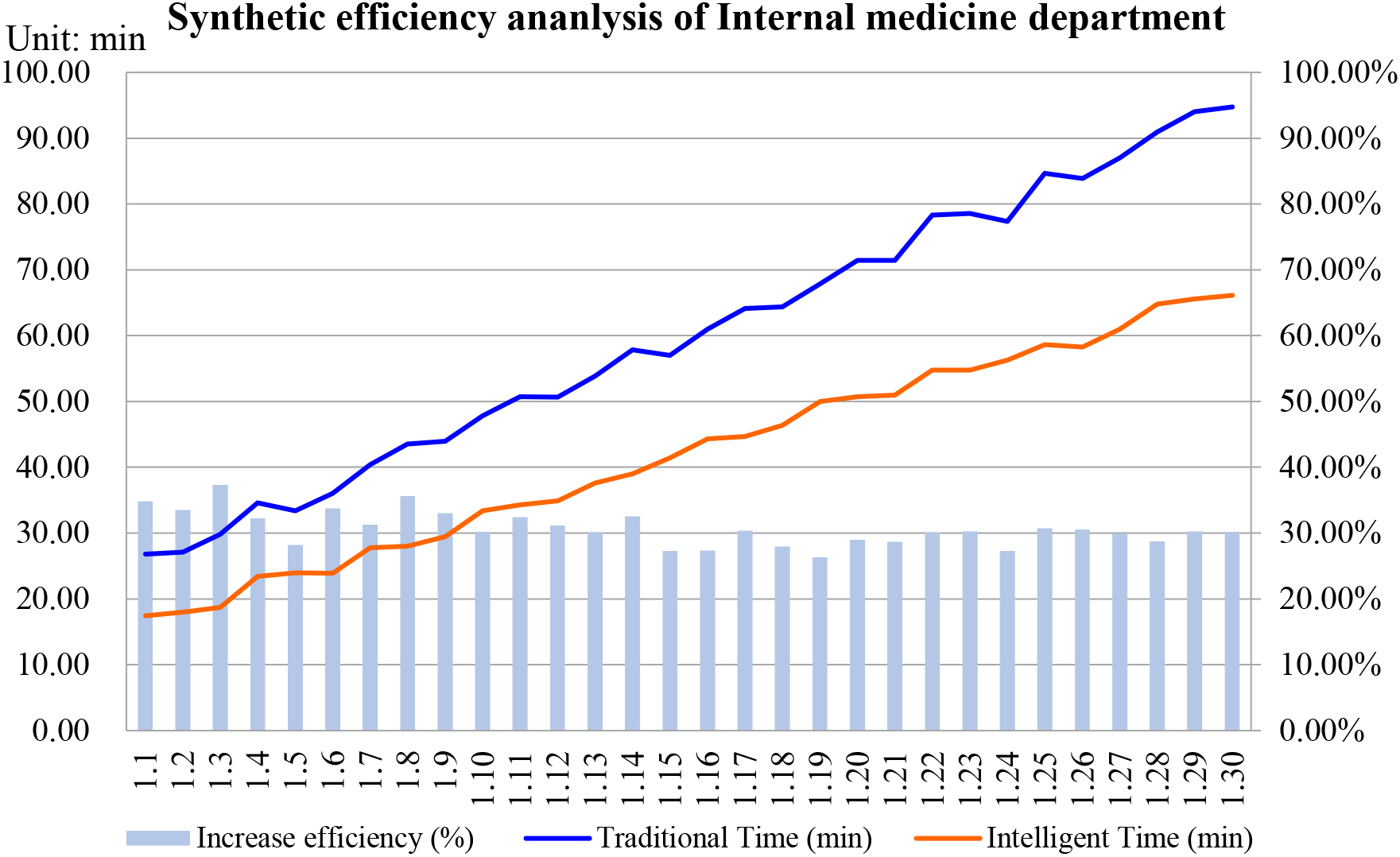
After consolidating the data from the Traditional and Intelligent consultation and medication pickup models, a comparative analysis of the internal medicine patient consultation and medication pickup data is shown in Fig. 8. It can be seen that the time taken to consultation and medication pick-up from 30 internal medicine patients at the hospital was significantly reduced with the adoption of the Intelligent consultation and medication pickup model.
In terms of time, the second patient spent 27.08 minutes in the Traditional consultation and medication pickup model, and 18 minutes in the Intelligent consultation and medication pickup model, reducing time by 9.08 minutes, the least of any of the 30 Internal medicine patients. The 30th patient took 94.72 minutes to complete the consultation and medication pickup with the traditional model and 66.11 minutes with the Intelligent model, reducing the time by 28.61 minutes, the most of any of the 30 internal medicine patients.
In terms of access efficiency, the 19th patient took 67.87 minutes under the Traditional model and 50.02 minutes with the Intelligent model, a reduction of 17.85 minutes and improved the efficiency of consultation and medication pickup by 26.30%, the lowest of the 30 patients. The third patient took 29.84 minutes under the Traditional model, but 18.70 minutes under the Intelligent model, a reduction of 11.14 minutes and a 37.33% improvement in medication pickup efficiency, the highest of the 30 internal medicine patients.
Efficiency analysis of the surgery department.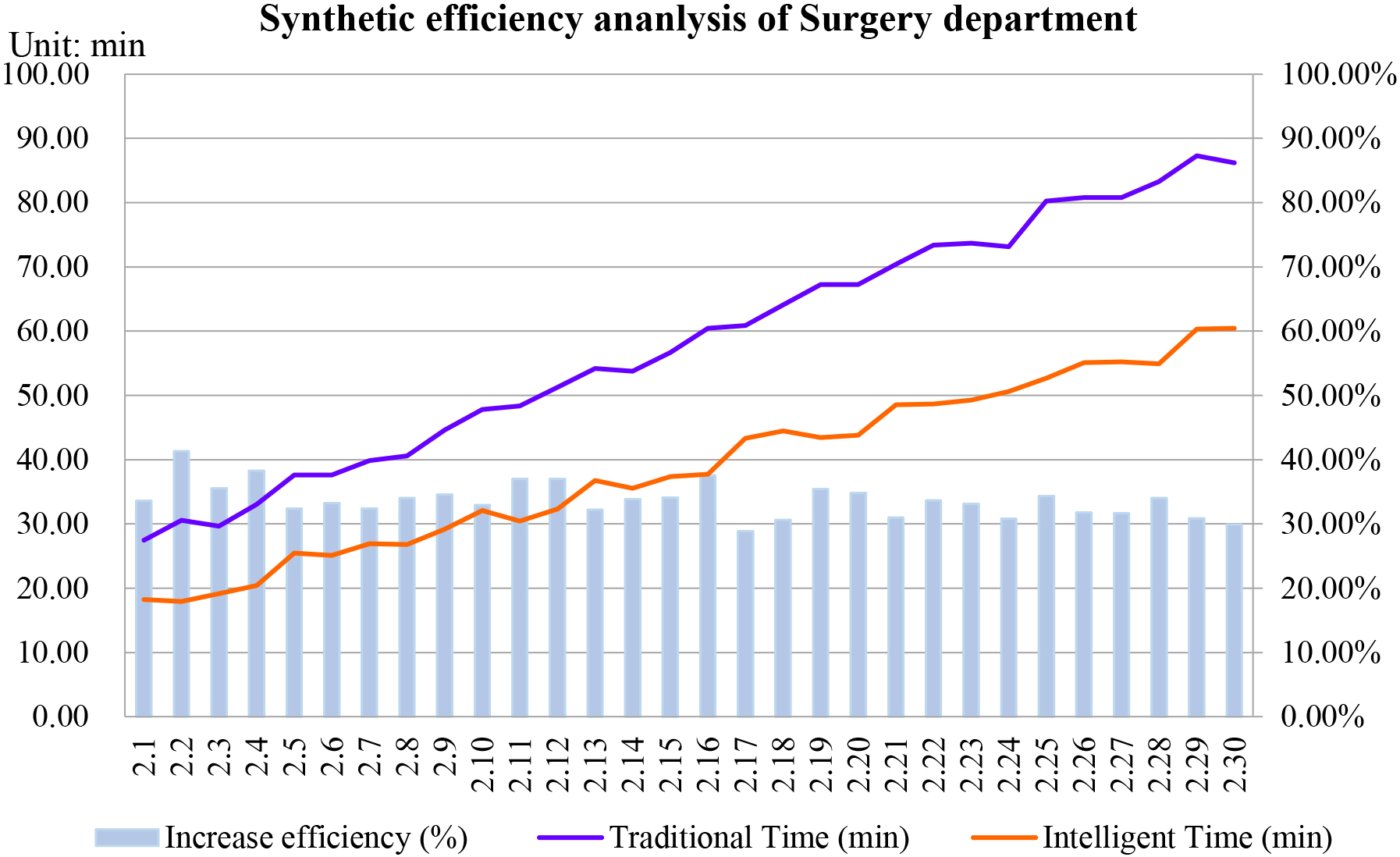
The data for surgical patients in both the Traditional and Intelligent models were combined to contrast the analysis of the consultation and medication pickup data shown in Fig. 9. Consistent with the case of the Internal medicine patients, the time taken to consultation and medication pickup was significantly reduced and the efficiency was significantly improved with the Intelligent model.
In terms of time, the first surgical patient took 27.46 minutes with the Traditional model and 18.23 minutes with the Intelligent model, reducing the time by 9.23 minutes, the least of any of the 30 surgical patients. The 28th surgical patient took 83.28 minutes to complete the consultation and medication pickup with the Traditional model and 54.92 minutes with the Intelligent model, reducing the time by 28.36 minutes, the most of any of the 30 surgical (ophthalmology) patients.
In terms of access efficiency, the 17th surgical (ophthalmology) patient took 60.88 minutes with the Traditional model and 43.32 minutes with the Intelligent model, a reduction of 17.56 minutes and improved the efficiency of consultation and medication pickup by 28.84%, the lowest of the 30 patients. The second surgical (ophthalmology) patient took 30.54 minutes with the Traditional model, but 17.93 minutes with the Intelligent model, a reduction of 12.61 minutes and a 41.29% improvement in medication pickup efficiency, the highest of the 30 surgical (ophthalmology) patients.
(1) Average time of traditional and intelligent
In a combined analysis of 30 internal medicine patients’ consultation and medication pickup data under the traditional and intelligent models, it was found that the total time spent by the 30 patients under the traditional consultation and medication pickup model was 1,802.96 minutes, with an average time of 60.10 minutes. The total time spent under the intelligent consultation and medication pickup model was 1258.40 minutes, with an average time of 41.95 minutes.
Similarly, 30 surgical (ophthalmology) patients spent a total of 1,742.08 minutes in the traditional consultation and medication pickup model, with an average time of 58.07 minutes. In contrast, the total time spent in the Intelligent consultation and medication pickup model was 1162.16 minutes, with an average time of 38.74 minutes.
(2) Average efficiency of traditional and intelligent
With the adoption of the Intelligent consultation and medication pickup model, both internal medicine and surgical patients experienced a significant reduction in consultation and medication pickup time, and a corresponding increase in consultation and medication pickup efficiency. A comprehensive analysis of the data from the Traditional and Intelligent consultation and medication pickup models showed that the consultation and medication pickup efficiency of 30 Internal medicine patients increased by a total of 921.10%, with an average increase of 30.70%. For the 30 surgical (ophthalmology) patients, the total increase in consultation and medication pickup efficiency was 1,010.95%, with an average increase of 33.70%.
Although there was some variation in the time taken between internal medicine and surgical patients, the improvement in efficiency was broadly consistent. As a result, the reduction in time taken between internal medicine and surgical patients was approximately 18.74 minutes with the intelligent consultation and medication pickup model, and the overall efficiency was increased by approximately 32.20%, which is roughly the same as the reduction in total time and improvement in efficiency.
In summary, the use of the Intelligent consultation and medication pickup model for both Internal medicine and Surgical patients resulted in a significant reduction in the time taken to consult and get medicine in the hospital and the efficiency can be increased by more than 30%, meaning that the hospital could treat 130 patients in the time and resources that can originally treat 100 patients. At the same time, the use of the intelligent consultation and medication pickup model can reduce the length of stay of patients in the hospital, reduce the gathering of people and unnecessary queues, and effectively reduce the contact between health care workers and patients during the epidemic, reducing the risk of disease infection, which is of great significance to the prevention and control of the epidemic.
Conclusion
This article investigates the problems of crowding, long queues and low efficiency in the process of patients’ traditional consultation and medication pickup, and designs an intelligent consultation and medication pickup model based on RFID technology and smart medicine cabinets. The main contributions of this article are as follows:
Based on the optimization of the flow of patients’ consultation and medication pickup in the hospital, a traditional consultation and medication pickup model and an intelligent consultation and medication pickup model were constructed. A simulation study was carried out on the patients’ consultation and medication pickup in the two models, distinguishing between internal medicine and surgical patients. The results of the simulation show that internal medicine and surgical patients have different consultation and medication pickup times, but the overall reduction in consultation and medication pickup time and increase efficiency are consistent, with an overall increase in consultation and medication pickup efficiency of approximately 32.20% and the reduction time of approximately 18.74 minutes, it is verified the important role of the intelligent model in reducing the time for consultation and medication pickup, improve the efficiency and reduce the concentration of personnel. Based on the principles of RFID technology, a panel model of smart medicine cabinets is designed to provide a technical prototype for the application of smart medicine cabinets in hospitals in real-life. At the same time, the proposed technical model provides a new idea to solve the problems of long queues, low efficiency and high risk of infection for patients to consult and get medicine during epidemics, and provides a new solution for epidemic prevention and control, especially within hospitals.
However, this article also has certain shortcomings, such as the number of patients attending the hospital and the consultation time can be disturbed by external factors, the input cost of the smart medicine cabinet and the possible economic or social benefits need to be considered comprehensively. In future research, these actual situations will be further considered and more in-depth research will be conducted to address these issues.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grant no. 72274032), the project funded by the China Postdoctoral Science Foundation (Grant no. 2022M710368), the Fundamental Research Funds for the Central Universities (Grant no. N2223033, N2223017), the Humanities and Social Science Research Project of Hebei Education Department (Grant no. BJ2021104), the Natural Science Foundation of Hebei Province (Grant No. G2021501012, G2022501004), and the Social Science Foundation of Liaoning Province (Grant no. L20BXW004).
Conflict of interest
The authors declare that they have no conflict of interest.
Availability of data and material
Data and materials are included in the article.