
Abstract
BACKGROUND:
In malignant tumours of the female reproductive system, cervical cancer is second only to breast cancer, seriously threatening the health and safety of most women.
OBJECTIVE:
To evaluate the clinical value of 3.0 T multimodal nuclear magnetic resonance imaging (MRI) in the International Federation of Gynecology and Obstetrics’ (FIGO) staging of cervical cancer.
METHODS:
The clinical data of 30 patients with pathologically diagnosed cervical cancer admitted to our hospital from January 2018 to August 2022 were analysed retrospectively. Before treatment, all patients were examined with conventional MRI, diffusion-weighted imaging and multi-directional contrast-enhanced imaging.
RESULTS:
The accuracy of multimodal MRI in the FIGO staging of cervical cancer (29/30, 96.7%) was significantly higher than the accuracy obtained in a control group (21/30, 70.0%), with a statistically significant difference (
CONCLUSION:
Multimodal MRI can evaluate cervical cancer comprehensively and accurately to enable accurate FIGO staging, providing significant evidence for clinical operation planning and subsequent combined therapy.
Introduction
In malignant tumours of the female reproductive system, cervical cancer is second only to breast cancer, seriously threatening the health and safety of most women [1]. Squamous cell carcinoma accounts for up to 85% of the pathological types of cervical cancer, with a minority being adenocarcinoma, adenosquamous carcinoma and small-cell neuroendocrine tumours [2]. Clinical research on cervical cancer mainly focuses on early diagnosis, staging diagnosis, treatment selection and prognosis evaluation. Magnetic resonance imaging (MRI), conventional gynaecology, ultrasonography, cytopathology and computed tomography are all used [3]. Because of its excellent soft tissue resolution and the advantages of multiplanar imaging, MRI has been widely recognised as the most effective imaging method for diagnosing and evaluating cervical cancer [4]. In recent years, with the development of modern medical equipment, the dynamic enhancement of MRI means it has been increasingly used to diagnose diseases [2]. Diffusion-weighted imaging (DWI) can differentiate between benign and malignant lesions and predict the invasiveness of malignant tumours by measuring the Brownian motion of water molecules in living tissues to diagnose different diseases [5]. Multi-directional contrast-enhanced MRI can clearly show the morphological and haemodynamic features of lesions [6], and enhanced DWI and MRI are valuable for staging and differentiating cervical carcinoma [5, 6].
Therefore, the present study aimed to compare and analyse the application of conventional MRI and multimodal MRI to determine the clinical value of 3.0 T multimodal nuclear MRI in the International Federation of Gynecology and Obstetrics’ (FIGO) staging of cervical cancer.
Data and methods
General information
The data of 30 cases of cervical cancer confirmed by surgery and pathology or biopsy in our hospital from January 2018 to August 2022 were collected. The age of the enrolled patients ranged from 35 to 83 years, with an average of (57.10
Inclusion and exclusion criteria
According to the criteria defined in the multicentre clinical trial protocol [7, 8], cases of sporadic cervical cancer with complete clinical presentation and data were screened for inclusion in the study group. Inclusion criteria: (1) MRI was performed within three to five days after menstruation in non-menopausal patients. (2) Cervical cancer was diagnosed by biopsy or surgery within seven days after MRI examination. (3) No cervical cancer-related treatment, such as chemoradiotherapy and immunotherapy, was performed before the MRI examination. (4) An informed consent form was signed before the examination. Exclusion criteria: (1) Contraindication to MRI or claustrophobia and failure to complete the whole sequence. (2) Poor MRI image quality due to other reasons. (3) A history of gynaecological surgery, radiotherapy, chemotherapy or immunotherapy.
Examination method
Magnetic resonance imaging examination: Before the examination, the patient was instructed to drink water to fill their bladder appropriately. An indwelling needle was placed in the vein on the back of the hand. The patient assumed a supine position and placed their hands on their forehead. before lying on the MRI bed, to prevent anxiety, it was explained to the patient that the machine would make a particular noise during the examination.
Using a Siemens Spectra 3.0 T Superconducting Magnetic Resonance Imaging system, an eight-channel phased-array surface coil was selected.
Routine MRI scan: T1WI horizontal axis (TSE sequence: TR: 552 ms, TE: 13 ms, THK: 4.5 mm), T2WI horizontal axis (TSE sequence: TR: 3,000 ms, TE: 42 ms, THK: 4.5 mm), T2WI-fs horizontal axis (TSE sequence: TR: 2,400 ms, TE: 42 ms, THK: 4.5 mm), T2WI coronal (TSE sequence: TR: 3,820 ms, TE: 53 ms, THK: 4.5 mm), T1WI coronal (VIBE–Dixon sequence: TR: 4.0 Ms, TE: 2.5 MS, THK: 3.0 mm), T2WI sagittal (TSE sequence: TR: 3,280 ms, TE: 73 ms, THK: 4.5 mm) and T2WI-fs sagittal (TSE sequence, TR: 5,180 ms, TE: 68 ms, THK: 4.5 mm). Between 25 and 40 layers of each sequence were collected.
Diffusion-weighted imaging transverse axis, the value of diffusion-sensitive gradient b
Multi-direction enhancement: After the intravenous injection of contrast agent Gd-DOPA (0.2 ml/kg), the transverse, coronal and sagittal T1WI sequences (VIBE-Dixon sequence: TR: 4.0 Ms, TE: 2.6 ms, THK: 3.0 mm) were scanned in sequence, and 40 layers were collected from each sequence.
Image analysis
A retrospective analysis of pathologically confirmed cervical cancer with conventional MRI plain scan images and assessment of FIGO staging was performed by two experienced deputy chief physicians (with 14 to 15 years’ experience, respectively) in the hospital’s imaging department [9], with the results used as a control group. Three months later, the two radiologists re-evaluated the FIGO staging using conventional MRI, DWI and multi-direction contrast-enhanced images, with the results used as observation data. In the event of a disagreement between the two observers, the determination of the FIGO stage of the images was discussed jointly.
Statistical methods
Measurement data were represented by (
Results
3.0 T MRI multimodal FIGO staging accuracy of cervical cancer
The final clinical stages of FIGO staging were as follows: Stage I (
Overall, the accuracy of the multiple imaging modalities was higher than that of conventional MRI (
Figo staging was performed in 30 patients with conventional MRI and multiple imaging modalities
Figo staging was performed in 30 patients with conventional MRI and multiple imaging modalities
Note: DWI: Diffusion-weighted imaging; MRI: Magnetic resonance imaging.
A 66-year-old woman with irregular vaginal bleeding for more than 4 months. The final clinical FIGO stage was stage IIIC 1. Conventional MRI images 1A (T2WI-FS) and 1B (T2WI) showed unclear small lymph nodes (white arrow) on the right side of the pelvis, which were evaluated as stage FIGO II. In the same slice, Fig. 1C (Dwi) and D (ADC) clearly show two lymph nodes with high signal on DWI and low signal on ADC (White Arrow), which were assessed as stage IIIC1 by multiple imaging modalities.
Female, 80 years old, 30 years menopause, 20 days vaginal bleeding, clinical final FIGO stage I. Figure 2A (sagittal T1WI enhancement), the cervical mucosa outside the mouth linear enhancement intact (white arrow). Figure 2B, (sagittal T2WI plain scan), the cervical canal and the mucosa of the external opening of the cervix showed “T-shaped” high signal (white arrow). The complete enhancement and “T-shaped” sign of the mucosa line of the external opening of the cervix are reliable signs of vaginal non-invasion. This case was evaluated as stage I with conventional MRI and multiple imaging modalities.
63 years old, irregular vaginal bleeding for 30 days, clinical final FIGO stage was stage IIB. Figure 3A (sagittal T1WI enhancement), disappearance of the “T-shaped” sign, interruption of the vaginal mucosal linear hyperintense shadow (white arrow), suggesting an invasion of the upper vaginal segment (stage IIB). Figure 3B (cross-sectional T2WI): the left margin of the lesion was indistinct from the pericervical fat border (White Arrow), with para-cervical invasion (stage IIA), Fig. 3C (coronal T2WI-FS), with the mass extending beyond the cervix (white arrow), and left para-cervical invasion (stage IIA).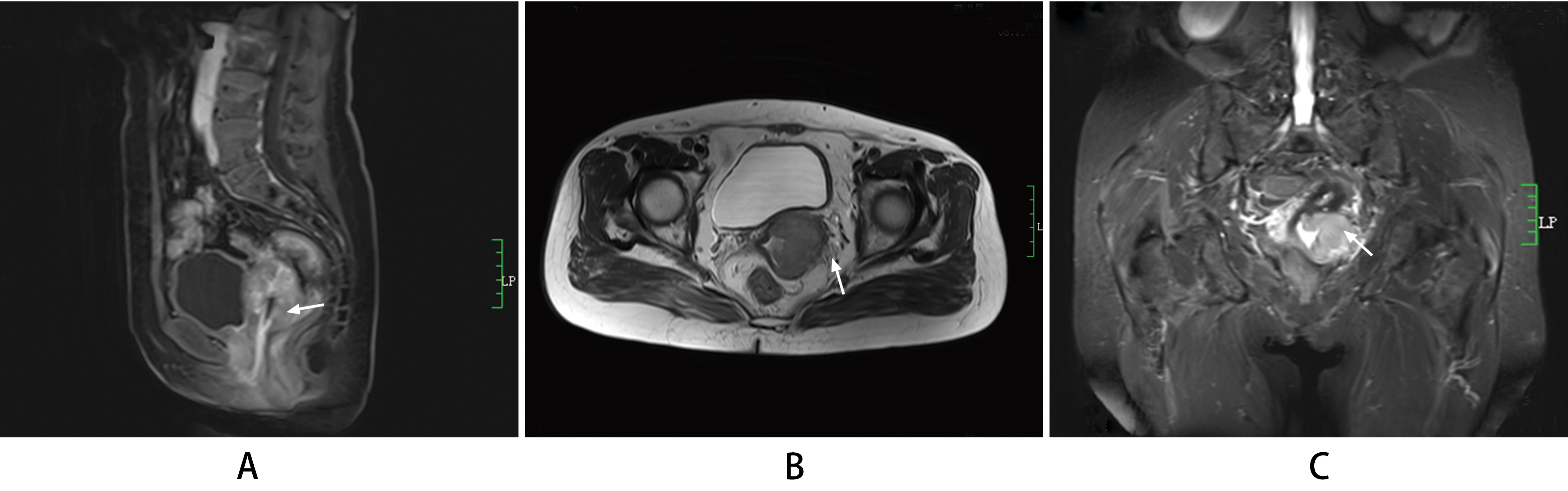
The two physicians did not find pelvic lymph nodes on conventional MRI, and the FIGO staging was Stage II. However, three months later, when the two physicians re-evaluated FIGO using multiple imaging modalities, the DWI layer and apparent diffusion coefficient (ADC) maps clearly showed enlarged lymph nodes; FIGO imaging staging was assessed at Stage IIIC1, and the final clinical FIGO staging confirmed correct FIGO staging with multiple imaging modalities (Fig. 1A–D).
The presence of T1WI-enhanced and intact mucosal line enhancement of the cervical external orifice (Fig. 2A) and the T2WI ‘T-shaped’ sign were reliable indications that the lesion was confined to the cervix, with no vaginal invasion (Fig. 2B).
Enhanced sagittal T1WI (Fig. 3A), axial T2WI (Fig. 3B) and coronal T2WI-fs (Fig. 3C) were combined to assess the extent of paracervical involvement more comprehensively.
Discussion
According to the FIGO 2018 staging principle, FIGO staging divides cervical cancer into clinical, imaging and pathological stages and unifies the criteria [5, 12]; combining clinical, imaging, pathology, etc. enables more effective multi-disciplinary collaboration. A study [13] showed that diagnosing cervical cancer by DWI combined with enhanced MRI significantly improved the sensitivity and specificity of the diagnosis. Consistent with this finding, the present study also found that the addition of DWI and multi-directional enhanced images significantly improved the accuracy and interobserver consistency of FIGO staging for cervical cancer compared with that obtained with conventional unenhanced images (Table 1).
DWI application and cause analysis
Diffusion-weighted MRI is an imaging method that uses MRI to observe the microscopic diffusion motion of water molecules in living tissues [5]. The speed of water diffusion can be expressed by ADC and DWI [14]. Maps of ADC are direct indicators of tissue diffusion and show the slow diffusion of water molecules in tissue, low ADC values, black images, and vice versa. Diffusion-weighted imaging reflects the strength of the diffusion signal; if the diffusion speed is slow, the signal loss is reduced when de-phased, the movement is high, and the image is white [14]. Both DWI and ADC are sensitive to displaying enlarged lymph nodes [14]. In this study, the primary and metastatic lymph nodes of cervical carcinoma were hyperintense on DWI and hypointense on ADC maps, i.e. ADC values were decreased, with good contrast to normal tissues (Fig. 1C and D). Therefore, it is of great importance in FIGO staging. The reason for this is that in cancer cells, growth and division are vigorous, the distribution of tumour cells is dense, nuclei are large, the cytoplasm is thin, and extracellular volume is reduced, limiting the movement of water molecules [15]. In addition, some studies have found that although the ADC values of lesions or lymph nodes in cervical cancer groups decreased, the degree of difference. The ADC values of cervical cancer cells with different pathological types or different degrees of differentiation are significantly different due to the other types of cancer cells volumes, the size and density of the outer space and the additional movement limits of water molecules [16]. Squamous cell carcinoma has a more compact extracellular space than adenocarcinoma, and water molecules are more severely restricted in this tight extracellular space; accordingly, the ADC value of squamous cell carcinoma of the cervix is lower than that of adenocarcinoma [17]. Therefore, the ADC value can further subdivide FIGO staging.
The application and analysis of multi-direction contrast-enhanced imagin
On MRI images, the edge of the lesion is clearly enhanced, which helps increase the contrast of the image against the surrounding normal tissue and improves the display of lesions [6]. The significant enhancement of the cervical and vaginal mucosa was helpful in determining the invasion of the corresponding structures and the staging (Figs 2 and 3). The tumour tissue is rich in blood vessels with different diameters, irregular distribution and rigidity, forming a vascular network of abnormal communications between arteries and veins. In addition, the cellular structural integrity of the vessel wall is poor, the basement membrane is deformed and incomplete – with only one layer of endothelial cells – and the permeability of the vessel wall is increased. After enhancement, the contrast agent enters the cancer focus and shows noticeable enhancement [18].
Key points of cervical cancer staging
Determining whether the vaginal fornix is invaded is a problematic point in FIGO staging, and the presence of a T-shaped sign on T2WI is a reliable indicator of non-invasion of the vagina. Interrupted vaginal mucosal line enhancement is the key to excluding Stage I and assessing Stages II to IV [19].
Diffusion-weighted imaging did not show the anatomic structure satisfactorily, T2WI and coronal T2WI showed the compression of fat well, and T2WI showed a low signal of the muscular layer, which had disappeared. In addition, the peripheral fat was blurred, and coronal T2WI examination revealed a mass protruding from the cervix (Fig. 3B).
Even if the lesion was localised to the cervix, Stage IIIC-1 was seen when pelvic lymph node metastasis was found, with Stage IIIC2 when para-aortic lymph node enlargement was observed (Fig. 1); the latter option involved extended-field full-dose radiotherapy [12], so lymph node enlargement should be evaluated. The staging criteria for inguinal lymph node metastasis are not specified but are included in this article for distant metastasis.
Klerkx [20] found that the sensitivity and specificity of conventional MRI in the evaluation of patients with cervical cancer were 33% and 83%, respectively. Anis Cerovac [21] found that MRI showed higher sensitivity, specificity and accuracy than transvaginal ultrasound in evaluating patients with endometrial cancer (97% vs. 77%; 85% vs. 88%; 90% vs. 83%, respectively). The above studies’ accuracy, sensitivity and specificity are significantly lower than those of this study, indicating that 3.0 T multimodal MRI FIGO has high accuracy in evaluating the staging of cervical cancer.
This study has the following limitations: 1. The sample size was small, only Stages I to IV were statistically analysed, and there was no further statistical research on sub-classifications. 2. No separate classification study was performed for cervical carcinoma with different pathological types and different degrees of differentiation. 3. Diffusion-weighted imaging was the only functional imaging method used from many imaging techniques, so further research on, for example, spectral imaging, dynamic enhancement and perfusion imaging, is required.
Conclusion
DWI and multi-directional enhanced images can significantly improve the accuracy and interobserver consistency of FIGO staging of cervical cancer; compared with using conventional plain scans, the use of multiple imaging modalities is of great value in FIGO staging.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki. Approval was obtained from the Ethics Committee of Sihong County Sub-Jinting Hospital (ID: LKPZ2022035). Written informed consent was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Funding
No funding or sponsorship was received for this study or publication of this article.
Author contributions
(I) Conception and design: PL; (II) Administrative support: SRY and GSF; (III) Provision of study materials or patients: ZY and BYY; (IV) Collection and assembly of data: FWJ and PL; (V) Data analysis and interpretation: ZY, GSF and SRY. All authors wrote and approved the final version of the manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.