
Abstract
BACKGROUND:
Acute appendicitis in children refers to the acute inflammation of the appendix, which accounts for 20%
OBJECTIVE:
This study aimed to establish a decision tree model of complicated appendicitis in children using appendiceal ultrasound combined with an inflammatory index and evaluated its clinical efficacy in pediatric patients.
METHODS:
A total of 395 children admitted to the Emergency Department of the Shanghai Children’s Hospital from January 2018 to December 2021 and diagnosed with appendicitis by postoperative pathology were retrospectively analyzed. According to the postoperative pathology, the children were divided into a complicated and non-complicated appendicitis group, respectively. Routine laboratory inflammatory indicators, including white blood cell count, N(%), neutrophil (Neu) count, Neu/lymphocyte ratio (NLR), C-reactive protein (CRP), and procalcitonin were collected from the two groups. Collecting data on ultrasound examination of the appendix includes whether the appendix diameter is thickened, whether the echogenicity of the mesenteric rim surrounding the appendix is enhanced, whether there is rich blood supply in the appendix, and whether there are fecaliths in the appendix lumen. The risk factors for complicated appendicitis were screened out by univariate and multivariate logistic regression analyses, the binary logistic regression prediction and decision tree models were established, respectively, and the receiver operating characteristic (ROC) curve was used to verify the accuracy of the two prediction models.
RESULTS:
Binary logistic regression analysis showed that CRP, NLR, the presence of an appendicolith, and peripheral retina echo enhancement were independent risk factors for complicated appendicitis in children (
CONCLUSION:
This predictive model, based on ultrasound of the appendix combined with inflammatory markers, provides a useful method to assist pediatric emergency physicians in diagnosing childhood appendicitis. The decision tree model reflected the interaction of various indexes, and the model was simple, intuitive, and effective.
Introduction
Acute appendicitis in children refers to the acute inflammation of the appendix, which accounts for 20%
Several articles have reported the diagnostic value of blood inflammation indicators for the classification and severity of acute appendicitis [5, 6]. Studies have found imaging examinations to be of great value for predicting the classification of appendicitis [7, 8]. Ultrasound examination is fast, convenient, and highly repeatable, and no ionizing radiation is involved. This study adopted a blood routine inflammation index combined with appendiceal ultrasound as a topic and explored its predictive value for acute complicated appendicitis.
Participants and method
Participants
A total of 395 patients who were admitted to the Emergency Department of the Shanghai Children’s Hospital from January 2018 to December 2021 and underwent general appendectomy surgery due to appendicitis were retrospectively studied. The 395 patients included 155 girls and 240 boys aged 28–264 months and a course of disease spanning 0.08–15 days. The course of disease was defined as the time interval from the onset of any clinical symptoms such as fever, anorexia, nausea and vomiting to the first visit to the doctor.
The study’s inclusion criteria were as follows: (1) patients with appendicitis confirmed by pathological examination after an appendectomy; (2) patients who received blood routine (fingertip prick) tests, C-reactive protein (CRP), procalcitonin (PCT), and appendix ultrasound; (3) patients with complete clinical data.
The study’s exclusion criteria were as follows: (1) patients complicated with inflammatory diseases, such as pneumonia and urinary tract infection, and consumptive diseases such as tuberculosis and tumors; (2) patients complicated with immunodeficiency disease; (3) children with chronic appendicitis or acute exacerbation of chronic appendicitis [9, 10, 11].
Grouping
According to the postoperative pathological results, the children were divided into two groups, i.e., the complicated and non-complicated appendicitis groups, respectively. The pathological results after surgery included extensive tissue necrosis or perforation of the muscular layer of the appendix, which suggested that gangrenous and perforated appendicitis be defined as complicated appendicitis. The pathological results confirmed that appendicitis without necrosis or perforation was included in the non-complicated appendicitis group.
Data collection
The clinical data of the children in the emergency department were collected, including age, gender, the course of the disease, symptoms (poor appetite and vomiting), physiological signs (body temperature and muscle tension), and other general data. Muscle tension was determined by palpation of McGomez’s point on the child’s right lower abdomen. Blood test results were collected from the child’s first visit to the emergency department. The blood test results included white blood cell (WBC) count, N[%], neutrophil (Neu) count, neutrophil/lymphocyte ratio (NLR), CRP, and PCT. Additional examination information included the patient’s ultrasound findings on admission (whether the appendix thickening, peripheral retina echo, blood supply, presence or absence of fecalith appears), intraoperative findings, and postoperative pathologic findings. The ultrasound examination is performed by the same sonographer with more than 10 years of working experience, and the final judgment is made by the superior chief physician when the judgment cannot be made (Fig. 1).
a. The appendiceal cavity has widened. The arrow indicates an appendiceal stone with an acoustic shadow; b. The appendiceal cavity widened and the blood supply of the appendiceal wall was abundant.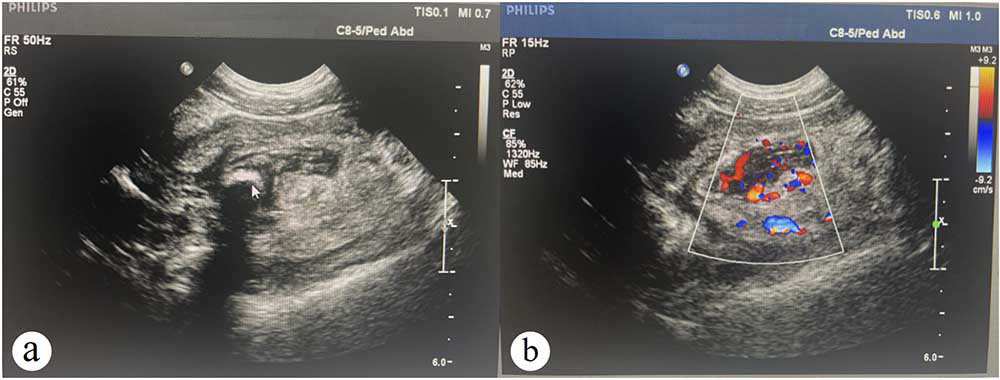
SPSS Statistics 25 (IBM) software program was used to conduct statistical analysis. According to the results of normality test, the measurement data do not follow normal distribution and therefore are represented in the form of median (interquartile) (M [P25 and P75]) range. Enumeration data were expressed as a rate (%) or relative composition ratio (%). For univariate analysis, a Mann-Whitney U rank-sum test was used for non-normality, a chi-squared (
Results
Comparison of the general data
There were no statistically significant gender differences between the two groups (
Comparison of general data of two groups of children
Comparison of general data of two groups of children
Univariate analysis of inflammation index and ultrasound between two groups
WBC, white blood cell; N, neutrophil count; NLR, Neu/lymphocyte ratio; CRP, C-reactive protein; PCT, procalcitonin;
Univariate analysis was performed on the blood routine inflammation index and appendiceal ultrasound index that were included in the study, and the results are shown in Table 2. The WBC, N(%), Neu, NLR, CRP, and PCT results in the complicated appendicitis group were significantly higher than in the non-complicated appendicitis group (
ROC curve calculation results of different inflammatory indexes
ROC curve calculation results of different inflammatory indexes
WBC, white blood cell; NLR, Neu/lymphocyte ratio; CRP, C-reactive protein; PCT, procalcitonin.
ROC curve of CA predicted by different inflammatory indexes including Neu/lymphocyte ratio (NLR), C-reactive protein (CRP) and procalcitonin (PCT).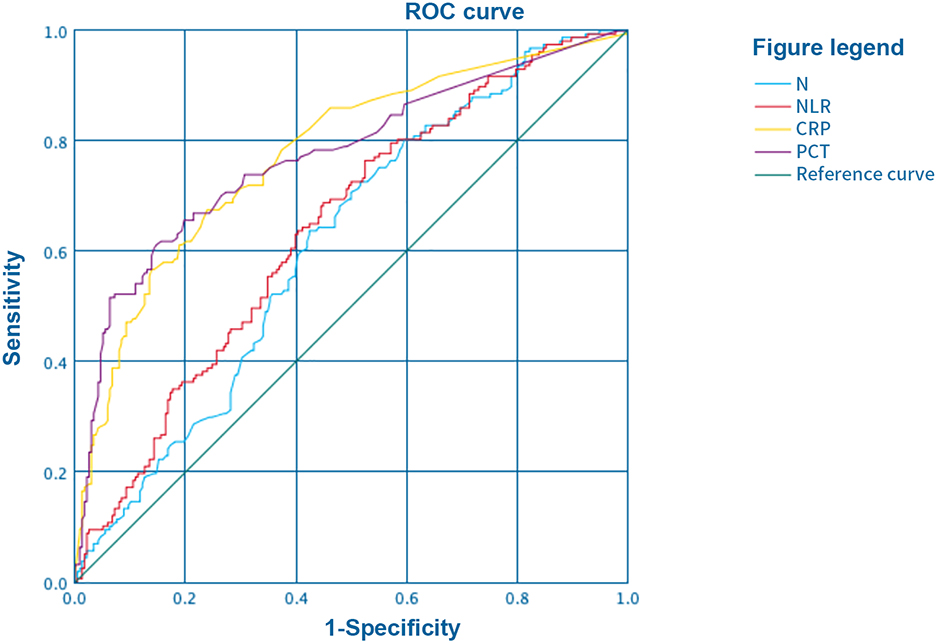
After conducting the collinearity analysis for variables with statistical significance in the univariate analysis, PCT, WBC, NLR, CRP, the presence of an appendicolith, and omental echo enhancement indexes in the area of the appendix were included for multivariate logistic regression analysis with the type of appendicitis as the dependent variable (assignment, non-complicated appendicitis
Multivariate logistic regression of effects of various indexes on types of acute appendicitis
Multivariate logistic regression of effects of various indexes on types of acute appendicitis
WBC, white blood cell; NLR, Neu/lymphocyte ratio; CRP, C-reactive protein; PCT, procalcitonin.
The decision tree model was applied in the SPSS Statistics 25.0 software program with complicated appendicitis (no
Decision tree of appendiceal ultrasound combined with inflammation index (C-reactive protein, CRP).
The AUC values of the decision tree model and the binary regression model were 0.809 and 0.823, respectively. The sensitivity of the logistic model was high, and the specificity and accuracy of the decision tree model were higher than those of the logistic model, suggesting that both had good application value for complicated appendicitis prediction with high accuracy (see Table 5 and Fig. 4).
ROC verifies results of CA prediction by decision tree model and logistic model
ROC verifies results of CA prediction by decision tree model and logistic model
ROC curve of CA predicted by decision tree model and logistic model.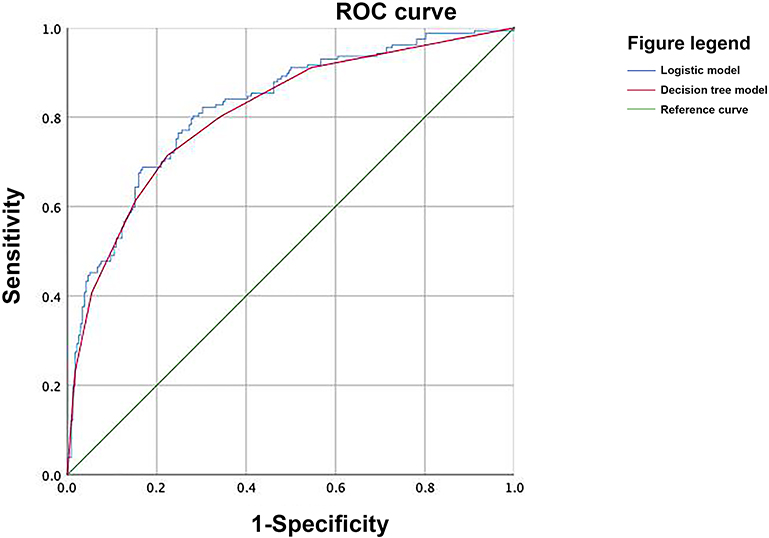
Appendicitis in children can progress rapidly. It has been reported in the literature that perforation of the appendix in children accounts for 12.7%–32.5%. Following perforation of the appendix, the incidence of complications, hospital stay, and re-hospitalization rate increased significantly [12]. At present, surgical resection is an important treatment approach for acute appendicitis, but complications such as intestinal obstruction, incision infection, and abdominal abscess, as well as the negative resection rate in cases of appendicitis following an appendectomy, are among the concerns of this approach shared by clinicians. Studies have found the effect of conservative treatment (e.g., antibiotics) on patients with non-complicated appendicitis to be precise [13]. An appendectomy does not deliver benefits in terms of reducing complications or shortening hospital stay [14]; as such, for pediatric patients, it is necessary that complicated appendicitis be identified promptly and followed up by the appropriate treatment.
To date, several studies have been conducted on the application of appendix ultrasonography and inflammatory indexes for predicting complicated appendicitis, both at home and abroad. A retrospective analysis of 794 children with acute appendicitis by Rawolle et al. [15] showed that appendix thickening, fatty inflammation around the appendix, and an appendix appendicolith were independent risk factors for predicting complicated appendicitis [16, 17, 18]. A study conducted by Nijssen [19] involving 176 children showed that the sensitivity of ultrasound for predicting complicated appendicitis was too low and could not be used as an independent prediction method.
A total of 395 children were included in the present study. The univariate analysis found significant differences in peripheral retina echo results and for the presence of an appendicolith between the two groups. Additionally, the binary logistic regression analysis found that omental echo changes near the appendix and the presence of an appendicolith were independent risk factors for complicated appendicitis; the ORs were 2.590 and 2.037, respectively, which had good predictive value and were consistent with Rawolle’s conclusion [15].
Inflammatory indexes can be used to evaluate the occurrence of infectious diseases. Presently, the predictive role of WBC, CRP, PCT, and NLR in complicated appendicitis is receiving more research attention. A study by WeiFeng et al. [20] showed that CRP, PCT, and Neu were significantly different in cases of complicated appendicitis when compared non-complicated appendicitis cases. Zani [21] posited that WBC and CRP could better predict the occurrence of complicated appendicitis in children above the age of 5 years old. The results of this study showed that when the CRP cut-off value was set to 25.5 mg/L, the sensitivity for predicting complicated appendicitis was 67.5% and the specificity was 76.1%, which was similar to the results of existing studies.
Research has also indicated NLR as an independent risk factor for complicated appendicitis [22]. In the data analysis of the present group, NLR was used to predict complicated appendicitis with an OR of 1.070, sensitivity of 76.4%, specificity of 47.5%, as well as low sensitivity; the results suggested that NLR on its own was inefficient for predicting complicated appendicitis. A meta-analysis showed that the comprehensive sensitivity of PCT in the diagnosis of complicated appendicitis was 89%, and comprehensive specificity was 90% [23]. However, the results of the current study showed that, with a cut-off value of 0.44 mg/ul, the sensitivity and specificity of PCT for predicting complicated appendicitis were 61% and 78.4%, respectively. The sensitivity was low in this instance and, overall, its ability for predicting complicated appendicitis on its own remained limited.
Zachos et al. [24] studied a combination of various inflammatory indexes that failed to show good prediction value for complicated appendicitis. The AUCs of the decision tree model and the binary regression model, which was established when NLR and CRP were combined with appendiceal ultrasound in the present study, were 0.809 and 0.823, respectively, with high sensitivity and specificity, indicating high diagnostic and predictive value and high clinical predictive efficiency. Using the decision tree model map, the echo in the region of CRP, appendicolith, or the appendix itself was enhanced, with strong interactivity. This study summarized the clinical independent risk factors of complicated appendicitis in children, which is helpful for clinicians to concentrate on screening key indicators in the process of diagnosis and treatment. Meanwhile, the decision tree model of this study provided clinical diagnosis and treatment ideas. Visualized research results can also help clinicians quickly reference and make clinical decisions in practice. Therefore, the result of this study is a conclusion with practical application value.
The current study has some limitations. First, its sample size was small, which limited the generalizability of the conclusions. Therefore, further verification of its results is required by conducting large-sample studies. Second, too few indexes were included in the appendiceal ultrasound. For example, the thickness of the appendiceal wall was excluded; therefore, conclusions on the predictive value of appendiceal ultrasound may not be sufficiently comprehensive, which can be addressed in future prospective clinical observations.
Conclusion
A decision tree model, based on a laboratory inflammation index combined with appendiceal ultrasound, could more intuitively and vividly predict the occurrence of complicated appendicitis. Compared with the logistic regression model, the decision tree model did not only reflect better interaction between different variables but could also intuitively compare the impact intensity of various factors on the occurrence of complicated appendicitis. Combining these factors (the most influential factors for complicated appendicitis) using a flowchart-style interface can assist clinical physicians in predicting the occurrence of complicated appendicitis in a timely manner, thereby improving the clinical outcomes of complicated appendicitis patients.
Competing interests
The authors declare that they have no competing interests.
Funding
No external funding was received to conduct this study.
Availability of data and materials
All data generated or analysed during this study is included in this article. Further enquiries can be directed to the corresponding author.
Ethics statement
This study was conducted with approval from the Ethics Committee of the Shanghai Children’s Hospital (2022R085-E01). This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was waived because of the retrospective nature of this study.
Clinical registration
The study was registered on www.chictr.org.cn on 29/06/2022 under registration number ChiCTR22000 61580.
Footnotes
Acknowledgments
We would like to acknowledge the hard and dedicated work of all staff that implemented the intervention and evaluation components of the study.