
Abstract
BACKGROUND:
Diarrhea is a prevalent complication after renal transplantation.
OBJECTIVE:
To examine the risk factors for diarrhea after renal transplantation, evaluate their combined predictive values, and analyze the prognosis.
METHODS:
Clinical data of patients who underwent allogeneic renal transplantation in the Second People’s Hospital of Shanxi Province from January 2019 to March 2020 were retrospectively analyzed, cases were screened and grouped, independent risk factors for diarrhea after renal transplantation were analyzed by univariate analysis and multivariate analysis, and their predictive value was evaluated by receiver operating characteristic (ROC) curve. The survival time of recipient grafts in diarrhea and non-diarrhea groups were evaluated by Kaplan-Meier and log-rank test.
RESULTS:
We included 166 recipients in the study and the incidence of diarrhea was 25.9%; univariate and logistic regression multivariate analyses revealed that independent risk factors for diarrhea in recipients were that the type of renal transplant donor was DCD (donation after circulatory death), immunity induction was onducted with basiliximab
CONCLUSION:
Diarrhea affected the two-year survival rate of the graft. The type of donor, immunity induction scheme, and the type of MPA and DGF were independent risk factors for diarrhea in recipients, and the combination of the four factors had good prognostic prediction value.
Introduction
Renal transplantation is one of the effective treatments for end stage renal disease (ESRD). In recent years, the quality of life of patients has been significantly improved with the development of renal transplantation. However, postoperative complications remain an essential factor plaguing the long-term survival of renal transplantation recipients [1]. Diarrhea is a prevalent complication after renal transplantation [2], and poor gastrointestinal symptoms after renal transplantation significantly reduce the quality of life of renal transplantation recipients [3]. Therefore, it is vital to predict diarrhea after renal transplantation and take early and effective interventions.
In this study, we collected clinical data of renal transplantation recipients who were followed up for more than two years in the Second People’s Hospital of Shanxi Province. We established appropriate inclusion and exclusion criteria, and analyzed the general conditions of renal transplantation recipients, possible clinical indicators related to diarrhea, and risk factors for diarrhea after renal transplantation, their predictive value, and their prognosis, to better predict and manage diarrhea after renal transplantation.
Material and methods
General data
Clinical data from 181 patients who underwent allogeneic renal transplantation in the Second People’s Hospital of Shanxi Province from January 2019 to March 2020 were collected, and the inclusion and exclusion criteria were set. Inclusion criteria: (1) patients who underwent allogeneic renal transplantation for the first time; (2) patients who were followed up for more than two years; (3) patients who met the diagnostic criteria for diarrhea in this study; exclusion criteria: (1) patients who were under 18 years old; (2) patients who received multiple organ transplantation (MOT); (3) patients with incomplete data and who were lost to follow-up; (4) patients who developed diarrhea due to a history of gastrointestinal disease before operation.
Among the 181 patients, 15 were excluded, 2 underwent secondary renal transplantation, 1 underwent tertiary renal transplantation, 3 were under 18 years old, 1 underwent transplanted kidney resection due to hyperacute rejection 20 h after the operation, 1 died of cardiac arrest four days after the operation, 1 died of aortic dissection one year after the operation, 1 had a history of ulcerative colitis before the operation, and 5 had incomplete follow-up data. The remaining 166 patients (including all inpatients and outpatients with diarrhea) were retrospectively analyzed.
Diagnostic criteria for diarrhea
Based on the diagnosis criteria of diarrhea in the Guidelines for Diagnosis and Treatment of Digestive Diseases (Edition 3) – increase in the frequency of bowel movements and thin stools, containing mucus, blood, pus, or undigested food.
Causes of diarrhea
The factors causing diarrhea include infectious factors, immune factors, and intestinal flora imbalance caused by long-term use of antibiotics. Infectious diarrhea can be caused by a variety of pathogenic microorganisms, such as bacteria, viruses, fungi, parasites and so on. We did not perform a detailed analysis of the causes of diarrhea, since the majority of patients were outpatients and we did not have clear etiologic evidence.
Preoperative treatment for infection prevention
All patients undergoing allogeneic renal transplantation were given piperacillin/tazobactam from the day of the operation to two weeks, to prevent bacterial infection, ganciclovir from 10 days after the operation to 3 months, to prevent viral infection, and compound sulfamethoxazole from 14 days after the operation to 6 months, to prevent Pneumocystis carinii infection. In addition, DCD renal transplantation recipients were given Caspofungin from the day of the operation to 10 days after the operation to prevent fungal infection.
Study content
Leading indicators of patients were collected, univariate and multivariate analyses were conducted on the risk factors for diarrhea in renal transplantation recipients, and their predictive value was evaluated. Leading indicators included: age, gender, body mass index (BMI), preoperative dialysis method, preoperative dialysis time, type of donor, immunity induction scheme, type of calcineurin inhibitor (CNI), type of mycophenolic acid (MPA), the occurrence of delayed graft function (DGF), the occurrence of acute rejection (AR), and others, of which the preoperative dialysis method included blood dialysis and peritoneal dialysis; the type of donor included DCD and living-related donors; the immunity induction scheme included basiliximab alone, anti-thymocyte globulin (ATG) alone and basiliximab
Statistical methods
Statistical analysis was conducted using the SPSS 26.0 software. Measurement data in normal distribution are expressed as mean
Results
Univariate analysis of risk factors for diarrhea after renal transplantation
Among the 166 patients, 43 had diarrhea and 123 did not. The incidence of diarrhea was 25.9%. The univariate analysis showed statistical differences between diarrhea and non-diarrhea groups in the type of donor, immunity induction scheme, type of MPA, and the occurrence of DGF (all
Comparative analysis of baseline information on risk factors for diarrhea after renal transplantation
Comparative analysis of baseline information on risk factors for diarrhea after renal transplantation
Note: BMI: body mass index; ATG: antithymocyte globulin; CNI: calcineurin inhibitor; MPA: mycophenolic acid; DGF: delayed graft function; AR: acute rejection.
Variables were included in the logistic regression multivariate analysis with
Multivariate analysis of risk factors for diarrhea after renal transplantation
Multivariate analysis of risk factors for diarrhea after renal transplantation
Note: ATG: antithymocyte globulin; MPA: mycophenolic acid; DGF: delayed graft function; OR: odds ratio; CI: confidence interval.
Based on the results of binary logistic regression analysis, ROC curves were drawn for the type of donor, immunity induction scheme, type of MPA, the occurrence of DGF, and the predictive scheme of the combination of the four factors (Fig. 1).
Comparison of classification effect of predictive schemes
Comparison of classification effect of predictive schemes
Note: MPA: mycophenolic acid; DGF: delayed graft function; AUC: area under the curve; CI: confidence interval.
Predictive value of combined predictive factors for diarrhea after renal transplantation.
ROC curve results showed that the area under the curve (AUC) of the combination of the four predictive factors in predicting diarrhea after renal transplantation was the highest, which was 0.822 (the 95% CI was 0.754–0.890), the critical value was 0.171, the sensitivity was 0.814, the specificity was 0.65, and the Youden’s index was 0.464 (
Among the 43 patients with diarrhea, they were treated with anti-infection, rehydration, antidiarrheal, adjustment of intestinal flora, and adjustment of immunosuppressive agents, and their conditions were improved, and the duration of the disease was not more than 2 weeks. Due to the strong dependence and vigilance of patients in follow-up after renal transplantation, only 5 patients had hypokalemia and 3 patients had Acute Kidney Injury (AKI) among 43 patients with diarrhea. Hypokalemia was diagnosed as serum potassium
Analysis of survival time of recipient grafts in two groups
All 166 patients were followed up for 0–37 months after the operation, with a median follow-up time of 22 months. The two-year survival rate for grafts in the 166 patients after renal transplantation was 96.9%, with 5 dysfunctional grafts. The log-rank survival statistical results indicated that the graft survival rate two years after the operation in the diarrhea group was significantly lower than that in the non-diarrhea group (82.5% vs. 97.8%,
Analysis of graft survival two years after operation in the two groups.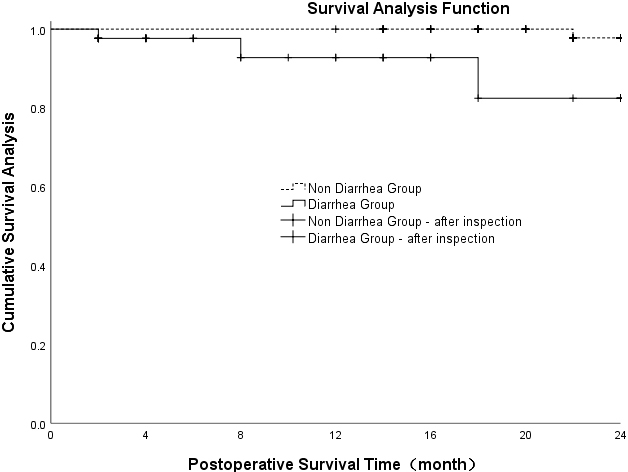
Incidence and prognosis of diarrhea after renal transplantation
Diarrhea is a crucial factor influencing the quality of life and long-term survival of renal transplantation recipients. According to a study that analyzed the medical insurance claim records from the United Network for Organ Sharing (UNOS), the incidences of diarrhea one, two, and three years after renal transplantation were 11.5%, 17.5%, and 22.6%, respectively [4]. In another survey of 4,232 Scandinavian renal transplantation recipients, the incidence of diarrhea was up to 53%, while their doctors estimated only 6.9% [5]. Poor gastrointestinal symptoms after renal transplantation significantly reduce the quality of life of renal transplantation recipients. According to the diagnostic criteria of diarrhea in the Guidelines for Diagnosis and Treatment of Digestive Diseases (Edition 3), in this study, we statistically analyzed the incidence of diarrhea after renal transplantation was 25.9%. The follow-up duration was more than two years. The postoperative follow-up indicated that the survival rate of grafts two years after the operation in the diarrhea group was significantly lower than that in the non-diarrhea group.
Meanwhile, we tried to analyze the statistical significance of the recipient survival rate after renal transplantation in diarrhea and non-diarrhea groups, finding that the two-year survival rates after the operation in the two groups were 100%. The main reasons were that the follow-up duration was short, the sample size of the study was small, and the study was a single-center study that lacked the analysis of more data from other centers. We collected multiple and large sample data and prolonged the follow-up duration to evaluate the incidence of diarrhea after renal transplantation, the changes in trend, and the prognosis of the transplanted kidney with diarrhea.
Independent risk factors for diarrhea after renal transplantation
Type of donor
Before 2015, the type of donor for renal transplantation in China included cadaveric donors by judicial channel and living-related donors. Later, with the gradual standardization of renal transplantation work, laws and regulations on organ transplantation have been improved. The use of condemned prisoner donors by judicial channels has been completely prohibited since January 2015, and the DCD donor has become the only source of cadaveric donor [6]. This has led to a massive shortage of kidneys. Due to the sharp rise in the number of patients awaiting renal transplantation, the scheme of expanded criteria donor (ECD) is one of the solutions to the severe shortage of kidneys, lower donor quality, and significant difference in the quality of the DCD donor and living-related donor [7]. Two studies have confirmed the relationship between DCD renal transplantation and postoperative diarrhea [8, 9]. They suggested that there was a correlation between DCD renal transplantation recipients and diarrhea complication, and analyzed the possible risk factors. Relevant data from 158 patients who underwent allogeneic renal transplantation from 2015 to 2018 were collected in a comparative study on DCD and living-related renal transplantation. The statistical analysis suggested that there were more complications in DCD renal transplantation than in living-related donor renal transplantation [6].
In contrast, Ma et al. [10] analyzed the characteristics of Clostridium difficile in patients who underwent DCD renal transplantation, and found that the time of intestinal infection occurring in DCD renal transplantation recipients was irregular and was unrelated to the time of oral tacrolimus and the trough concentration of tacrolimus. Therefore, we included two types of donors in this study as the risk factors that cause diarrhea after renal transplantation. We found that one independent risk factor for diarrhea after renal transplantation was the type of donor in which DCD conformed to the original hypothesis. However, in terms of DCD renal transplantation recipients, our center chose ATG or basiliximab
Induction scheme
Immunity induction treatment before renal transplantation is an important method to prevent renal transplantation rejection. On the relationship between the immunity induction scheme and diarrhea, a study showed that ATG and monoclonal antibody OKT3 treatments were associated with diarrhea in nearly a third of patients, with diarrhea lasting for 3–4 days and going away automatically [11]. One possible mechanism by which these antibodies cause diarrhea is that the tumor necrosis factor (TNF) is released by activating T cells. Then, the TNF interferes with the absorption of the sodium ion and destroys the intestinal mucosal barrier [12]. Studies have suggested that T cell-mediated acute diarrhea occurs after the injection of CD3 + specific antibody, for which a possible mechanism is the increased intestinal permeability. In this disease model, the injection of anti-CD3 + monoclonal antibody leads to systemic cytokine release and acute TNF-dependent diarrhea [13]. Thus, there is a significant correlation between diarrhea and monoclonal antibody and polyclonal antibody. In this paper, the three immunity induction schemes applied before renal transplantation included basiliximab alone, ATG alone, and basiliximab
MPA
The combination of CNI and MPA is the standard immunosuppressive therapy after renal transplantation. For a long time, the view that enteric-coated mycophenolate sodium (EC-MPS) and mycophenolate mofetil (MMF) cause diarrhea after renal transplantation [14]. It was reported that the frequency of diarrhea in patients who took 3 g MMF daily for three years after transplantation was up to 38.4% [15, 16]. A meta-analysis showed that the relative risk of diarrhea from MMF was 1.57 [17]. The study by Ortega et al. [18] indicated that the incidence of diarrhea from EC-MPS may be lower compared to renal transplantation recipients who used MMF. The pathological mechanism of diarrhea from MMF remains unclear. One possible mechanism is that gastrointestinal epithelial cells grow and proliferate, relying in part on the de novo synthesis pathway of purine synthesis, and thus are efficiently inhibited by MPA and lead to diarrhea [19]. Whether the immunosuppressor combination scheme that converts MMF to EC-MPS reduces the diarrhea symptom remains controversial. One study showed that for renal transplantation recipients who developed poor gastrointestinal symptoms due to MMF, conversion of MMF to EC-MPS increased the maximum tolerance for MPA and reduced gastrointestinal complications, thereby improving patients’ gastrointestinal tolerance [9]. In the face of MPA-related diarrhea, it has been reported that most transplantation centers convert MPA to azathioprine, mizoribine, and sirolimus. This method is safe in the short term [20]. However, some studies have confirmed that azathioprine reduces the long-term survival rate of grafts [21]. The long-term survival rate of the transplanted kidney after conversion of MPA to mizoribine or sirolimus remains unclear. Yet, the American Registry of Kidney Transplant Science suggests that MPA reduces the relative risk of graft loss by 27% (
DGF
Faced with the high proportion of DCD renal transplantation currently in society, many transplantation centers choose ECD donors who are older or have cardiovascular and cerebrovascular disease complications, so as to not waste scarce kidney resources [28]. Then, the DGF is inevitable after renal transplantation and occurs in the majority. Akinlolu et al. [29] found that DGF is one of the critical risk factors for the increased incidence of AR, and DGF after renal transplantation significantly reduces the quality of life of renal transplantation recipients. Studies have reported that the incidence of DGF is as high as 40% in current renal transplantation recipients [30]. In the analysis of risk factors for diarrhea after renal transplantation, DGF is an indispensable factor. The results of this study suggest a statistical differences in the occurrence of DGF after renal transplantation between the diarrhea and non-diarrhea groups. The relevant mechanism of DGF, as an independent risk factor for diarrhea after renal transplantation, is that the transplanted kidney’s functional recovery is poor, and some drugs metabolized by the kidney accumulate in the human body for a long time, increasing the risk of diarrhea to a greater extent. This is consistent with the analysis of risk factors for renal transplantation perioperative diarrhea conducted by Ma et al. [31], however, the specific mechanism of DGF involvement in diarrhea after renal transplantation still needs to be explored.
In addition, it should be noted that immunosuppressive therapy before and after renal transplantation is one of the critical links to preventing rejection reactions. Then, the decline of immune function after renal transplantation undoubtedly leads to infection, while infection is the most common cause of death after renal transplantation [32]. Therefore, most transplantation centers provide antibiotic treatment to prevent infection in the renal transplantation perioperative period. The antibiotic treatment essentially leads to an imbalance of intestinal flora, thereby leading to diarrhea. Thus, different infection prevention schemes are the risk factors for diarrhea after transplantation. Ma et al. [33] showed that the use of different antibiotics in the renal transplantation perioperative period had statistically significant differences between the diarrhea and non-diarrhea groups. In this study, infection prevention schemes were not included in the analysis because our center adopted a unified antibiotic infection prevention scheme.
Predictive factors
The ROC curve was drawn for the above four predictive factors and the combination of predictive factors, and the AUCs were calculated. According to the medical statistical analysis, the ROC curve results were interpreted as follows: AUC
Conclusion
In conclusion, based on the above four predictive factors, we suggest the adoption of immunosuppressors with small gastrointestinal reactions for DCD renal transplantation recipients or patients with postoperative DGF while avoiding drugs excreted by the kidney. For patients with risk factors for diarrhea after renal transplantation, it is necessary to choose the immunity induction scheme more carefully, strengthen the monitoring, promptly adjust the immunosuppressor when diarrhea occurs, and initiate prevention schemes early, such as adjusting the intestinal flora and protecting the gastrointestinal mucosa, to reduce the incidence and poor prognosis of diarrhea after renal transplantation.
Funding
No external funding was received to conduct this study.
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of the Second People’s Hospital of Shanxi Province (No. 202301).
Informed consent
Written informed consent was obtained from the participants or legal guardians for participating in this study.
Availability of data and materials
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Footnotes
Acknowledgments
We are particularly grateful to everyone who helped us with our article.
Conflict of interest
The authors declare that they have no competing interests.