
Abstract
BACKGROUND:
To improve gait disability in patients with chronic stroke, ankle muscle strengthening and calf muscle stretching exercises are required. However, currently available ankle training equipment limit ankle exercises based on the position. Recently developed ankle training equipment enables spring resistance-based plantar press exercises to be performed in the standing position with weight support.
OBJECTIVE:
To conduct a usability test of the ankle training equipment in the standing position by stroke patients with hemiplegic gait and verify its effects on ankle movements.
METHODS:
The ankle training equipment was applied to five patients with chronic stroke and hemiplegic gait. In the standing position, the patients performed forefoot and rearfoot press exercises in the affected side with a day’s interval at 20 repetitions maximum (RM). During the exercises, surface electromyography (sEMG) was used to measure the maximum voluntary isometric contraction (%MVIC) of the leg muscles. The System Usability Scale (SUS) was used to assess the ankle training equipment. Wilcoxon signed-rank test was used to evaluate the differences in muscle activity between the two exercises.
RESULTS:
Forefoot and rearfoot press exercises increased the %MVIC in the biceps femoris. Additionally, the tibialis anterior and medial gastrocnemius activity was significantly different between the two exercises. The SUS was 78.75% (SD 12.7).
CONCLUSION:
The usability test of the passive-control foot press trainer (PFPT) that with improvements in the structure and functions for convenience, it could be commercialized. PFPT could be an alternative to the ankle rehabilitation robot that necessitates a sitting position.
Introduction
Stroke is a common cerebrovascular disease characterized by chronic neurological deficits arising due to brain tissue destruction [1]. It is the third most frequent cause of death in countries belonging to the Organization for Economic Cooperation and Development and commonly leads to various disabilities [2]. Stroke limits all physical activities, including movements of the upper and lower limbs, posing a challenge to performing activities of daily living and consequently reducing the quality of life [2]. With the advancements in healthcare technology, the survival of patients with stroke is steadily increasing. Currently, Furthermore, due to the declining incidence of stroke, there is a concurrent reduction in the post-stroke survival period [3].
For the rehabilitation of stroke patients, interventions traditionally administered by physical therapists and occupational therapists are now being executed through the utilization of machines or robotic systems. However, while these systems are making strides in assisting with walking and upper limb movements, they are not yet capable of replicating the full spectrum of therapeutic interventions provided by human therapists, motivating active research efforts in this domain [4].
Post-stroke disability affects a wide spectrum of functions from muscle tension to balance, weight shift and support, and motor control abilities according to the area of brain damage. Based on the cause, post-stroke disability can include defects in the perception, muscle strength and tension, sensation, and motor control. Patients with ankle disability, such as foot drop due to reduced muscle strength on the paretic side, presents with a partial or complete loss of motor function, making it difficult to maintain independent ankle range of motion (ROM). The reduced ankle ROM causes muscular atrophy and contraction-induced ankle stiffness, which is the main cause of gait disability [5]. In foot drop, the impulse is reduced in the stance phase and forefoot clearance is reduced in the swing phase, causing dragging of the foot and toes. Foot drop is seen in several brain and spine diseases, including stroke, polio, Charcot-Marie-Tooth disease, multiple sclerosis, and cerebral palsy [3, 5, 6, 7, 8].
The level of recovery of gait is a key predictor of post-stroke disability and a top-priority in post-stroke rehabilitation [6, 9]. The Robot-based Ankle Foot Orthosis and Functional Electrical Stimulation (FES) enhance the gait in patients with post-stroke hemiplegia, by effectively improving the gait cycle, gait speed, and muscle strength. A combination of FES and the newly developed muscle synergy-based stimulation algorithm contribute to normalizing gait and effectively improving it in patients with chronic deficits [10].
The conventional rehabilitation training for the recovery of lower limb motor function in patients with post-stroke hemiplegia includes a high-intensity exercise program. The exercise program consists of stepwise contractions and passive, assistive, active or active resistance exercises. As the frequency and duration of these exercises directly affect the level of recovery, the training program should be repeatedly offered; however, this is physically demanding for therapists [11, 12, 13, 14]. To address this issue, various training equipment and robots have been developed and applied.
For the recovery of lower limb motor function, eccentric strengthening exercises are superior to concentric exercises; eccentric exercises stimulate collagen synthesis in the muscle and tendon and promote muscle cell growth and generation. Thus, the Eccentron (BTE Technologies Inc., Hanover, MD, USA) was developed to allow eccentric lower limb exercises in a seated position. However, it cannot be applied to certain regions due to the limitation of the stepper-type multi-joint exercise methods [15]. Conventional ankle rehabilitation relies on the experience of physical therapists and induces physical burnout in those who are required to hold the patient’s ankle toward contraction during ankle movements. To overcome these issues, platform-based ankle rehabilitation equipment and robots have been developed, focusing on ankle dorsiflexion strengthening in a seated position in lieu of therapists. However, ankle training in a seated position eliminates the effect of gravity, and the protocol does not incorporate tailored trainings [16, 17, 18]. As an alternative to the conventional high-cost ankle rehabilitation robots (Stewart’s platform or powered exoskeleton), the Motorized Ankle Stretcher (MAS) was developed to increase the ankle dorsiflexion and adaptability through active and gradual stretching of the lower calf muscles in the standing position. However, the MAS was limited in allowing active muscle strengthening [19]. A 360∘ anterior pedaling exercise while standing leads to high ankle torque and gastrocnemius activity as the pedal on the paretic side approaches 180∘, which is the farthest point with increased exposure to gravity. However, performing this exercise in a seated position with little exposure to gravity leads to higher gastrocnemius activity as the pedal approaches the closest point [20].
Based on the training equipment developed and evaluated in previous studies, we developed a passive-control foot press trainer (PFPT) as an ankle training. Forefoot and rearfoot press exercises can be performed using the PFPT and a spring resistance-based pedal in the standing position with exposure to gravity. Improving lower limb motor function is the key to the recovery of motor function. The novel equipment allows for repeated trainings of gait simulation in the standing position. We aimed to assess the usability of the PFPT ankle training equipment in patients with post-stroke hemiplegic gait in combination with spring resistance-based plantar press exercises in the standing position.
Methods
Device development
The PFPT ankle-training equipment is a device that allows the user to perform forefoot and rearfoot press exercises while controlling the contraction intensity. The device comprises a plate on which the user can perform the exercises. There are handles on either side of the plate for the user to maintain stable postures during exercise. The center of the plate has a spring that can be replaced with a spring of a different elasticity level to control the resistance and contraction intensity during plantar press exercises. The pedal-based forefoot and rearfoot press exercises depict anterior and posterior rotations in the ankle joint, respectively. The novel equipment was developed to allow forefoot and rearfoot press exercises with motions simulating gait patterns.
Participants
In a study conducted by Virzi [21], it was determined that the optimal number of subjects for usability evaluation is between 5 and 8 people, as up to 90% of usability-related issues can be identified within this range. Therefore, the study utilized a sample size of 5 participants for analysis, in accordance with this finding. Five community-dwelling patients with post-stroke hemiplegia participated in the study. The inclusion criteria were as follows: 1) hemiplegia caused by a cerebrovascular event, cerebral hemorrhage, or infarction; 2) stroke
This study complied with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of the National Rehabilitation Center Rehabilitation Hospital (No. NRC-2022-07-055; date 8 November 2022). Informed consent was obtained from each participant for voluntary participation in the study. The participants’ baseline general characteristics, including age, affected side, height, weight, body mass index (BMI) and FAC are summarized in Table 1.
General characteristics of participants (
5)
General characteristics of participants (
SD: Standard deviation.
First, this study was structured as a single-group, cross-sectional investigation with a singular measurement, and it did not incorporate any randomization procedures. Second, sEMG was used to measure the maximum voluntary isometric contraction (MVIC) of the target lower limb muscle on the paretic side. Subsequently, each participant performed the forefoot and rearfoot press exercises using the PFPT ankle training equipment at 20 repetition maximum (RM) in set time intervals, with a metronome set to 60 bpm to maintain identical exercise speed. During the exercises, the activity levels of the tibialis anterior, medial and lateral gastrocnemius heads, rectus femoris, and biceps femoris were measured using the five channels of the sEMG. The %MVIC values were compared. At the end of the test, the System Usability Scale (SUS) was applied to the participants to evaluate the usability of the PFPT.
Measurements
First, the manual muscle test (MMT) was performed and the passive ROM (dorsi- and plantar-flexion) of the affected ankle was measured. The MMT comprises six grades from 0 to 5: 0 (Zero), indicates no palpable or visible muscle contraction; 1 (Trace), indicates palpable muscle contraction without motion; 2 (Poor), indicates motion upon reduced or eliminated gravity; 3 (Fair), indicates motion against gravity; 4 (Good), indicates complete motion against moderate resistance and gravity; and 5 (Normal), indicates complete motion against maximum resistance and gravity. The passive ankle ROM was measured using a goniometer; triplicate measurements were obtained and the mean was used in the analysis.
The muscle activity levels of the tibialis anterior, medial and lateral gastrocnemius heads, rectus femoris, and biceps femoris were measured during the forefoot and rearfoot press exercises using a wireless sEMG device (Delsys Trigno Wireless EMG Surface Electrodes; Delsys Incorporated, Boston, MA, USA). To ensure accurate measurements, the electrodes were attached to the target muscles on both lower limbs, parallel to the direction of the muscle fibers. To minimize resistance, the skin of the target sites and electrodes were wiped with alcohol prior to attachment. The electrode attachment sites were determined via palpitation according to the SENIAM guidelines (www.seniam.org). EMG signals were detected at each channel in the five muscles. The sampling rate of the EMG signal was set at 1,259 Hz. The amplified waveforms were filtered through 20–45 Hz band pass filters. The signals collected during muscle contraction were processed by Root Mean Square (RMS). For use as the normalization criteria, the %MVIC was derived from the MVIC measured after resampling at 1,000 Hz. The MVIC was measured before the exercise, just as in a previous study. The participants were instructed to perform ankle and knee joint flexion and extension in the standing and seated positions. The ankle ROM was recorded three times, with each motion held at the maximum force for 5 s. There was a 30 s period of rest between each measurement. The 3-s mean muscle activity, by excluding the first and last s, were recorded as the result.
System Usability Scale questionnaire
System Usability Scale questionnaire
System Usability Scale score classification
The SUS is a simple, practical, and reliable questionnaire, consisting of 10 questions, that were used to evaluate the usability of various products and services. The tool can detect a problem associated with usability in various digital products and services. Each of the 10 items are rated on a 5-point Likert scale (1
The participants’ general and functional characteristics were expressed as mean
Functional characteristics
Functional characteristics
ROM: Range of motion, MMT: Manual Muscle Testing, SD: Standard deviation.
System Usability Scale evaluation results (
M: Mean, SD: Standard deviation.
The developed passive-control foot press trainer.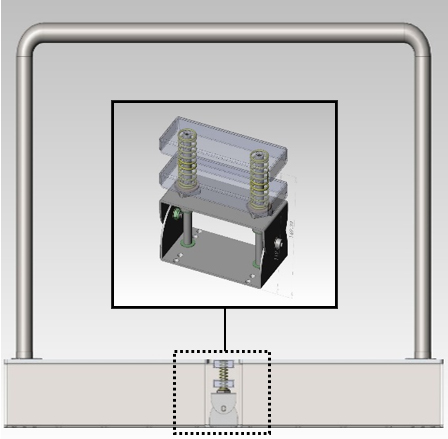
Measuring muscle activity of tibialis anterior, medial and lateral gastrocnemius, rectus femoris, biceps femoris. (a) Forefoot press exercise, (b) Rearfoot press exercise.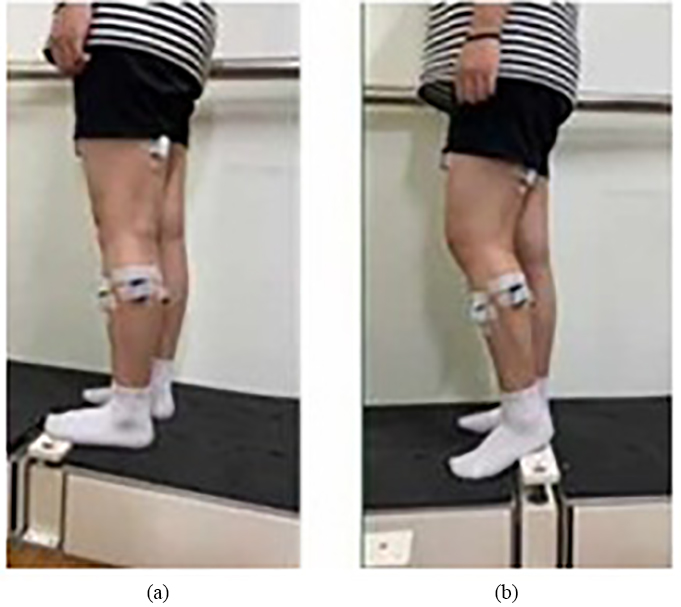
Comparison of EMG activity between forefoot and rearfoot exercises. %MVIC: Maximum Voluntary Isometric Contraction.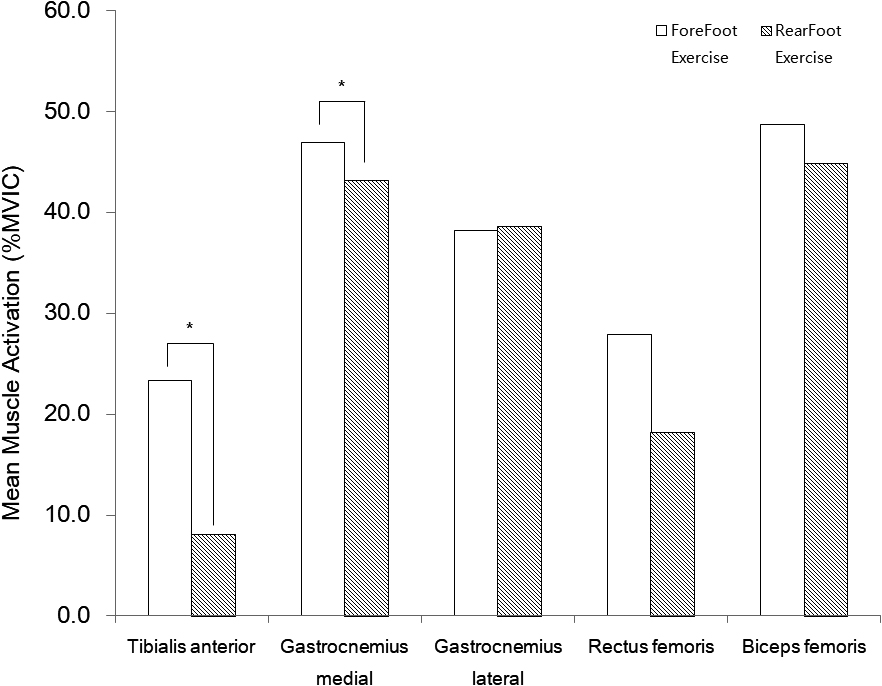
The mean MMT and passive ROM values of the paretic ankle are presented in Table 4.
The biceps femoris muscle showed the highest activity during the forefoot and rearfoot press exercises, followed by the medial gastrocnemius, lateral gastrocnemius, rectus femoris and tibialis anterior muscles. The %MVIC of the tibialis anterior and medial gastrocnemius were significantly different between the two exercises (
The mean SUS score was 78.75, indicating a B
Discussion
The PFPT, an ankle training equipment, was developed in this study to strengthen the foot and ankle muscles for the recovery of lower limb motor function and gait. The novel equipment allowed forefoot and rearfoot press exercises to be performed in the standing position with exposure to gravity and use of a spring resistance-based pedal. An advantage of this system is the possibility of repeated gait training simulations in the standing position. We conducted a usability test on the PFPT training equipment in patients with post-stroke hemiplegic gait for spring resistance-based plantar-press exercises in a standing position.
The mean SUS score in our study was 78.75; Excellent for adjective ratings, acceptable for acceptance level, and neutral for recommendations, implied an overall high level of satisfaction with the PFPT ankle training equipment developed in this study. Based on previous studies [22, 23], the structure and function of the equipment was improved for convenience, with a focus on the items showing scores lower than the mean (simplicity, integration, learnability and convenience). Improvement of these parameters could allow PFPT to become commercialized and satisfy consumer demands. However, formative and summative usability tests should continue to be performed to determine improvement, which is critical in developing effective equipment [24]. Further studies that repeatedly conduct usability tests for PFPT are required to ensure systematic improvements.
The differences in muscle activity levels were comparatively analyzed based on the %MVIC; the biceps femoris muscle had the highest muscle activity level during the foot press exercises, followed by the medial gastrocnemius, lateral gastrocnemius, rectus femoris and tibialis anterior. The high biceps femoris activity may be attributed to the high use of biceps femoris to efficiently create exercise motions against gravity in the standing position, to compensate for the inadequate passive ROM and MMT. The passive ROM was 8∘ (Dorsiflexion normal range: 20∘) and 27∘ (Plantarflexion normal range: 50∘) for dorsiflexion and plantarflexion, respectively. The MMT was 2.3 and 2.7 for dorsiflexion and plantarflexion, respectively [25]. reported an increase in the biceps femoris activity in response to an increase in the weight load. In our study, the medial and lateral heads of the gastrocnemius muscle showed high activity during the forefoot and rearfoot press exercises, which concur with the results of a previous study [20, 26]. Brown et al. stated that the ankle torque and gastrocnemius activity was highest as the pedal on the paretic side approached the farthest point, with increased exposure to gravity during exercises in the standing position.
The forefoot press exercise led to significantly higher activity levels in the tibialis anterior and medial gastrocnemius muscle than the rearfoot press exercises did. As patients with stroke pedaled, the tibialis anterior activity significantly varied [27]. Likewise, the tibialis anterior activity was higher in the forefoot press exercise than in the rearfoot press exercise in our study. Our findings indicate that the forefoot press exercise in the standing position could be used as an alternative to the conventional dorsiflexion exercise using an ankle rehabilitation robot for strengthening the tibialis anterior and medial gastrocnemius muscles [16, 17, 18].
In this study, we conducted an evaluation focusing on exercise movements involving the pressing of the forefoot and hindfoot in a standing position. However, as part of our ongoing research, we intend to develop an expanded range of applications beyond these two simple movements. Our specific goal is to conduct a comprehensive usability assessment that considers the distinct traits of patients with central nervous system diseases. We will primarily focus on aligning the device’s functions with therapeutic standards and differentiating it from existing commercial lower extremity exercise devices [28]. Through these efforts, we anticipate potential enhancements to the device’s functionalities based on the insights gained from our research. If such improvements are realized, they could lead to advancements in existing device design. It’s worth noting that while this study employed EMG measurements using a similar design, future investigations will require additional considerations. Both needle electromyography (EMG) and surface electromyography (sEMG) quantify motor unit activation through muscle electrical signals. Consequently, Manual Muscle Testing (MMT) yields numeric strength measurements that exhibit a correlation with EMG [29] but are limited to the ordinal grading scale. This limitation arises from the inherent constraints of an evaluation method reliant on maximal muscle strength as the benchmark, in line with Maximum Voluntary Contraction (MVC) and Reference Voluntary Contraction (RVC), which serve as the primary means for interpreting EMG signals. Therefore, while our device is designed for use by a broad spectrum of individuals, from the general public to patients with central nervous system diseases, follow-up research is imperative to separately assess usability and design refinements, while validating the device’s appropriate utilization.
Conclusions
With improvements on the structure and functions for convenience of use, the PFPT ankle training equipment developed in this study could be commercialized to satisfy the consumer demand, as suggested by the results of the usability test in our study. Furthermore, the forefoot press exercise in the standing position using the PFPT could be an alternative to the conventional dorsiflexion exercise in the seated position using an ankle rehabilitation robot, as confirmed by our comparative analysis of the muscle activity.
Nevertheless, there was a limitation in analyzing the characteristics of the forefoot and rearfoot press exercises and defining the method of use; it is difficult to apply the PFPT in a standing position in participants with abnormal ROMs and low muscle strengths. Further studies are required to verify the effects of the equipment by conducting usability tests in a wider population with varying levels of physical function. This will aid in applying PFPT in exercises tailored to each patient’s characteristics, improving the electric motor control-based PFPT, and establishing guidelines for its use for suitable exercise intensity application.
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This study was supported by the Translational Research Project for Rehabilitation Robots, National Rehabilitation Center, Ministry of Health and Welfare, South Korea (#NRCTR-IN23006).