
Abstract
BACKGROUND:
Ectopic pregnancy is a major contributor to maternal morbidity and mortality across the globe.
OBJECTIVE:
This study aims to investigate the clinical benefits of laparoscopic surgery in treating ectopic pregnancy, and its impact on tubal patency and reproductive outcomes.
METHODS:
A clinical study was conducted to compare laparoscopic and medical conservative treatment for ectopic pregnancy. A total of 206 patients were treated for ectopic pregnancy at our hospital from January 2018 to June 2020. Among them, 46 underwent laparoscopic ipsilateral salpingectomy, 54 underwent laparoscopic ipsilateral salpingostomy with lesion removal, and 106 were treated conservatively with medication.
RESULTS:
The age range and average age of each group are provided, with no significant differences in these general demographic characteristics (
CONCLUSION:
Laparoscopic surgery for ectopic pregnancy offers significant clinical benefits over conservative medical treatment, including higher rates of tubal patency and improved reproductive outcomes. These findings support laparoscopic surgery as an effective approach for the management of ectopic pregnancy.
Keywords
Introduction
Ectopic pregnancy, characterized by the implantation of a fertilized ovum outside of the uterine cavity, is a major contributor to maternal morbidity and mortality across the globe [1]. Tubal pregnancy, the most prevalent type, constitutes over 90% of all ectopic pregnancies. In recent years, the incidence of ectopic pregnancy has been on the rise, particularly amongst nulliparous women [2]. Traditionally, ectopic pregnancies have been managed by medical conservative treatment, primarily through laparotomy and salpingectomy to remove the implanted embryo [3]. However, the nature of medical conservative treatment can introduce substantial risks to the patient, encompassing a prolonged recovery period, elevated risk of postoperative complications, and potential detrimental effects on future fertility [4].
In the past years, laparoscopic surgery, a minimally invasive approach, has emerged as the increasingly preferred option for treating ectopic pregnancies [5]. Several benefits of this technique have been recognized, including reduced hospital stays, faster recovery periods, less pain, and lesser intraoperative blood loss compared to open surgery [6]. Additionally, laparoscopy is linked with better conservation of the fallopian tubes, which may potentially enhance future fertility outcomes [7].
At present, when choosing a treatment plan, clinical focus is not only given to its effectiveness but also to the impact of the treatment on future pregnancy outcomes. The clinical treatment options available include expectant management, medical conservative treatment, surgical treatment, and interventional treatment. This article offers a comparative analysis of two laparoscopic surgical techniques, specifically salpingectomy and salpingostomy, as well as the pregnancy outcomes and tubal patency following medical conservative treatment, with the aim of providing a foundation for selecting treatment options in clinical practice.
Materials and methods
This study was formulated as a retrospective cohort analysis aimed at comparing the outcomes of laparoscopic surgery versus medical conservative treatment in the management of ectopic pregnancy.
Patient selection
We collected clinical data from 206 patients diagnosed with tubal ectopic pregnancy who were admitted to our hospital from January 2018 to June 2020. Among them, 46 underwent laparoscopic salpingectomy on the affected side, 54 underwent laparoscopic salpingostomy to remove the pregnancy tissue while preserving the affected fallopian tube, and 106 received medical conservative treatment. The salpingectomy group had an age range of 21 to 42 years, with an average age of (33.5
Inclusion criteria for medical conservative treatment
Methotrexate (MTX) is widely used for the treatment of tubal pregnancy [8]. The criteria include: (1) Pre-treatment evaluations suggest an unruptured ectopic pregnancy, and the patient wishes to retain fertility. (2) The patient’s vital signs are relatively stable, with no severe abdominal pain or significant intra-abdominal bleeding. (3) The tubal pregnancy mass measures less than 35–40 mm, with no cardiac activity observed. (4) Serum beta-human chorionic gonadotropin (
Inclusion criteria for laparoscopic surgery
(1) Unstable vital signs and symptoms of ruptured tubal pregnancy (pelvic pain, intra-abdominal bleeding). (2) Absolute contraindications to medical treatment or treatment failure requiring surgical intervention. Surgical treatment may be considered for patients with relative contraindications. The laparoscopic procedures include salpingostomy (removal of the ectopic pregnancy while preserving the fallopian tube) and salpingectomy on the affected side.
Salpingectomy is indicated for the following:
Patients who require removal of the affected fallopian tube. Emergency cases with significant intra-abdominal bleeding and shock. Patients with severe tubal adhesions or large lesions that compromise the mesosalpinx or blood vessels. Patients with a history of disease or surgery on the affected side, such as previous tubal pregnancy or tubal anastomosis for infertility.
Specific methods for conservative treatment
Calculate the patient’s body surface area based on their height and fasting body weight, and administer methotrexate (MTX) by intramuscular injection at a dose of 50 mg/m2. After 7 days of treatment, evaluate the patient’s liver and kidney function, as well as blood
Laparoscopic salpingectomy on the affected side
After the patient achieves effective general anesthesia, the patient is positioned with the head lowered and the buttocks elevated. A vertical incision of approximately 1.0 cm is made at the upper edge of the umbilical ring, and a 1.0 cm trocar is inserted for puncture. Under laparoscopic guidance, the second puncture hole was made at the medial aspect of the anterior superior iliac spine on left sides, and the third puncture hole was made 20–30 cm lateral to the midline and 20 cm above the pubic symphysis. A fourth puncture hole was added at the McBurney’s point if necessary for the surgical procedure, and a 0.5 cm cannula was inserted for puncture. Surgical instruments are inserted. The pelvic and abdominal cavities are explored, and the surgical field is adequately exposed. The uterus and bilateral adnexa are examined to restore normal anatomical structures and expose the site of pregnancy. Starting from the fimbrial end of the affected side fallopian tube, the fallopian tube is coagulated and cut using bipolar electrocoagulation along the mesosalpinx to the proximal cornual area of the uterus. The fallopian tube is removed, and after confirming the absence of residual lesions, the pelvic cavity is irrigated with sterile water for injection. If there is bleeding at the incision site, bipolar electrocoagulation is used for hemostasis, and a drainage tube may be placed if necessary. Weekly follow-up of blood
Laparoscopic salpingostomy for the removal of ectopic pregnancy
The exploration steps are the same as those for laparoscopic salpingectomy. The site of pregnancy is exposed, and a unipolar needle-shaped electrode is used to make a longitudinal incision on the serosal side of the fallopian tube at the weakest point of the ectopic pregnancy. The length of the incision is approximately equal to the size of the pregnancy lesion. The pregnancy sac is exposed, and a flushing tube is gently inserted into the fallopian tube for hydrodissection. An aspirator is used to remove the trophoblastic tissue at that location, which can usually be completely aspirated. If the trophoblastic tissue is densely adhered to the tube wall, gentle grasping forceps can be used for extraction. After removing all visible lesions, the fallopian tube lumen and pelvic cavity are irrigated with sterile water for injection to ensure no residual trophoblastic tissue. Bipolar electrocoagulation is used to stop bleeding at the incision site. A drainage tube may be placed if necessary. Weekly follow-up of blood
Outcomes measures
The primary outcomes were the comparison of observation indicators in 3 groups of patients after 3 years of treatment for normal intrauterine pregnancy and ectopic pregnancy, and comparison of tubal patency and ectopic pregnancy sites between the group undergoing laparoscopic salpingostomy for the removal of ectopic pregnancy and the group receiving medical conservative treatment. Tubal patency refers to the unobstructed or un-narrowed condition of the fallopian tubes, allowing sperm and egg to meet without difficulty. To evaluate this, we used hysterosalpingography (HSG) or laparoscopy, which are standard methods in clinical practice.
Statistical analysis
Statistical analysis was performed using SPSS 19.0 software. Count data were presented as number of cases (%) and compared using the chi-square test. A
Ethics approval
The study was approved by the Institutional Review Board of our hospital, and all methods were carried out following the relevant guidelines and regulations. As this was a retrospective study using de-identified data, the requirement for informed consent was waived.
Results
Patient demographics
This study incorporated clinical data from 206 patients who were treated for ectopic pregnancy at our hospital from January 2018 to June 2020. Among these patients, 46 underwent laparoscopic ipsilateral salpingectomy, 54 underwent laparoscopic ipsilateral salpingostomy with lesion removal, and 106 were treated conservatively with medication. The age range for the salpingectomy group was between 21 and 42 years, with an average age of 33.5
The demographic and characteristics of three study groups
The demographic and characteristics of three study groups
Both the group that underwent laparoscopic unilateral salpingostomy for ectopic pregnancy removal and the group receiving conservative medical treatment exhibited higher rates of ectopic pregnancy compared to the group that underwent laparoscopic unilateral salpingectomy. These differences were statistically significant (
Long-term reproductive outcomes in three groups
Long-term reproductive outcomes in three groups
When comparing tubal patency between the group that underwent unilateral salpingostomy for ectopic pregnancy and the group that received conservative medical treatment, the results were as follows: Three months post-normalization of blood
Tubal patency in the group of conservative surgery and the group of medical conservative treatment
Tubal patency in the group of conservative surgery and the group of medical conservative treatment
Image data during laparoscopic surgery. Laparoscopic View During Ectopic Pregnancy Surgery. This figure represents intraoperative image data captured during laparoscopic procedures performed on patients with ectopic pregnancies. The image highlights the surgical field, demonstrating the real-time visibility afforded to surgeons during laparoscopic intervention, enabling precise surgical intervention while minimizing collateral tissue damage.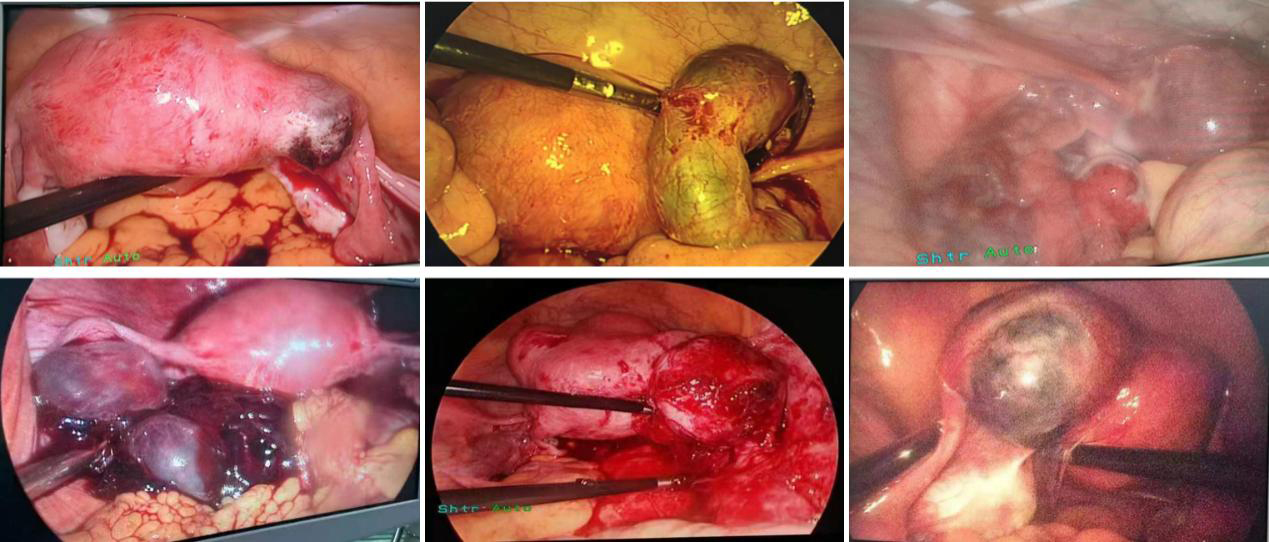
The fundamental aim of this study was to delve into the clinical benefits of laparoscopic surgery for ectopic pregnancy treatment, and to comprehend its implications on tubal patency and reproductive results. Ectopic pregnancy remains a significant health issue that contributes to global maternal morbidity and mortality, especially in areas with limited access to advanced healthcare infrastructures [10]. This study encompassed a total of 206 patients who received ectopic pregnancy treatment at our hospital between January 2018 and June 2020. It was discovered that the laparoscopic ipsilateral salpingectomy and salpingostomy groups exhibited different outcomes compared to the conservative medication treatment group. There were no statistically significant variations in the demographic attributes among the groups, implying that factors such as age did not considerably affect the treatment outcomes. Notably, we found that the ectopic pregnancy rates were elevated in the salpingostomy and medication groups in comparison to the salpingectomy group. Furthermore, within a span of three years, we noticed a recurrence of ectopic pregnancies, with the salpingostomy and medication groups demonstrating higher recurrence rates. Interestingly, the salpingostomy group showed a higher rate of tubal patency three months post blood
Comparison with previous studies
Our findings are consistent with existing literature, which indicates that laparoscopic surgery, whether salpingectomy or salpingostomy, provides better outcomes compared to the medical management of ectopic pregnancy [11]. Moreover, the higher rates of recurrent ectopic pregnancy observed in our salpingostomy and medication groups are in line with previous studies that suggest an increased recurrence risk following conservative treatments [12]. However, the higher tubal patency rate observed in our salpingostomy group three months post-treatment represents a significant finding that contradicts some prior studies, which have reported similar patency rates between surgical and medical management groups [13]. This finding implies a potential advantage of laparoscopic salpingostomy in preserving tubal patency, which merits further investigation.
Explanation of findings
The reduced recurrence rate of ectopic pregnancy in the salpingectomy group is likely attributable to the complete removal of the affected fallopian tube. By eradicating the site of the ectopic pregnancy, the risk of reimplantation in the same location is theoretically eliminated [14]. However, it is important to mention that this doesn’t entirely rule out the possibility of an ectopic pregnancy in the opposite tube.
The superior tubal patency observed in the salpingostomy group can be credited to the conservative nature of the procedure. Salpingostomy involves the extraction of the ectopic pregnancy while preserving the fallopian tube, thereby retaining its potential functionality and contributing to improved rates of subsequent intrauterine pregnancy [15]. It should be considered, however, that while tubal patency is enhanced, the risk of recurrent ectopic pregnancy persists.
Clinical implications
The study’s findings could influence the management of ectopic pregnancy. It presents a clear rationale for considering the preservation of the fallopian tube in patients who desire future fertility. However, it is important to balance this desire against the risk of recurrent ectopic pregnancy. These factors should be discussed with patients when making a decision about the best treatment approach.
The standard medical suggestions for future fertility for patients who have had previous ectopic pregnancies are individualized based on the patient’s specific conditions, such as their age, overall health status, and the details of their previous ectopic pregnancy. Generally, we emphasize close monitoring in subsequent pregnancies, as the risk for another ectopic pregnancy increases after one has occurred. We also recommend waiting for at least three months after treatment for an ectopic pregnancy before trying to conceive again, to allow for physical recovery and emotional readiness. We understand the importance of explicitly stating these suggestions in our manuscript.
Strengths and limitations
The strengths of this study involve a sizable sample and the comparison of three distinct treatment methods, which bolsters the validity of our findings. In addition, our study was executed at a single center, thereby minimizing variability due to differing institutional practices or patient demographics [16].
Nonetheless, it is imperative to acknowledge some limitations. Firstly, the absence of long-term follow-up may have influenced our comprehension of fertility outcomes post-ectopic pregnancy treatment, especially considering that fertility impacts might not be evident until years later. Secondly, the study’s retrospective design is prone to potential biases, including selection bias and information bias. Although the manuscript has a retrospective design, it is still necessary to point out the risk of elevated type I errors. Lastly, although we accounted for known confounding variables, the potential for residual confounding from unmeasured variables persists [17].
Future research directions
Our study underscores the importance of continuing research in this area. Future prospective studies with longer follow-up periods could provide valuable information about long-term fertility outcomes. Research could also be aimed at identifying patient-specific factors that could help predict which patients might benefit most from each treatment approach, allowing for more personalized care.
Artificial intelligence (AI) technologies, such as machine learning and deep learning, are rapidly evolving and are being integrated into various aspects of healthcare, including predicting outcomes, diagnosing conditions, and personalizing treatments [18]. In maternal-fetal medicine and obstetrics, AI can be beneficial in several ways. For instance, it can improve the accuracy of prenatal screening and diagnosis, optimize the management of high-risk pregnancies, and enhance fetal monitoring during labor. Previously, a study demonstrated the potential of a machine learning model in predicting preterm birth based on electronic health record data [19]. Another study investigated the reliability of using deep learning in quantifying the synchronization between the mother and fetus cardiac rhythms throughout gestation.
AI has been making significant strides in the realm of medical imaging, particularly in the diagnosis of infant neurological impairment disorders. Ultrasound remains a crucial tool in detecting such conditions. However, the interpretation of results often depends on the skill and experience of the sonographer, which can lead to inconsistencies. This is where AI can play a transformative role. AI-based ultrasound image classification systems leverage sophisticated algorithms to analyze the ultrasound images, identify patterns, and make predictions about potential neurological impairments. These systems can be trained on large datasets to increase their accuracy and efficiency. For example, a study by Xie et al. [20] utilized deep learning mode to classify pediatric brain ultrasound images and achieved promising results. Not only can AI help increase the accuracy and consistency of diagnoses, but it can also support radiologists by alleviating their workload and reducing the risk of human error.
AI continues to show substantial potential in the field of diagnostic medical imaging [21]. Recent advancements in machine learning and deep learning techniques have led to the development of models that can aid in image acquisition, interpretation, and diagnosis. A study comprehensively examined the use of AI in medical imaging [22]. They found that AI has been used across various imaging modalities, including MRI, CT, and Ultrasound, and for various diseases, such as cancer, cardiovascular diseases, and neurological disorders. AI-based models have demonstrated performance on par with or even exceeding that of human experts in some tasks, such as detecting certain types of cancer in imaging studies [23]. The application of AI in diagnostic medical imaging brings several benefits, such as improving diagnostic accuracy, enabling quantitative imaging, and potentially reducing the workload of radiologists. However, despite these promising results, the transition of AI into clinical practice presents challenges. These include the need for robust validation of AI models, regulatory concerns, issues related to data privacy and security, and the need for proper integration with existing healthcare IT systems. In conclusion, while the application of AI in diagnostic medical imaging presents considerable promise, careful consideration must be given to the aforementioned challenges to ensure its safe and effective use.
Conclusion
Our findings emphasize the clinical advantages of laparoscopic surgery for ectopic pregnancy, particularly with respect to tubal patency and possible reproductive outcomes. However, patient preference and unique clinical circumstances should always be taken into account when choosing the most suitable treatment modality for ectopic pregnancy.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the Aviation General Hospital of China. All subjects signed the informed consent form.
Data availability
All data in this study are true and reliable. The data that support the findings of this study are available from the corresponding author upon reasonable request. The remaining figure data are uploaded as supplementary materials.
Funding
None to report.
Author contributions
JY initiated the study. STS and YLQ coordinated the study. JY and PY contributed to the study design, literature search, figures, statistical analysis, data synthesis of outcomes and drafted and edited the final manuscript. All authors critically revised the manuscript and have read and agreed to the published version of the manuscript.
Footnotes
Acknowledgments
None to report.
Conflict of interest
The authors declare no competing interests.