
Abstract
BACKGROUND:
There is no specificity in the clinical presentation of hemophagocytic lymphohistiocytosis (HLH).
OBJECTIVE:
To study some clinical, etiological, and prognostic features of HLH to improve the clinical understanding of the disease.
METHODS:
Retrospective analysis of the clinical data of 125 patients with HLH admitted to our hospital from June 2015 to August 2021, including clinical characteristics, laboratory indicators, and survival period. Statistical analysis was performed from the overall group of study indicators, which included population, children, and adults.
RESULTS:
In the whole population, sex, age, blood myoglobin, and NK cell ratio of M-HLH and non-M-HLH patients (
CONCLUSION:
The survival rate of non-M-HLH was significantly better than that of M-HLH; the proportion of NK cells had predictive value for the diagnosis of M-HLH; in the general population, non-M-HLH was more likely to have abnormal liver function than M-HLH: lower platelet count and serum albumin level were associated with poor prognosis, and the lower the platelet count and serum albumin level, the worse the prognosis: in addition, adults with lower serum albumin levels are also associated with poor prognosis.
Introduction
Hemophagocytic lymphohistiocytosis (HLH), also called hemophagocytic syndrome (HPS), was first described by Farquhar et al. in 1952 [1]. There is no specificity in the clinical presentation of HLH. The main symptoms are persistent fever, hepatosplenomegaly, hepatocytopenia, liver dysfunction, coagulopathy, and phagocytosis of the bone marrow HLH is divided into primary and secondary phagocytic lymphohistiocytosis according to its cause. Primary hemophagocytic lymphohistiocytosis, also called familial hemophagocytic lymphohistiocytosis (FHL), is now a molecularly characterized autosomal recessive disease associated with mutations in the FHL1-5 gene. Mutations in the FHL1-5 gene can cause autosomal recessive illnesses that can have a variety of health effects on different organ systems. These could include irregularities of the heart, muscles, and skeleton, as well as possible effects on general mobility and function. Although the symptoms may differ, affected individuals frequently face serious health difficulties as a result of these genetic abnormalities. It primarily includes immunodeficiency-associated and familial phagocytic lymphohistiocytosis, although immunodeficiency-associated phagocytic lymphohistiocytosis is primarily associated with genetic mutations and primary immunodeficiency. Secondary hemophagocytic lymphohistiocytosis (HLLC) was first described by Chandra et al. in 1975 [2] and includes tumor-related, infection-related, autoimmune disease-related, post-transplant and drug-related hemophagocytic lymphohistiocytosis [3]. Secondary phagocytic lymphohistiocytosis can occur at any age, and the main causes of secondary phagocytic lymphohistiocytosis are tumors and infections, with secondary tumors, infections, and autoimmune diseases in adults and viral and bacterial infections in children being the most common causes. M-HLH is usually caused by hematologic tumors, but less frequently by solid tumors M-CLD can be divided into tumor-induced CHF and chemotherapy-related CHF. Although the mechanism is not well understood, chemotherapy-related HLH is thought to be related to pathogenic infection due to immunodeficiency after tumor chemotherapy, while tumor-related HLH is thought to be related to invasive metastasis of the malignancy, cytokine secretion by the tumor cells themselves, and viral infection. A Swedish single-center study reported an annual incidence of M-HLH of approximately 3.6 million, with an age-independent incidence, higher in adults and relatively low in adolescents and children [4, 5]. Other studies have also reported the occurrence of M-CLD in children, again less frequently than in adults [6]. However, with the growing awareness of M-HLH in children and adolescents, it should not be overlooked: there are few studies on the treatment of M-HLH and no single treatment protocol that indicates whether to direct initial treatment to GLH, chemotherapy for malignancy, or both Although there is no single protocol, many researchers believe that if initial treatment is directed toward GLH, chemotherapy should be given according to tumor type and then chemotherapy should be given to the tumor once GLH is under control [7]. Certainly, chemotherapy for malignant diseases often results in side effects such as nausea, fatigue, hair loss, immune suppression, anemia, and gastrointestinal issues. Specific side effects depend on the drugs used and individual factors. The number of patients with M-HLH has been on the rise in recent years, and the study of its pathogenesis, clinical features, and treatment is of particular importance to improve the diagnosis and prognosis of patients with the disease.
To further understand M-HLH, this paper selected 125 patients diagnosed with HLH admitted to our hospital from June 2015 to August 2021. According to different etiologies, they were divided into two parts: M-HLH and non-M-HLH. Analyzing clinical characteristics such as sex, age, myoglobin, NK cells, serum albumin, and direct bilirubin is necessary to distinguish M-HLH from non-M-HLH. Age-specific considerations are necessary due to the existence of variances in both pediatric and adult populations. The goals include better knowledge of HLH, increasing the accuracy of diagnosis, and customizing management. M-HLH emphasizes a dual strategy to better patient outcomes, with a focus on early cancer detection and treatment. Age-specific manifestation recognition improves clinical understanding and leads to more targeted therapy. The overall goals of this thorough analysis are to improve patient care techniques and progress the field of HLH. The general data, laboratory test results, survival, and other aspects of M-HLH and non-M-HLH groups were analyzed in three different groups, adults and children.
Materials and methods
General information
The related data of 125 patients diagnosed with hemophagocytic lymphohistiocytosis admitted from our hospital from June 2015 to August 2021 were collected.
Inclusion criteria
The included patients all met the diagnostic criteria of HLH-2004 established by the International Society of Histology and Cells. Inclusion criteria for children: age
Diagnostic criteria
HLH-2004 diagnostic criteria: finding associated HLH molecular genetic abnormalities or meeting 5 of the following 8 diagnostic criteria: fever; splenomegaly; hematocrit (two or three lines): hemoglobin M-HLH diagnostic criteria According to tissue and organ biopsy and immunohistochemical staining, the type of malignant tumor must be determined, and the diagnostic criteria of HLH-2004 must be met. Epstein-Barr virus infection criteria One of the following two conditions can be diagnosed as EB virus infection.
Serological examination of EB virus VCA-lgM, EA-lgG positive; Real-time quantitative PCR detected EBV-DNA positive.
Demographic characteristics: gender, age; Clinical symptoms and signs: fever, splenomegaly, hepatomegaly; Blood laboratory tests: Muscle (CREA), Urea (UREA), fibrinogen (Fib), serum ferritin (SF), serum sodium (Na), bone marrow smear hemophagocytic cells, Epstein-Barr virus infection, peripheral blood T lymphocyte subsets (CD3*T cell ratio, CD4* T cell ratio, CD8*T cell ratio, NK cell ratio); Laboratory examination of etiology: hematological malignancies, non-hematological malignancies (infection-related HLH, rheumatism-immune-related HLH); Outcome of the disease: survival.
The 125 patients should be divided into two parts: M-HLH and non-M-HLH groups, and the age, sex, WBC, Hb, PLT, and GGT of the two groups were compared from three groups: general, adult, and children. LDH, ALB, DBIL, IBIL, TG, CREA, UREA, Fib, SF, Na, bone marrow hemophagocytosis, Epstein-Barr virus infection, peripheral blood T lymphocyte subsets (CD3*T cell ratio, CD4*T cell ratio, CD8 *T cell ratio, NK cell ratio) and other indicators and prognosis, and statistical analysis was performed.
Statistical methods
The enumeration is described in terms of number and percentage. The method was used to describe the median (interquartile range). The ROC curve was used to screen the optimal cutoff value for the proportion of NK cells. To find the ideal cutoff value for the fraction of NK cells, the ROC curve is a useful tool. The cutoff is selected to optimize diagnostic accuracy by taking into account the intended trade-off between genuine positives and false positives. Sensitivity and specificity are balance factors in this process. Hyperferritinemia, cytopenias, hypertriglyceridemia, hypofibrinogenemia, and signs of hemophagocytosis in bone marrow or other tissues are often important diagnostic criteria for diagnosing and validating hemophagocytic lymphocytosis in patients. Elevated soluble interleukin-2 receptor levels and aberrant natural killer cell activity could be additional requirements. Logistic regression was used to screen independent related factors of M-HLH, and a multivariate COX regression model was used to screen independent risk factors affecting survival. Kaplan-Meier evaluation and Log-Rank test were used for survival time. Both statistical methods, which support many predictor variables and categorical outcomes, are applied in survival analysis. Clinical research uses them to predict binary outcomes and analyze time-to-event outcomes. They also entail statistical testing for significance, parameter estimation, and the assumption of proportional hazards (in the case of COX regression). Even though these models are similar, there are variances in their underlying assumptions and specific applications, which highlight the significance of choosing the right model according to the study setting. An expansion of the Cox proportional hazards model used in survival analysis is the multivariate Cox regression model. In the fundamental model, an event’s risk is expressed as the product of an initial risk and the exponential of the covariate coefficients. This is expanded upon in the multivariate form to encompass numerous predictor variables, enabling the concurrent analysis of their combined impact on the hazard. Hazard ratios are frequently used in interpretation to show the ratio of dangers for various covariate levels. Proportionate hazards and the lack of unmeasured confounding are among the assumptions. Due to their non-parametric nature and lack of assumption on a particular survival time distribution, the Kaplan-Meier estimator and Log-Rank test are utilized in survival time analysis. It is possible to analyze censored data and time-to-event outcomes using them because they are reliable methods for calculating survival curves and comparing survival distributions among groups, without putting a lot of pressure on the underlying data distribution.
Demographic characteristics of patients with M-HL and non-M-HLH groups
Demographic characteristics of patients with M-HL and non-M-HLH groups
Demographic characteristics of patients.
Of the 125 HLH patients, 70 (56%) were male and 55 (44%) were female. There were 39 M-HLH patients, 28 males (71.6%) and 11 females (28.5%), male to a female ratio: of 28:11. There were 86 non-M-HLH patients, including 42 males (47.7%) and 44 females (52.3%), with a male-to-female ratio of nearly 1:1.125 HLH patients. The youngest age was 0.25 years, the oldest was 75 years old, and the median age was 7 years old. The youngest age of M-HLH patients was 2 years old, the oldest was 68 years old, and the median age was 19 years old. The minimum age of non-M-HLH patients was 0.25 years, the maximum age was 75 years, and the median age was 4 years (see Table 1 and Fig. 1 for details).
Etiological characteristics of 125 patients
Etiological characteristics of 125 patients
Etiological characteristics.
Among the 125 HLH patients, 39 were M-HLH patients, including 33 lymphomas, 4 leukemias, and 2 myelodysplastic syndromes. There were 86 non-M-HLH patients, including 80 infection-related HLH and 6 rheumatic immunity-related HLH (see Table 2 and Fig. 2 for details).
More than 90% of the patients had fever and markedly elevated ferritin, 62.50% had hepatomegaly, 56.00% had splenomegaly, and 56.00% had hemophagocytosis in the bone marrow, and hemoglobin
The clinical manifestations and laboratory indicators of 125 patients who met the diagnostic criteria
The clinical manifestations and laboratory indicators.
WBC, Hb, PLT, GGT, ALP, TG, LDH, Na, CD3*T cell ratio, CD4*T cell ratio, CD8*T cell ratio, UREA, Fib in M-HLH and non-M-HLH groups in the general population, SF, bone marrow hemophagocytic phenomenon, EB virus infection had no statistical difference (
Comparison of M-HLH and non-M-HLH demographics and laboratory results in the overall population
Comparison of M-HLH and non-M-HLH demographics and laboratory results.
Gender, WBC, Hb, PLT, GGT, ALP, ALB, TG, LDH, Na, CD8*T cell ratio, there was no significant difference in CREA, UREA, Fib, SF, bone marrow hemophagocytosis, and Epstein-Barr virus infection (
Comparison of M-HLH and non-M-HLH demographics and laboratory results in children
Comparison of M-HLH and non-M-HLH demographics and laboratory results in children.
Gender, age, WBC, Hb, PLT, GGT, ALP, ALB, TG, LDH, Na, CD3*T cell ratio, CD8*T cell ratio, CREA, UREAFib in M-HLH and non-M-HLH groups in the adult group. However, there is no difference here in IBIL, CD4*T cell ratio, or NK cell ratio between M-HLH and non-M-HLH patients between the two groups. Multivariate Logistic regression analysis of the factors with differences in ALT, AST, DBIL, IBIL, CD4*T cell ratio, and NK cell ratio showed that none of the factors were associated with M-HLH (see Table 6 and Fig. 6 for details).
Comparison of M-HLH and non-M-HLH demographics and laboratory results in adult groups
Comparison of M-HLH and non-M-HLH demographics and laboratory results in adult groups.
Our group of patients with hemophagocytic lymphohistiocytosis were patients hospitalized in our hospital for 1 month and included 1 male and 1 female, aged 1 year with a median of 10 years. All patients with histiocytic lymphocytosis had hyperthermia between 1∘C and showed varying degrees of hemophagocytosis in the bone marrow with varying proportions of hemophagocytosis. The patient had hepatosplenomegaly. The incidence of peripheral thrombocytopenia was 1, median platelet, 1, median white blood cell, and 1, median hemoglobin age. The incidence of hypertriglyceridemia was higher than the incidence of hypofibrinogenemia. The main causes of hypertriglyceridemia, which is more common than hypofibrinogenemia, include sedentary lifestyle choices and poor diets that raise triglyceride levels. Hypofibrinogenemia is relatively uncommon and can be caused by either acquired or hereditary reasons, including liver illness or specific drugs. In contrast, hypertriglyceridemia is frequently linked to modifiable risk factors. The increased prevalence of hypertriglyceridemia in the general population is partly explained by lifestyle-related factors. Serum ferritin was elevated and variable, with more than half of the patients exhibiting ferritin values surpassing a specified threshold. Over half of individuals have ferritin readings over a threshold due to underlying illnesses such as hemophagocytic syndromes, infections, inflammations, or malignancies, which can raise ferritin levels as part of the body’s immunological response. In healthy individuals, serum ferritin secretion and expression are affected by cytokine activity and inflammation, while iron levels control serum ferritin levels. By holding extra iron and releasing it when needed, ferritin contributes to iron homeostasis. During the acute-phase response, ferritin synthesis can be stimulated by inflammation and cytokines, leading to higher blood ferritin levels. Patients in the cases had viral seropositive findings. Virus-positive cases, cytomegalovirus positive cases. In patients with hemophagocytic lymphocytosis, the final diagnosis was lymphoma, infection, kala-azar, autoimmune disease, and unknown cause. All patients with kala-azar disease were diagnosed by bone marrow smear and cured by antimony treatment. The diagnosis of visceral leishmaniasis, or kala-azar, is made using bone marrow smears, in which Leishmania parasites are identified and detected under a microscope using Giemsa staining. The goal is to detect the amastigote form inside macrophages; measuring the parasite burden helps determine the extent to which the infection exists. These measurements on bone marrow smears are crucial for a precise diagnosis, which guides suitable kala-azar treatment plans. The dosage, length of treatment, patient demographics, and any side effects that may have been noticed are all covered in the supplemental data on antimony treatment. A thorough assessment of the antimony treatment’s effectiveness and safety profile would also be possible with the inclusion of data on treatment response rates and follow-up times. The remaining patients received hormonal, gamma globulin, anti-infective, and antiviral therapy, and some patients with malignant disease used chemotherapy on top of this.
Contrast-enhanced CT of the abdomen revealed nodular enhancement in the upper jejunum, which was considered a vascular malformation. and arrow points.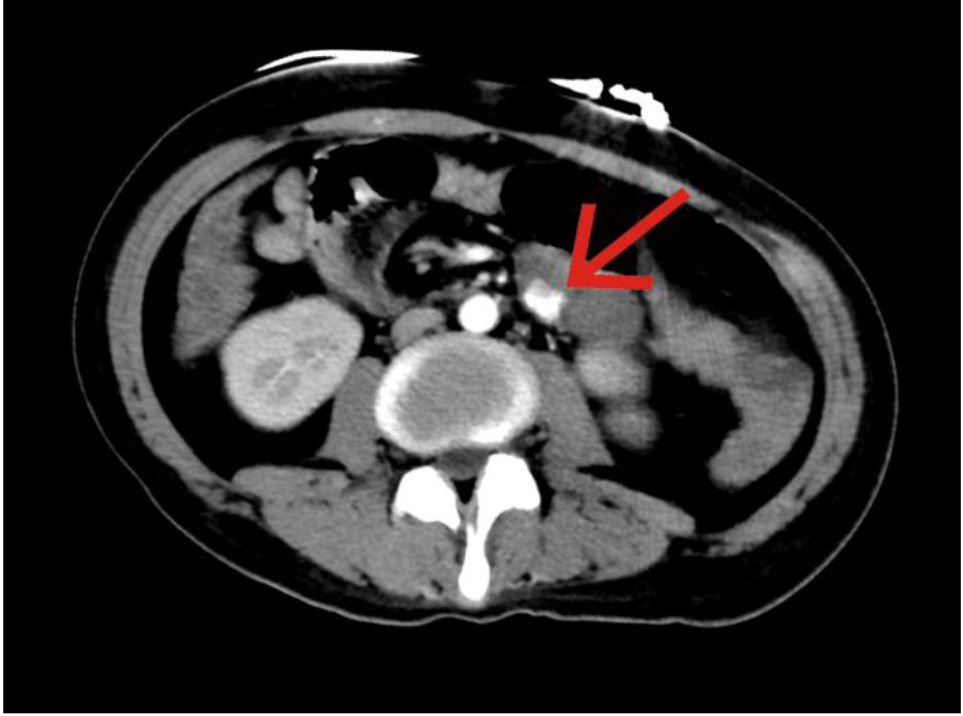
Bone marrow biopsy showed a huge number which is about EBER-positive T lymphocyte infiltration with hemophagocytic, considered as a T-lymphocyte proliferative disease which has a relationship with to severe EBV infection.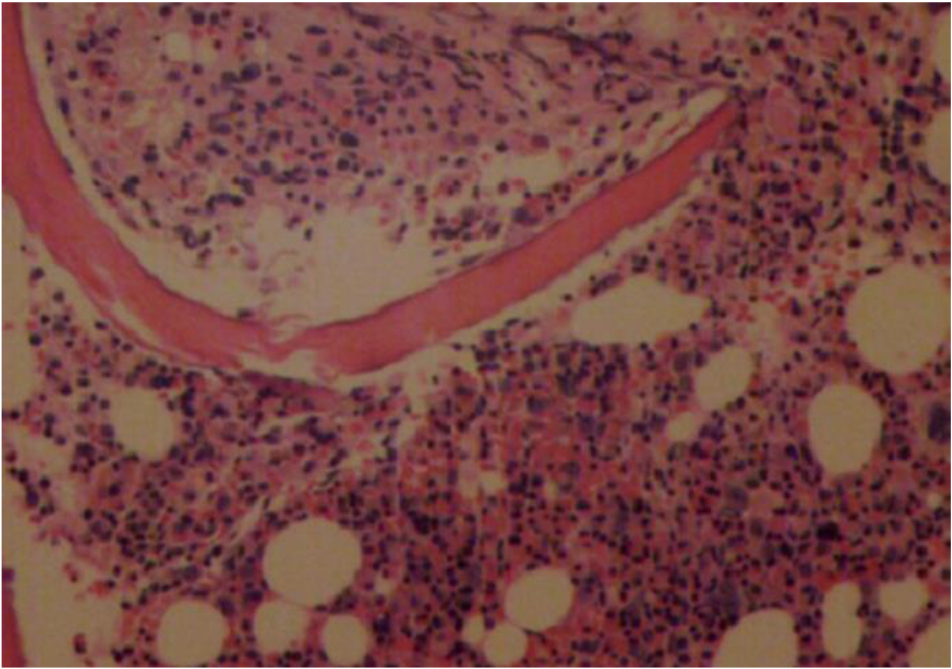
Hemophagocytic lymphocytosis is a common clinical syndrome that occurs equally in men and women, with a slightly higher incidence in males than in females, as seen in the present case data. Secondary hemophagocytic lymphocytosis is more common in young people and its occurrence is associated with viral infection. Hemophagocytic lymphocytosis in adults is the most common tumor-related disorder. Treating the underlying cancer, using immunosuppressive medication with caution, keeping an eye on symptoms of hyperinflammation, monitoring organ failure and cytopenias, and providing supportive care are important factors to take into account when diagnosing and treating secondary hemophagocytic lymphocytosis in adults with tumor-related disorders. For complete management, regular cooperation between hematologists and oncologists is crucial. In this patient population, the causes of hemophagocytic lymphopenia are, in order of frequency, viral, bacterial, mycoplasmal, Down’s syndrome and other infectious diseases, cellular lymphomas, autoimmune diseases, and other neoplastic diseases. Symptoms often begin with fever, hepatosplenomegaly, and associated stage III cytopenia. The disease progresses quickly, patients often have progressive disability, and symptoms associated with liver failure often appear late in the disease. The prognosis is directly dependent on the underlying disease. Liver failure symptoms associated with HLH include hepatomegaly, jaundice, increased liver enzymes, coagulopathy, and hepatic dysfunction. The aforementioned signs are a result of hyper-immune activation and cytokine release, underscoring the significance of prompt identification and intervention for enhanced outcomes. The prognosis and patient outcomes of M-HLH patients are greatly improved by early diagnosis. Prompt immunosuppressive therapy beginning in conjunction with timely detection and treatment of the underlying cancer can improve survival rates and reduce consequences related to organ malfunction and hyperinflammation. For M-HLH patients, improved outcomes require early intervention. In some patients, nonneoplastic hemophagocytosis may be associated with viral infection or protozoa. With hormonal therapy, immunosuppressive therapy, and etiologic therapy, hypereosinophilia can be controlled and even cured. Treatments for hypereosinophilia include immunosuppressive medication, which lowers the immune response, hormonal therapy, which controls hormone levels, and etiologic therapy, which aims to address the underlying cause of eosinophilia to effectively treat the condition. When the primary disease is poorly controlled, symptoms associated with hemophagocytic lymphocytosis may temporarily remit or improve with appropriate therapy, but the disease tends to recur and the prognosis is poor. The body experiences substantial improvements such as decreased fever, improved organ function, decreased cytopenias, and resolution of hemophagocytosis in tissues after therapies temporarily alleviate hemophagocytic lymphocytosis.
Serum ferritin is the major form of iron stores and is associated with a variety of physiological and pathological processes. Increased serum ferritin levels have been linked to effects such as organ damage and hyperinflammation in HLH and adult Still’s disease, as well as possible diagnostic markers for these illnesses. The expression and secretion of serum ferritin are affected by many stresses (1). Antibodies reduce the phagocytic capacity of granulocytes. Antibodies, like anti-FC
Among 123 patients with HLH, the most common clinical manifestations were fever (100, 81.3%), followed by lymphadenopathy (53, 43.1%) and splenomegaly (51, 41.5%); the most common hematologic changes were thrombocytopenia (86, 70.0%), followed by anemia (49, 39.8%). The liver was enlarged (15, 68.2%), spleen (29, 56.9%), lymph nodes (29, 54.7%), and laboratory tests showed hypofibrinemia, with HLH being the most common (16, 64.0%), see Figs 7 and 8.
The proportions of serum ferritin above 10 000–19 999, 20 000–29 999, 30 000–39 999, 40 000–49 999, and 50 000
Age, gender, fever, disturbance of consciousness, initial ferritin, maximum ferritin, blood cell changes, aspartate aminotransferase (AST), total bilirubin (TBIL) between the two groups, direct bilirubin (DBIL), triglyceride.
HLH is a multisystem disease with severe immune dysfunction, usually occurring in an immunologically challenging environment, resulting in high mortality and a poor prognosis. When the body is immunologically challenged, the disease may be the result of a fundamental defect in the body’s immune system that results in an overactive but ineffective response of the compromised immune system. Disorders resulting from basic deficiencies in the immune system exhibit a variety of clinical presentations, including autoimmune disorders, inflammation, and recurring infections. The degree of symptoms varies according to the particular defect, highlighting the necessity of a precise diagnosis for customized treatment. Because the body’s immune response cannot adequately eliminate cytokine stimulation, the immune system does not physiologically downregulate in response to constant cytokine stimulation, resulting in a vicious cycle of increased cytokine release and increased immune activation. It is difficult to manage conditions involving immune dysregulation and chronic cytokine stimulation because immunosuppression must be carefully balanced, long-term therapy side effects can occur, and underlying causes of immune activation that persist can’t be addressed. A continuous release of cytokines and an inability to restore homeostasis can result from the immune response of the body failing to effectively eliminate cytokine stimulation because of things like persistent inflammation, dysregulation of immune checkpoints, or an overwhelming and prolonged immune activation. M-HLH and other variants of HLH are similar in that they both have hepatosplenomegaly, cytopenias, and fever. However, certain clinical features, such as tumor-related fever, weight loss, and organ involvement, are frequently linked to the underlying malignancy in M-HLH. Accurate diagnosis and customized treatment depend on the identification of these characteristics associated with cancer. Instead, modern treatment aims to stop this vicious cycle by seeking out any triggering factors, reducing the immune response, and eliminating inflammatory factors with myelosuppressive and immunosuppressive therapy.
HLH is a relatively rare disease: according to global data including 2,197 patients with HLH [8, 9], the annual incidence is 1 per 800,000 population and 1–10 per 1 million children in Italy, Sweden, and the United States, the mean age at diagnosis is 50 years, 775 patients, over 50% from Japan and approximately 2–6% of patients with HLH have been proven to be from China. Compared with the present study, the mean age of 27 years in the present study is significantly lower, which may be due to the small number of cases in the present study and the inclusion of one-third of patients with mild HLH. The average age of diagnosis of VHL in adults is about 47 years and in children about 7 years, which is generally consistent with the above data.
In adults with the triad of hypothyroidism, splenomegaly, and hepatic disorder, the percentage of patients diagnosed with HLH reached 62.62%: 23%, 81.33%, 86.89%. One study [10] showed that the proportion of HLH patients increased with increasing ferritin levels in adult patients; in HLH patients, ferritin levels ranged from 1 000
The study compared the HLH and non-HLH groups and found statistically significant differences in liver, spleen, and lymph node enlargement, ALB, and Fib between the two groups (
HLH is a very dangerous disease, especially M-HLH, which progresses rapidly and has a very high mortality rate. Clinical studies require clinical data with a large sample size. Since we have a small number of cases, if we can increase our sample size and analyze M-HLH patients in detail, we will be able to provide more clinical data for the diagnosis and treatment of M-HLH, which will improve our understanding of M-HLH, improve the diagnosis and early treatment of M-HLH. improve the diagnosis of HLH and improve early treatment and patient prognosis.
Conclusion
Non-M-HLH survived significantly better than M-HLH. the proportion of NK cells was predictive of the diagnosis of M-HLH. In the overall population group, non-M-HLH was more likely to have abnormal liver function than M-HLH. Decreased platelet count and serum albumin levels were associated with poor prognosis, with lower platelet count and serum albumin levels associated with poorer prognosis. In addition, lower platelet counts and serum albumin levels were also associated with poor prognosis in the adult group.
Funding
There is no specific funding to support this research.
Data availability
All data generated or analyzed during this study are included in the manuscript.
Author contributions
The manuscript is mainly written by Cancan Lu. Huixian Hu was tasked with revising the manuscript, approved the final version, and is the article guarantor. Interpret data was tasked by Jimin Shi and Yamin Tan.
Footnotes
Conflict of interest
All authors related to this work do not have any conflicts of interest to report.