
Abstract
BACKGROUND:
Uncemented acetabular components are widely used in modern total hip arthroplasty (THA). Modularity has numerous advantages including the ability to use supplementary screw fixation for the shell, and allow to switch from ceramic to polyethylene (PE) bearings and vice versa, and the use of lipped and face-changing liners.
OBJECTIVE:
Despite these advantages, a problem with modular PE liners is dissociation. This is a rare complication in modern implants. The rate of liner dissociation is reported to be very low between 0.17% and 0.8%. Typical symptoms are sudden onset of groin pain in a previously well-functioning hip joint, followed by grinding or clicking sensations during hip joint motions indicating, that the femoral head is articulating with the metal acetabular shell rather than with the PE liner. Any newly observed noise or squeaking from a THA should undergo radiographic investigation to exclude liner dissociation.
CASE PRESENTATION:
We present the case of an 88-yearold male patient who developed PE liner dissociation in a cementless THA with a Pinnacle acetabular component six years after the index operation. We recommended revision of the left hip, which was performed two days later. In the interim, the patient was advised to use a pair of crutches. During revision surgery, it was observed that the metal head made contact with the cementless cup shell without damaging it from a macroscopic standpoint. Consequently, a simple exchange of the PE liner was conducted, and a 36 mm metal head was implanted due to scratches on the original head.
CONCLUSION:
Early diagnosis facilitates a straightforward exchange of the liner along with the head, potentially preserving the osseous integrated cup shell and stem integrity. Routine radiologic follow-up allows to distinguish between PE liner dissociation and severe PE wear.
Introduction
Uncemented acetabular components are widely used in contemporary total hip arthroplasty (THA). Most are modular, which has a number of advantages including the ability to use supplementary screw fixation, and allow ceramic and polyethylene (PE) bearings, different head sizes, and the use of lipped and face-changing liners [1]. However, modularity introduces the challenge of PE liner dissociation, a complication well- documented in older uncemented acetabular components [2]. Dissociation of the liner from the acetabular shell is a rare but severe complication in contemporary THA. Failure mechanisms encompass fatigue, wear, component placement and weakness of the liner locking mechanism. One reason might be new designs (e.g. offset liners vs. standard liners), new locking mechanisms or new PE materials (ultra-high-molecular-weight polyethylene (UHMWPE) vs. highly cross-linked polyethylene (HXLPE)) There have been reports of PE liner dissociation as well as ceramic liner dissociation [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20]. The incidence is low, with some authors reporting a frequency of 0.8% [3]. Although improvements in locking mechanisms nearly eradicated this problem, it has resurfaced with the advent of third-generation acetabular components [5, 7]. Initial cases primarily involved the Harris-Galante acetabular component (Zimmer, Warsaw, IN, USA), which has been replaced on the market with new generation prostheses [1, 5, 6, 7, 18]. This issue is rarely seen nowadays because of improved prosthetic designs. However, recent reports indicate a resurgence of liner dissociation with the latest prosthetic designs, suggesting an increased occurrence or improved recognition of this complication. The Pinnacle acetabular component (DePuy, Warsaw, IN, USA) has been associated with several cases of liner dissociation, to the extent that some authors consider it a specific complication associated with this implant type. In 2009, the first published case of DePuy Pinnacle liner dissociation was described by Mesko [13]. In the case of Mesko [13] a man suffered from PE liner dissociation twenty-three months postoperative when he arose from a squatting position in his garden. Surgical exploration revealed the polyethylene liner had spun out leaving the posterior, superior aspect of the shell exposed to the metal head. The cup and femoral anteversion were deemed acceptable. Neither screw was protruding, but instead was fully seated at the time of revision. The acetabular rim locking mechanism was judged to be uncompromised [13].
We present the case of an 88-yearold male patient suffering from PE liner dissociation in a cementless THA with a pinnacle cup, occurring six years after the index operation.
Case report
An 88-year-old male very sportive patient presented to our outpatient department with slight pain of the left hip and squeaking noise for the last day in November 2017. The day before, the patient dismounted from his bike and experienced a short sharp pain in the left hip, followed by the onset of a squeaking noise phenomenon. Six years prior, the patient underwent total hip arthroplasty (THA) for left hip osteoarthritis, utilizing a Tri-Lock stem (Size 6) and a cementless Pinnacle cup (Size 52) along with a polyethylene (PE) inlay and a 32 mm diameter metal head (DePuy, Warsaw, IN, USA). The liner was intended for used acetabular system. Regular X-ray follow-up was performed and showed no signs of loosening. The most recent follow-up in March 2017 was uneventful. The left hip was stable, there was no leg-length discrepancy, no swelling, irritation-free scar tissue, strong pelvitrochanteric muscles, the range of motion (ROM) was excellent with extension/flexion 0/0/120∘, abduction/adduction 40/0/40∘, and external/internal rotation 40/0/40∘. X-Ray imaging of the left hip showed an uncemented total hip, correct position of the implants, absence of radiolucent lines and good head centration (Fig. 1).
X-ray of the left hip in 2 planes (most recent imaging 6 months before the current presentation): ap view (a) and lateral view (b) showing a cementless total hip arthroplasty without radiolucent lines and good centration of the metal head within the PE liner.
Current clinical examination of the left hip in November 2017 showed no swelling, irritationfree scar tissue after anterior minimal invasive approach, leg length shortening of about 1 cm on the left side, no local tenderness and a good ROM with extension/flexion 0/0/100∘, abduction/adduction 25/0/25∘ and external/internal Rotation 40/0/20∘. During ROM testing, squeaking was detected. X-ray imaging of the left hip showed an uncemented total hip and no radiolucent lines but definite decentration of the head, suggesting a PE liner dissociation (Fig. 2).
X-ray of the left hip in 2 planes (at the current presentation): ap view (a) and lateral view (b) showing a cementless total hip arthroplasty without radiolucent lines and definite decentration of the metal head.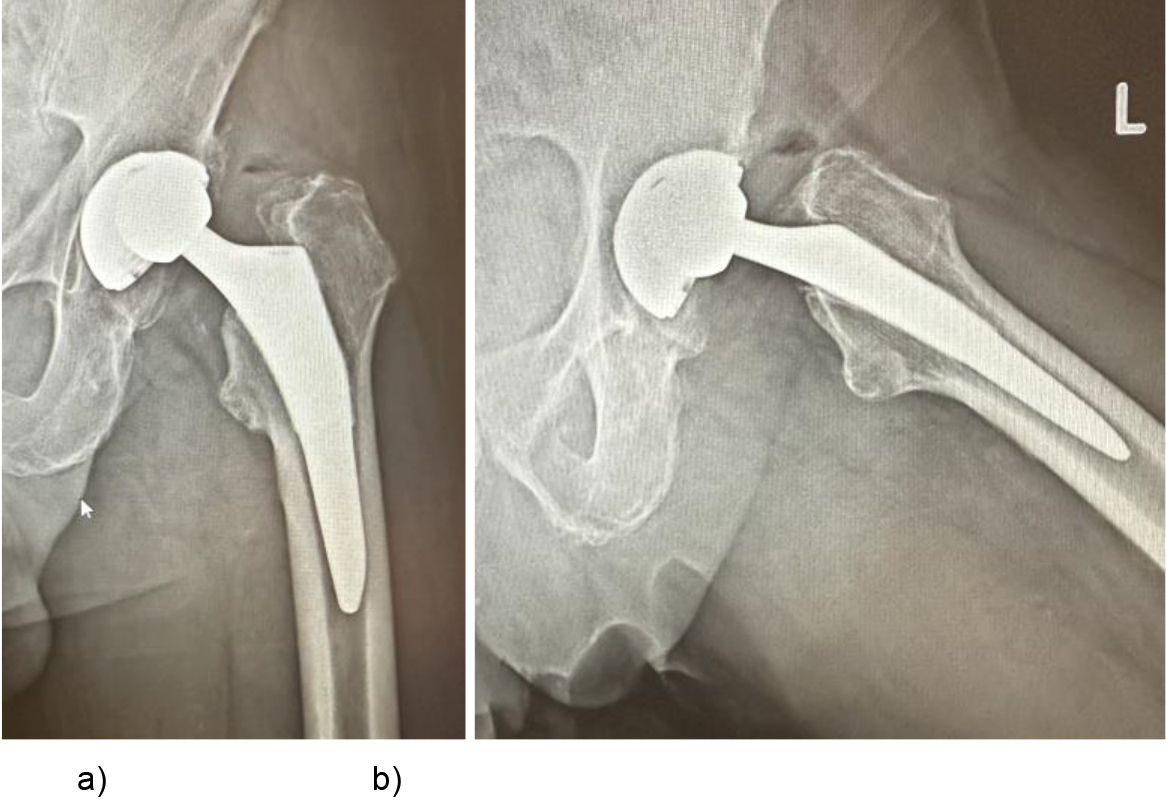
We recommended revision of the left hip via a posterior approach, which was performed two days later. In the interim, the patient was advised to use a pair of crutches. During revision surgery, it was observed that the metal head made contact with the cementless cup shell without damaging it from an macroscopic standpoint. Consequently, a simple exchange of the PE liner was conducted, and a 36 mm metal head was implanted due to scratches on the original head. We used a metal head for revision surgery in respect to the age of the patient, despite a ceramic revision head with a titanium adapter sleeve should have been used according to guidelines.
Six years post-revision the patient is free of any complaints, and X-ray imaging of the left hip shows an uncemented total hip without radiolucent lines and a good centration of the 36 mm diameter metal head (Fig. 3).
X-ray of the left hip in 2 planes (after surgical revision): ap view (a) and lateral view (b) showing a cementless total hip arthroplasty without radiolucent lines and good centration of the metal head within the PE liner.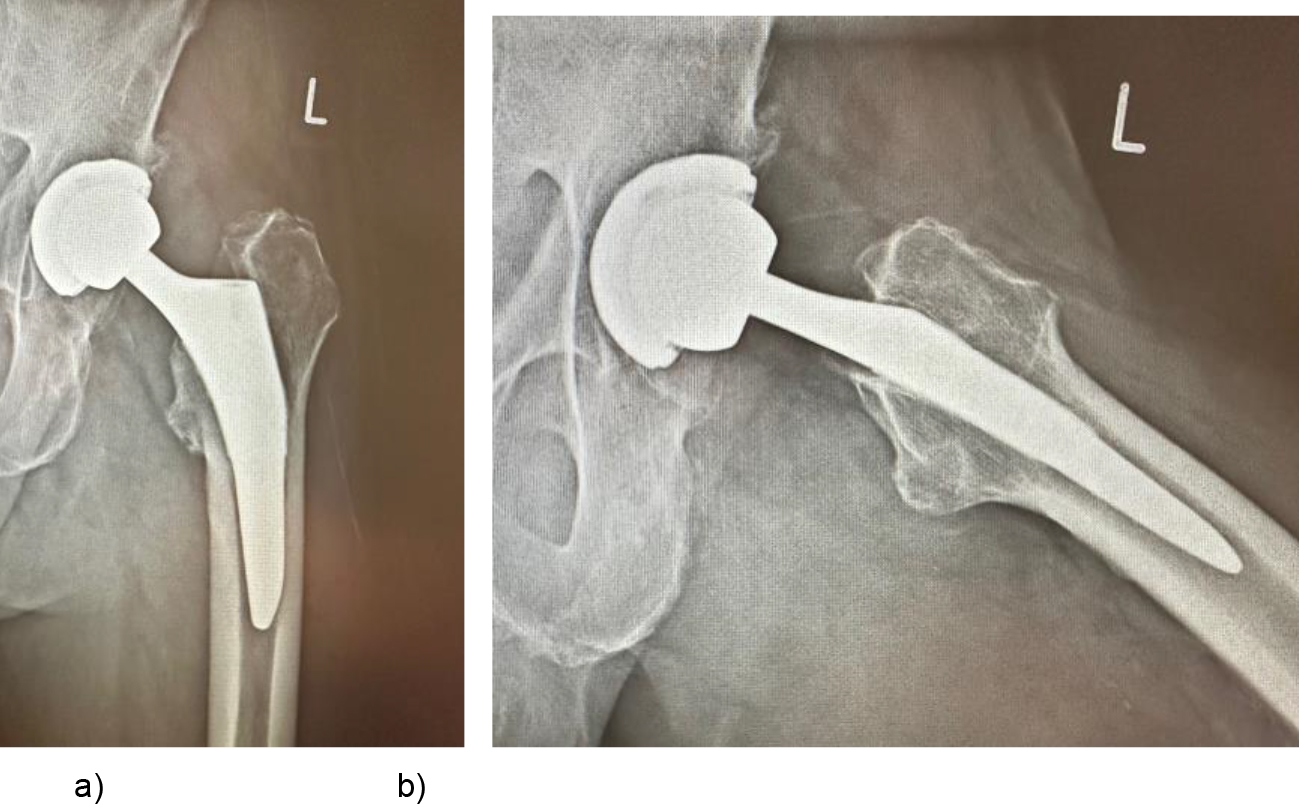
Dissociation of the liner from the acetabular shell is a rare yet severe complication in THA. Numerous case reports and series have documented instances of liner dissociations associated with the Pinnacle cup [1, 8, 9, 13, 19, 20]. These dissociations can manifest either early (within two years) or late (two to ten years) [11, 12]. Dissociations occurring in the early postoperative period are likely attributable to inadequate seating of the PE liner and failure of the locking mechanism of the acetabular component. In contrast, late dissociations are thought to result from either femoral neck impingement against the PE liner or edge loading, resulting in fatigue failure of the locking mechanism [16]. In our presented case we encountered a late liner dissociation in a highly active and very sportive patient engaged in daily cycling activities (7 days per week). We hypothesize that the substantial stresses exerted on the liner-locking mechanism during sporting activities, coupled with potential impingement, contributed to the liner dislocation in this case. Although the rate of liner dissociation with the Pinnacle system is reported to be very low, ranging between 0.17% and 0.8% between 12 and 14 years, the likelihood of underreporting, especially in registry studies, cannot be dismissed [1, 20]. Vigilance in recognizing and reporting such complications is crucial for a comprehensive understanding of the true incidence and contributing factors associated with liner dissociation in THA.
Historically, liner dissociation was more common with first-generation acetabular designs such as the Harris-Galante (Zimmer) cup, thought to be due to failure of the locking mechanism. Second-generation cementless acetabular cups retained successful ingrowth surfaces from earlier designs and incorporated congruent contact between the liner and shell. While these cups demonstrated compatibility with ultra-high-molecular-weight polyethylene (UHMWPE), the introduction of highly cross-linked polyethylene (HXLPE) to enhance wear characteristics resulted in several reported cases of rim fracture. Rim fracture was thought to be a consequence of chronic impingement of the femoral neck against the elevated PE, eventually leading to fatigue failure of the PE and subsequent dissociation. To address these issues, third-generation designs were developed to reduce the risk of liner rim fracture. High stresses at the liner-locking mechanism are reduced by eliminating PE protruding above the rim, minimizing sharp corners at the liner-locking mechanism, and recessing the locking mechanism into the interior of the metal shell [1]. The consensus among most surgeons and company representatives is that incorrect seating of the PE liner is a primary cause of dissociations. Other suggested reasons for dissociation may include malposition of the shell, use of face-changing liners, impingement, PE fatigue, and rim fracture with thin PE and larger heads [4, 7, 8].
The occurrence of this event may be linked to trauma, but it can also manifest spontaneously. Patients typically report abnormal sounds and squeaking, a grating sensation, relative shortening of the operative leg, or alterations in the gait pattern [4].
Typical symptoms involve the sudden onset of hip pain in a previously well-functioning prosthesis, followed by grinding or clicking with hip movements as the prosthetic femoral head articulates with the metal acetabular shell instead of the PE liner [15].
Upon examination, notable limb shortening or restricted internal rotation is commonly found with a posteriorly dislocated THA. Audible grinding or clicking is reproduced with hip movements, provided that pain allows.
Radiographs obtained in cases of PE liner dissociation reveal abnormal eccentric articulation with superolateral migration of the femoral head into the shell on the anteroposterior view (AP), and medial migration of the femoral head in the lateral view is usually confirmatory. In contrast to PE liner dissociation associated with PE wear, these changes are abrupt, as seen in our case. The PE can be seen as a radiolucent ring in some cases (“bubble sign”/“crescent sign”). When in doubt, CT scans, MRIs, and ultrasounds are utilized for confirmation of the diagnosis [4, 15]. In certain cases hip arthroscopy can be performed in cases of doubt if the orthopedic surgeon is familiar with hip arthroscopy. The comparison of current radiographs with previously normal X-rays on Picture Archived Communication Systems (PACS) can also be a valuable tool in aiding the diagnosis [15].
A CT scan can be helpful to locate the displaced radiolucent PE, however, beam hardening artifacts may obscure some details. The displaced PE can be seen inferiorly below the capsule or posterior joint recess/greater trochanteric bursa or may be partially associated with the shell.
On MRI, Metal Artifact Reduction Technique Sequence (MARS) can enhance diagnostic confidence compared to routine pulse sequences. MRI with MARS is often superior in providing clearer visualization of the PE compared to other diagnostic modalities [4]. An arthrogram can also serve to confirm the diagnosis [4].
Sonographic evaluations have also been described, typically performed with the patient supine to assess the presence or absence of parallel double hyperechoic lines, which are termed “sonographic tram track signs” [4]. However, in most cases, plain radiographs with a clinical history of the sudden onset of a squeaking sound are usually confirmatory [4, 15].
In a systematic review Ciolli et al. [5] demonstrated that liner dissociation is a complication affecting adult patients (mean age of 56.5, ranging from 31 to 75 years), comprising both genders (53% female and 47% male) after a mean delay from the replacement surgery of almost four years (mean delay of 45.8 months, ranging from 0 to 120 months).
Liner dissociation is a rare but severe mechanical complication of modular THA, necessitating immediate implant revision. This complication seems to be not related to a specific prosthetic implant, liner material or design, surgical approach, or acetabular positioning within the safe zone. 60 dissociations were reported for polyethylene liner combinations. Manufacturer frequency in the study of Napier et al. [5] was: 21 Pinnacle (DePuy) dissociations, and 39 non-Pinnacle (10 Trident (Stryker), 6 CSF (Furlong JRI), 6 Trilogy (Zimmer) and 17 others) [1]. PE liner dissociation has been reported for several other implants from other companies, such as S-ROM (Depuy Synthes, Warsaw, IN, USA), ABS or AMS-HA (Kyocera, Med, Osaka, Japan), Trident (Stryker, Mahwah, NJ, USA), R3 or EP-FIT PLUS (Smith & Nephew, Memphis, TN, USA), Bencox (CorenTec, Seoul, Korea), Dynasty (Wright Medical Technology Inc, Arlington, TN, USA) and Maxera (Zimmer, Warsaw, IN, USA) [5].
Liner dissociation typically occurs in the absence of trauma. Revision of the cup is required in almost 40% of patients, while in few cases a revision of the stem is necessary [4]. Metallosis may be associated with liner dissociation, particularly in cases of delayed diagnosis. It is crucial to consider liner dissociation as a potential complication in THA. If left unaddressed for an extended period, metallosis can set in, leading to extensive damage to local tissue. During the early postoperative period, the diagnosis can be challenging to make, as patients may still bear weight and walk on the affected joint, and the pain they experience may be easily confused with postoperative pain [4].
Conclusion
The occurrence of any new noise or squeaking from a polyethylene (PE) liner in total hip arthroplasty (THA) warrants radiographic investigation to rule out liner dissociation. An early diagnosis facilitates a straightforward exchange of the liner, coupled with replacement of the head, thus preserving the integrity of the stem and cup. Regular radiologic follow-up is instrumental in distinguishing between PE liner dissociation and severe PE wear.
Footnotes
Conflict of interest
None to report.