
Abstract
BACKGROUND:
Wound complications after lumbar spine surgery may result in prolonged hospitalization and increased morbidity. Early identification can trigger appropriate management.
OBJECTIVE:
The aim of this study was to investigate the efficacy of infrared-based wound assessment (FLIR) after lumbar spine surgery in the context of identifying wound healing disorders.
METHODS:
62 individuals who underwent lumbar spine surgery were included. The immediate postoperative course was studied, and the patient’s sex, age, body mass index (BMI), heart rate, blood pressure, body temperature, numeric rating scale for pain (NRS), C-reactive protein (CRP), leukocyte, and hemoglobin levels were noted and compared to thermographic measurement of local surface temperature in the wound area.
RESULTS:
Measurement of local surface temperature in the wound area showed a consistent temperature distribution while it was uneven in case of wound healing disorder. In this instance, the region of the wound where the wound healing disorder occured had a lower temperature than the surrounding tissue (
CONCLUSIONS:
This study demonstrates the ongoing importance of clinical wound assessment for early detection of complications. While laboratory parameter measurement is crucial, FLIR may serve as a cost-effective supplemental tool in clinical wound evaluation. Patient safety risks appear minimal since local ST is measured without touch.
Introduction
Within the last decades, there was significant increase in spinal surgery due to numerous circumstances [1]. While it may be recommended for a variety of reasons, the most common root cause for performing spine surgery is decompression and stabilization of spinal and neuronal structures. Apart from acute care surgery there is also large number of indications for elective surgery. In general, clinical results are very good to excellent, high patient satisfaction is also evident in the long term [2, 3].
Nevertheless, surgical procedures on the spine are associated with numerous perioperative complications. Incidences are variably reported in literature between 16% and 51% [4]. Although the improvement of perioperative management due to increasing availability of diagnostic methods has led to a substantial reduction of complications related to spine surgery, they are still of enormous clinical relevance. Greatest possible minimization of complications is essential due associated increased morbidity and prolonged hospitalization [5, 6, 7, 8, 9, 10, 11].
In general, all patients undergoing surgery are at risk of surgical site infection (SSI). Especially posterior surgical access in spine surgery is associated with adverse healing events including wound and sutured dehiscence as well as higher SSI rate [12]. While increasing mortality, important economic factors such as the need for more intensive wound management, higher medication costs due to use of antibiotics and ultimately higher re-operation rates must be considered here [13]. In order to prevent postoperative complications or to detect them at an early stage, routine checks of vital signs and laboratory parameters as well as clinical wound checks are performed. Radiological procedures are used in cases of justified suspicion.
Wound and tissue healing is defined as biological event replacing damaged or dead tissue with new viable tissue. Adequate oxygenation and aerobe metabolism due to tissue perfusion is necessary for propriate wound healing. Objective assessment in clinical setting may be difficult due to different evaluation depending on personnel and experience [14]. A non-invasive method for assessing surface temperature and thus indirectly tissue perfusion is infrared measurement [15]. Forward looking infrared thermography (FLIR) has already been used in the context of burn wound assessment [16]. This study evaluated the diagnostic use of FLIR in context of surgical site infection after spine surgery. Primary objective of this study was to investigate whether FLIR can be used to detect wound complications at an early stage by assessment of local surface temperature (ST) in wound area. The secondary objective was to investigate specific patient characteristics and the development of clinical and laboratory parameters after lumbar spine surgery depending on the thermographic finding. In addition, it was investigated whether a relation to the respective thermographic measured local ST in the wound area can be determined.
Materials and methods
Study cohort
A total of 62 patients undergoing lumbar spine surgery in our department were enrolled in the study. The immediate postoperative course (defined as seven days after surgery) was observed and the following patient characteristics and parameters were recorded: Sex, age, body mass index (BMI), heart rate/min, blood pressure, body temperature, numeric rating scale for pain (NRS), as well as CRP, leukocyte and hemoglobin levels. The defined number of patients was based on assessment of the following factors: Estimated recruitment time of the patient collective, performance of the surgery by the same surgical team and measurement of ST by only one applicant ensuring standardized experimental conditions.
Experimental set-up
Thermographic measurement of local ST in the wound area was performed using a smartphone-based camera (FLIR ONE Gen 3), (Fig. 1a and b). The measurements were taken by the same and single person (LW) under standardized conditions at a skin-to-camera distance of approximately 30 cm–45 cm. Measurements were not taken immediately after patients got out of bed so that skin surface was not overheated. Numerous test measurements were carried out beforehand in order to obtain optimal and reproducible measurements, and similar conditions have already been described in other studies [17].
Visualization of thermal radiation through skin surface by FLIR. Color spectrum and associated temperature scaling is demonstrated on the right. A: Standard imaging of wound area. B: Reduced thermal emission due to lower tissue perfusion in caudal wound area gets visible.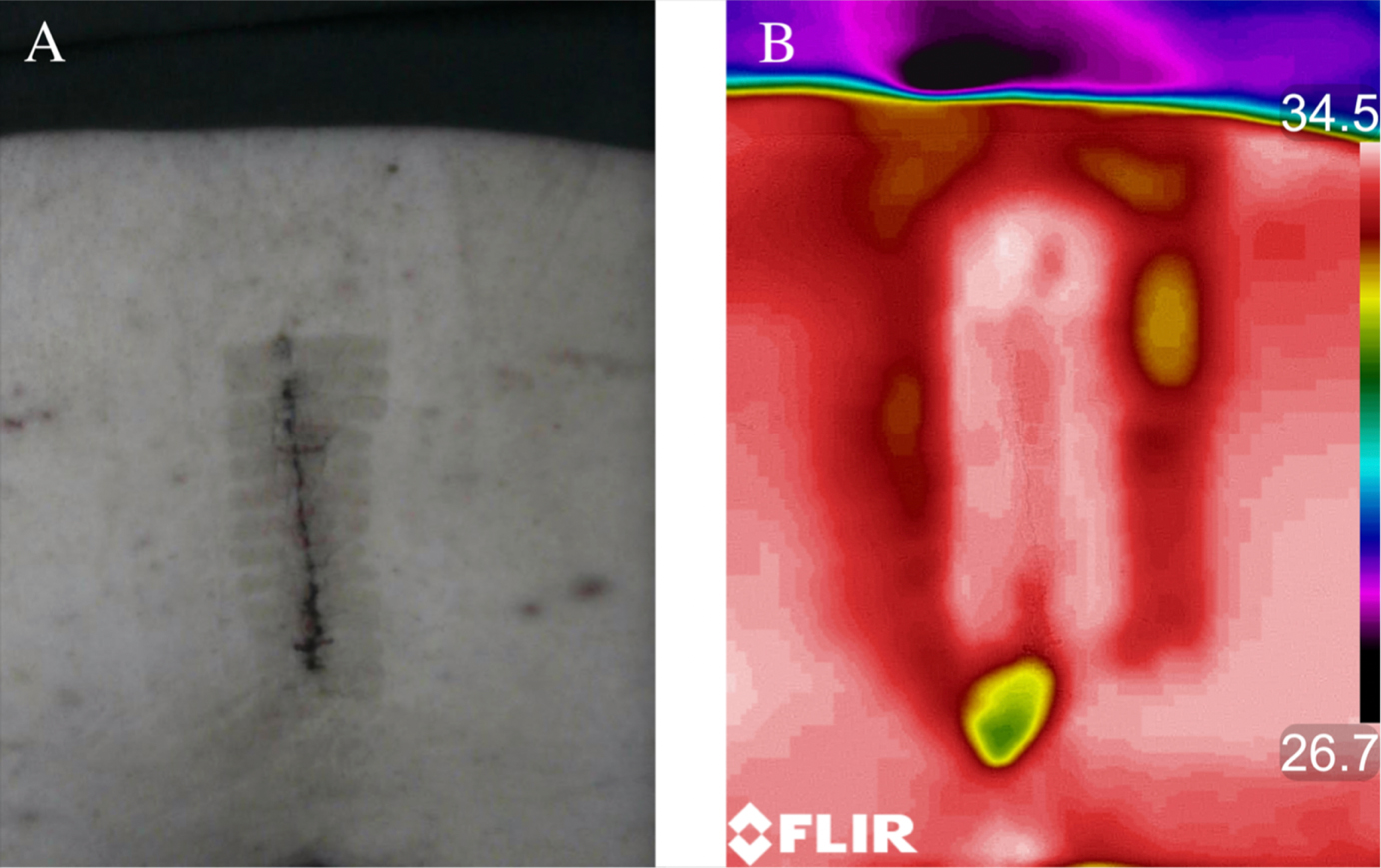
Temperature was measured in three regions of interest (ROI): Proximal, medial and caudal third of wound surface. Evaluation was performed using the associated software (FLIR Tools). Mean values of the measured surface temperature in ∘C were evaluated in each case.
Patients undergoing inpatient stay after lumbar spine surgery with surgical access from posterior. Patient age had to be
Exclusion criteria
Exclusion criteria were defined as acute postoperative deterioration of the clinical condition, intensive care unit stay, occurrence of any cardiopulmonary complication as well as insufficient mobilization of the patients. Patient’s withdrawal from the study was possible at any time without giving reasons.
Data collection
Medical data were collected and stored electronically. Pseudonymization was strictly ensured.
Statistics
Statistical analysis was performed using SPSS V28 software (SPSS Inc., Chicago, IL, USA).
Descriptive statistics were used to determine the mean and range of the data. Test data were assessed with the Kolmogorov-Smirnov and were found out to lack a normal distribution.
The Mann-Whitney U test was used to identify sex related differences among the measurements.
As the ST of the surgical site is the key factor analysed in this study, we performed a Kendall’s Tau test to determine the correlation of the ST measured on each study day with the respective secondary measurements. Therefore, non-parametric tests were employed for analysis. The level of significance was defined as a
Results
A total of 62 patients with a mean age of 67.5 years (range: 21–89) were included. Of the 62 patients, 28 (45.16%) were male, with a mean age of 69.4 years (range 36–85), and 34 (54.8%) were female, with a mean age of 65.2 years (range 21–89).
The most common surgical procedures undergone by the study population (
62)
The most common surgical procedures undergone by the study population (
Surgical procedures were listed as follows (Table 1). The mean height and weight were 1.67 m (range 1.49–1.94 m) and 80.5 kg (range 50.0–133.0 kg) respectively. The mean body mass index was 28.9 kg/m2 (range 20.5–50.1 kg/m2).
The ST showed a sex related difference on day one (
We witnessed an increase in ST of surgical site within the first three days after surgery while peak was recognized on day three after surgery (mean 34.48∘C
Secondary measurements
The evolution of our primary parameter (ST) and our secondary parameters from prior to surgery until the fourth postoperative day have been graphically presented in Fig. 2, where D0 refers to the preoperative day and D1–D4 refer to the days after surgery. Statistically significant negative correlations between ST and Hb-level were found on the first, second and fourth postoperative days (
The evolution of primary parameter (ST) and secondary parameters from prior to surgery until the fourth postoperative day (the graphs have been scaled to data). D0 refers to the preoperative day and D1–D4 refer to the days after surgery. A: Skin temperature measured by FLIR, B: CRP blood level, C: Hemoglobin blood level, D: Leucocyte blood level; E: Body temperature.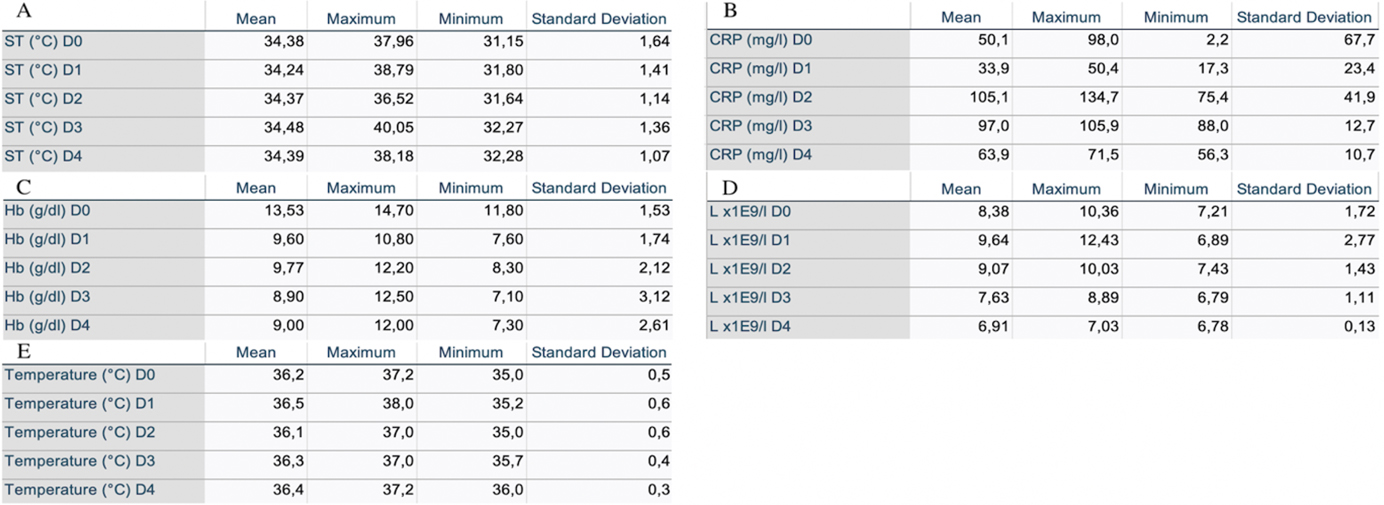
The level of CRP and leukocytes increased within the first two days after surgery. While CRP value reached its maximum at postoperative day two (mean 105.1 mg/l
Correlations between ST and CRP level were found on day one and day two after surgery (
Hb-level decreased after surgery within the first 3 days and was stable afterwards (mean Hb on postoperative day 3: 8.90 g/dl
Further significant differences between other measured parameters were found between day 0 and day 1 among NRS, systolic and diastolic blood pressures, CRP, leukocyte count and haemoglobin level with a
Significant differences were also found between day one and day two among the systolic blood pressure and diastolic blood pressure (
In this study, we investigated the measurement of local ST in the wound area after posterior lumbar spine surgery in context of wound healing complications. In addition, and in order to evaluate its suitability in clinical wound-assessment, laboratory parameters and vital signs were collected from patients respectively.
SSI is considered an important complication in spine surgery and is associated with both significant increased treatment costs and increased morbidity. Need for revision surgery and antibiotic therapy as well as prolonged hospital stay with risk for secondary complications are serious consequences.
The incidence of SSI is variable and is reported to range from 1% to 16% according to surgical procedure and approach [18, 19, 20, 21]. Although occurrence of wound healing disorders and SSI is caused by multiple factors, local tissue ischemia appears to be crucial. Sufficient perfusion and therefore supply with oxygen and nutrients of the whole wound area is proposed as a key factor in the healing process.
Monitoring of tissue perfusion after surgery is challenging due to lack of accurate diagnostic methods in clinical routine. It has already been shown that tissue oxygenation can be visualized by hyperspectral imaging and therefore the present technique can be used in wound examination [22].
In our study we demonstrated that smartphone based FLIR can detect local ST after lumbar spine surgery. In general, ST in surgical site was lower than before surgery while it increased within the first three days after surgery. It is known that cooling down of tissue is associated with higher risk of infection and rather wound healing disorders. Due to local vasoconstriction and therefore increasing the affinity of Hb for oxygen there is a decrease in oxygen available for neutrophils that fight infection. Important factors like activity of neutrophils, fibroblasts and epithelial decreases when local temperature drops [23, 24, 25, 26].
Interestingly, patients in our study showed a decrease in hemoglobin levels within the first three days after surgery. Statistically significant negative correlations between ST and Hb-level were found on the first, second and fourth postoperative days (
Furthermore, we have demonstrated, that FLIR can visualize ischemic area in surgical site. Comparing to vital tissue, there was a decrease of 0.8∘C in ischemic tissue area. Unfortunately, in our study we have only detected one case of wound healing disorder which lay not claim to representativity (segmental decompression of stenosis L4/5).
Moreover, we investigated inflammatory laboratory markers after surgery. Values are varying due to diverse indications for surgery. The results showed increasing blood levels of CRP and leukocytes within the first three days after surgery in all patients. CRP level reached a maximum on day three after surgery (mean 105.1 mg/l
Regular CRP response after uncomplicated elective surgery is well studied. It is known that CRP level increases after surgery as an effect of tissue damage [27, 28, 29]. It is valid that there should not be a continuous elevation or a second rise within the first weeks after surgery [30]. Nevertheless, CRP is meant to be a non-specific value and is therefore only of limited significance. This must be considered particular in context of clinical wound assessment. As also shown in our study, clinical wound assessment supported by FLIR was more important than measurement of laboratory parameters.
Several limitations of the study must be mentioned. First, the heterogenic patient collective with different surgical interventions, second the small sample size which cannot represent a connection between thermographic measurement by FLIR and wound healing disorders. Third, we only observed the inpatient stay, thus immediately after surgery. We did not collect any information after patient’s discharge and therefore cannot make an assessment on laboratory and wound healing course in ambulatory setting. Probably few SSIs and wound healing disorders were diagnosed after discharge and thus not detected in our study.
Despite these limitations, the present study provides promising results for the use of thermography in the early detection of wound healing disorders.
Conclusions
This study demonstrated that clinical wound assessment must remain top priority in early detection of SSI as well as wound healing disorders after posterior lumbar spine surgery. Nevertheless, measurement of laboratory parameters is also crucial due to several other complications. FLIR is an easy-to-handle low-cost method which can be used as complimentary tool in clinical wound assessment. Due to non-contact measurement of local ST, there seems to be no risk to patient-safety.
Author contributions
All authors have participated in the study, helped in the preparation of the manuscript, and approved this submission.
Funding
The authors report no funding.
Ethical approval
All procedures performed in our study involving patients were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Institutional ethics committee approval was given prior to this study.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.