
Abstract
BACKGROUND:
Physical inactivity is prevalent among hospitalized patients and the daytime spent lying should be utilised for exercise. However, implementing new interventions in hospitals’ complex daily routines is difficult and requires a participatory approach.
OBJECTIVE:
Exploring clinical settings and clinicians’ perspectives regarding exercise in hospitalized patients to gauge the potential of further development of an in-bed training device and to formulate development goals.
METHODS:
A User-Centered Design approach was employed, consisting of work shadowing and focus groups with physiotherapists and nurses. Content and network analyses of the focus group data were performed. Personas were then developed and used to create clinical scenarios.
RESULTS:
Some clinicians perceived in-bed exercise counterproductive, while others recognized potential for unsupervised training. The most important design characteristics appeared to be a small size, low weight and simplicity of use to facilitate storage, transportation, and administration, respectively. The scenarios revealed that the device’s use could increase the physical activity time by 1.4%, although it would also increase the working time of clinicians.
CONCLUSION:
The study highlighted the difficulties in developing a usable training device but encouraged the authors to pursue their efforts under the strict condition of following the formulated development goals.
Introduction
Decreased physical activity levels are frequently found among patients in hospital and rehabilitation settings [1], leading to functional decline and further diseases [2]. The clearest example of deconditioning is found in critically ill patients from the Intensive-Care Unit (ICU) who may develop ‘ICU-Acquired Weakness’ [3]. However, physical inactivity is a phenomenon that also concerns many other patient groups [2], particularly in elderly. Functional decline can be observed on multiple systems of the human body, including physical and cognitive [4, 5]. For example, it has been shown that bed rest during hospitalization can lead to significant loss of strength in the lower extremities [6], representing an important risk factor for falls in elderly [7]. Other studies have shown that even mental health is affected by physical inactivity in hospital [8]. Altogether, the consequences are that after discharge, patients not only have to recover from their condition that caused hospitalization and/or rehabilitation, but also from the hospital-acquired deconditioning (HAD). It is therefore not surprising that HAD represents a major risk factor for readmission to hospital after discharge (e.g. [9, 10]).
Given this serious issue of HAD, it is important to improve the level of physical activity in hospitalised patients. However, implementing interventions for this purpose is a complex task [11] and it is important to provide as many innovative options as possible to facilitate it. For example, to counteract ICU-Acquired Weakness, an in-bed leg press-typed training device has recently been developed [12]. The device consisted of a base containing two cylinders to which two pedals were connected. It could be placed in patients’ bed allowing them to push the pedals against adjustable resistance. The device presented high levels of usability [12] based on indicators, such as the system usability scale [13] or the Kano model [14].
Nevertheless, ICU patients represent a very limited proportion of patients, which limits the impact of the device. Hence, it appeared interesting to pursue the idea of adapting this leg press to suit other patient groups. The starting point was the notion that the current version of the leg press would likely under-challenge many patients outside the ICU. To increase the challenge, it was assumed that adding more functions to the device was necessary. For example, adding multiple degrees of freedom (DOF) to allow diverse movement patterns and utilizing the potential of exergame-technologies appeared to be sensible ideas.
But since there is a need to shift towards User-Centered Design’ (UCD) processes in the development of healthcare devices [15, 16], our development ideas were only considered one way of looking at the problem and had to be opposed to clinical practice routines and end-users’ perspectives to ensure optimal usability. Consequently, this study placed its focus on potential end-users and aimed to objectify their clinical settings and to understand their views regarding exercise in hospitalized patients. The finale objectives were to gauge the potential of such a device outside the ICU and to formulate first evidence-based development goals.
Methods
General methodology
This study represented the first iteration of a UCD process. To achieve the study’s aim, multiple data sources were required, allowing triangulation of objective and subjective data. This method affords more robust conclusions [17].
First, work shadowing sessions were carried out to objectify clinical settings and to observe clinical practices. Then, based on these results, a list of relevant topics for discussion was generated for focus groups. Focus groups were performed, and a network analysis of the data was conducted to identify impactful development domains. The focus group data were also used to define user profiles (personas). Based on these intermediate results, the initially conceived design of the device was revised and clinical scenarios involving the personas were developed. All data were used to formulate development goals. Figure 1 illustrates the overall procedure.
Overall study procedure. The black rectangles (‘Work Shadowing’ & ‘Focus Groups’) represent data collection phases, whereas the ellipses represent how the data was utilized and/or analyzed. The lowest rectangle (‘Development Goals’) represents the aim of the study.
The study did not fall under the Swiss Human Research Act because it neither investigated human pathology or physiology, nor involved collection of health-related data [18]. Hence, no ethical clearance was required. Ethical principles based on the Declaration of Helsinki [19] were respected, nonetheless. All participating clinicians were informed about the goals of the study, their tasks, the voluntary nature of their participation (including their right to withdraw at any time), and the anonymization of the data. Informed consent was obtained from all participating clinicians.
Work shadowing
We used the ‘fly on the wall’ method [17], where the first author passively observed physiotherapists during their daily work routine. All clinicians were recruited among the six sites of Switzerland’s largest hospital group (Insel Gruppe), including Bern University Hospital. Field-notes were taken on a custom form and photographs were shot to substantiate the notes. The objective was to perform i) worker (i.e. working preferences), ii) environmental, and iii) task analyses. The data were summarized in a table and formed the basis for the development of an interview guide for the focus groups.
The six themes are depicted as the first column of ellipses on the left. Each theme is composed of thematically similar sub-themes (second column of ellipses). Sub-themes are composed of ‘positions’ (rectangles), which are statements summarizing raw opinion data.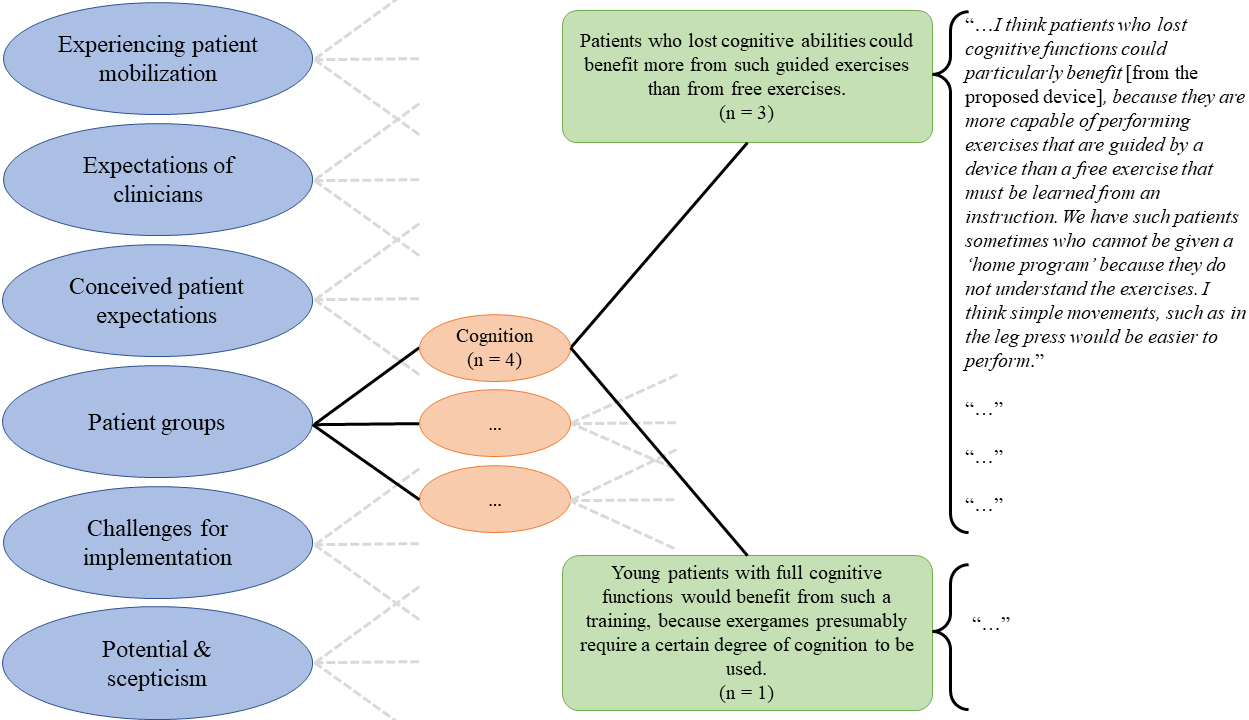
An interview guide was drafted by the first author, reviewed by two experienced qualitative researchers, and tested with an expert in musculoskeletal physiotherapy. The final version of the guide covered the five following key questions to structure the focus groups:
How do you experience patient mobilization and exercise in patients? What would be your expectations regarding a device for unsupervised exercise in patients, in order to integrate it into your daily practice? What do you think are patients’ expectations regarding such a device? What patient groups could benefit from that device? What challenges do you see in using such a device in your daily practice?
Target population for the focus groups consisted of physiotherapists and nurses. Personnel from ICU were excluded because this was the topic of the first leg press [12]. Personnel from orthopaedic departments were also excluded because it was thought that patients recovering from orthopaedic surgery would frequently have non-weightbearing rehabilitation regime, making exercise with a leg press difficult. Inclusion criteria were i) having a minimum of 1 year of clinical experience at full-time equivalent, and ii) working at least two hours per day with in-patients. These criteria allowed a selection of participants who have a clear understanding of the work with the patients, of the daily clinical routines, and of the problems that may occur. Participants’ recruitment was based on voluntary response sampling [20], where flyers were distributed in four sites of the Insel Gruppe. In addition, key persons consisting of head physiotherapists and advanced practice nurses from these sites and other hospitals were contacted for a network sampling strategy [20].
Online focus groups were conducted and recorded using Microsoft Teams. First, demographic data and information on work experience were collected, a short presentation of the first leg press version [12] was provided, and then, the discussion was launched.
After the focus groups, intelligent verbatim transcription of the records was performed using the software f4analyse (v. 3.0.0) and finalized transcripts were sent to interviewees for review as quality check [21]. A content analysis was then performed according to Kuckartz and Rädiker [22] with a combination of a concept- and data-driven coding system. Five concept-driven themes were first generated based on the interview questions. Transcript content was coded into these themes and grouped into subthemes based on their topic in a data-driven process. The contents forming these subthemes are called ‘positions’ in this study (Fig. 2). Also, additional data-driven themes were generated where necessary. The software MaxQDA (v. MaxQDA Plus 2022, release 22.1.1) was used for this step.
Further data processing and utilization
Network analysis
A network analysis of the data from the focus groups was performed [23], in which subthemes represented the nodes. Edges were defined as cases where positions within subthemes had direct practical implications for other positions in other subthemes. Weights were also attributed to the nodes and edges. Node weights were calculated as the sum of all positions they contained and edge weights by the number of times connected positions were mentioned. The analysis regarded all nodes that related to the design of the device (‘design-related’) as independent variables because the design is typically invariable once the device is implemented. Edge weights from these design-related nodes were examined and ranked to indicate what the design would impact most.
Review of the initial design
The results of the network analysis were then used to discuss and reflect on the initially conceived design of the proposed device within the research team. Adaptations to that design were made based on consensus achieved during these discussions. Characteristics of a first hypothetical prototype were sketched.
Personas and scenarios
Using the focus groups data, personas were generated according to the method described in Cooper [24]. The target population for the proposed device was identified from these profiles. Using the target population personas in combination with the observational data from the work shadowing sessions, two user-scenarios were developed to conceptually test the feasibility of using the proposed device (Supplementary material 1). Both scenarios illustrated the hospital stay of a patient, once without (a) and once with the use of the proposed device (b). The scenarios were drafted by the first author with the focus on the description of a patient case that is frequently encountered in a public hospital, and on the patient’s activities during hospital stay. Clinicians from the authors’ institution and from the Insel Gruppe who did not participate in the work shadowing sessions and focus groups were recruited to review the scenarios. They were asked to rate the scenarios regarding their credibility using a scale ranging from 0 (‘The scenario is not credible. It does not reflect a plausible patient case and hospital stay’) to 10 (‘The scenario is credible. It does reflect a plausible patient case and hospital stay’). In addition, they were allowed to comment the scenarios where required. The scenarios were adapted according to the comments. In a final step, the time during which the fictive patient conceivably performed different activities, as well as their intensity was estimated. The intensity of the activities was classified as ‘lying’, ‘sitting’, or ‘moving’ (e.g. walking) [25]. Using the proposed device was classified as a ‘moving’ activity. The estimated activity-times were calculated as a percentage of the total daytime spent in hospital. Daytime was preferred as a reference over the entire hospitalization time, because the importance of sufficient quality sleep at night was acknowledged for optimal convalescence (e.g. [26]). The staff’s working time spent helping the patient in ‘sitting’ and ‘moving’ activities was also counted. The two scenarios were compared using these time-related results.
Formulation of development goals
Based on raw (work shadowing and focus groups) and processed data (network analysis, personas, and scenarios), development goals were formulated, discussed, and finalized.
Results
Work shadowing
Three institutions accepted to participate. Two were hospitals for acute care with integrated rehabilitation centers (geriatric, cardiac, and pulmonary) and one was a rehabilitation center for neurological patients. In one institution, two different physiotherapists were observed, making a total of four participating clinicians. A total of 13 patients were viewed by the four clinicians during the work shadowing periods.
Worker analysis
All participants chose to provide active therapy sessions over passive therapy, except for one session in which the patient complained about pain. Nearly all sessions consisted of practising an activity of daily living (ADL), such as walking, or getting up from bed or from the ground. Only one contained the use of an exercise device (digital balance training device). All patients also received instructions to exercise by themselves as adjunct therapy, but these exercises included no or minimal equipment, such as elastic bands.
Environmental analysis
All beds had the same dimensions (2 m long, 0.95 m wide), and the space beside the bed was consistently relatively narrow, ranging from 0.85 to 2 m. The space at the foot of the bed was even narrower, ranging from 0.75 to 1.8 m. Also, when disregarding regular furniture, up to seven additional large objects, such as wheelchairs, walking frames, or monitoring system, were counted in patient rooms (range: 1–7). The dimensions of the lift ranged from 2 to 2.7 m in depth, and 0.7 to 1.8 m in width. In two institutions, the storage room, in which therapeutic devices are stored, was located in the basement, making unplanned use of a device difficult. Only one institution had an auxiliary storage room level to patients’ rooms. In both hospitals, all therapy sessions started and ended in patients’ rooms, whereas in the rehabilitation center the meeting point was either an exercise room or the patient’s room.
Task analysis
Main diagnoses were most often of cardiac, pulmonary, or neurologic nature and the majority of patients were co-morbid. Some patients also were hospitalized for deterioration of their general condition. Overall, 47% of the patients were autonomous, while the other 53% needed help to walk and/or get out of bed.
On average, 22 minutes (range: 16–32 min.) of contact time between therapists and patients were measured per patient. However, therapists had to add time for documentation.
Focus groups
In total, 10 clinicians (7 physiotherapists and 3 nurses) participated in three focus groups, which lasted, on average, 41 minutes (range: 32–47). Participants had an average working experience of 11 years (range: 1–27 years), with 7 years (range: 1–25) in their current settings. Five participants worked in a hospital, and five in a rehabilitation center. Six participants worked in several departments, where internal medicine was represented most frequently (5 participants), followed by the geriatric, neurologic, pneumological departments (each 2 participants), and oncologic rehabilitation (1 participant). Out of the 10 participants, seven reviewed the transcripts and returned their feedback. Thematically, nothing had to be added, removed, or changed.
Representation of the network analysis. The six themes (described in the legend) contain the subthemes, which are represented by circles. The size of the circles is proportional to the node weight. The connecting lines represent the edges. The thicker and lighter Gray they are, the larger the edge weight is.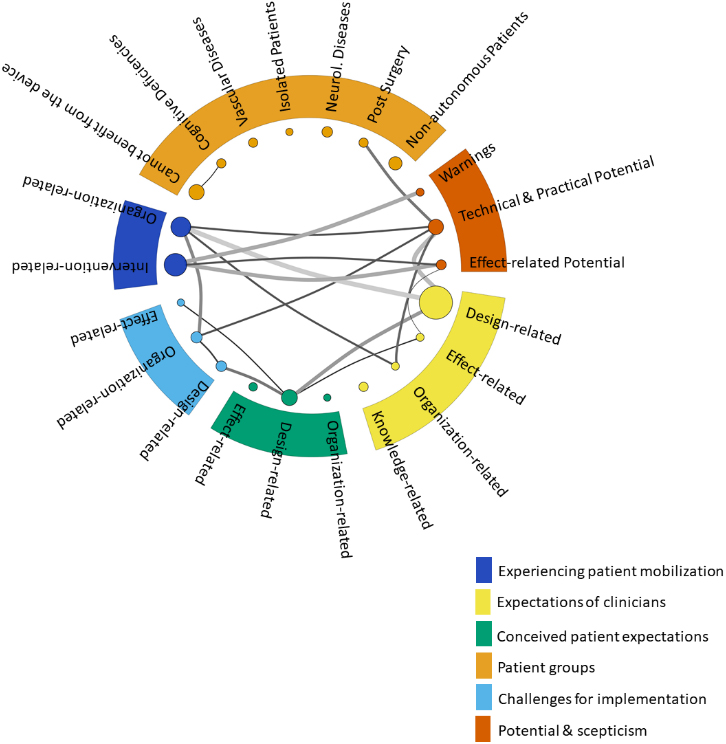
Six themes were generated (Fig. 3). The themes ‘Experiencing patient mobilization’, ‘Expectations of clinicians’, ‘Conceived patient expectations’, ‘Patient groups’, and ‘Challenges for implementation’ were concept-driven, whereas the theme ‘Potential and scepticism’ was data-driven.
All clinicians agreed that mobilizing patients into an upright posture as early as possible is the most important goal in hospitalized patients (subtheme ‘Therapy-related’,
Expectations of clinicians
Much of the expectations were ‘design-related’ (
Patient safety was also mentioned. The aspect of technology was a dividing issue, with some participants proposing the use of visualization effects (e.g. biofeedback) and exergaming, while others thought using such technology would rather be a barrier because it would increase complexity of use. Some participants were also concerned about the repercussion a sophisticated device could have on the price. For example, frames used to help mobilizing weak patients into a sitting or standing position are cheap, and if the leg press is comparatively expensive, it would make more sense to invest in several of those mobilization frames to achieve the goal of getting out of bed as soon as possible.
Two participants stated that using the device should show clear strengthening effect (‘Effect-related’). Also, they stated that the device should have a motivating effect because patients often have low functional levels and therefore low self-efficacy, self-esteem, and motivation levels. Participants also wished strong evidence showing the benefit of such a device before using it in their clinical practice (‘Knowledge-related’,
Conceived patient expectations
Most conceived expectations were also related to the device’s design (‘Design-related’,
Here, the level of technology use and technical complexity divided opinions, too. One participant intentionally formulated an exaggerated description:
“…patients aged 80 or older are all adverse [to new technologies], while all patients below 70 years of age are fascinated by all technological gadgets …”.
Patients would also value comfortable design. Finally, participants thought that patients wish clear benefits from using the device in achieving their therapeutic goals (‘Effect-related’,
Patient groups
‘Non-autonomous patients’ were considered the patient group that could benefit the most (
Challenges for implementation
Most challenges in using a device like the proposed leg press in daily practice were seen to be ‘organization-related’ (
Second-most mentioned positions were ‘Design-related’ (
Finally, seeing no positive effects from using the device could be perceived as a challenge (‘Effect-related’,
Potential and scepticism
The focus groups showed that the interview guide did not cover all relevant topics as some discussions drifted away from the key questions to reveal other important aspects. These contents were coded as theme ‘Potential and scepticism’. They expressed explicit scepticism towards the device or, in contrary, ideas for potential use or further development. Here, ‘scepticism’ differs from the theme ‘Challenges’ in that it addresses negative opinions on the idea of implementing the device while challenges referred to practical aspects if the device was implemented.
First, some participants realized ‘Technical and Practical Potential’ (
In contrary, some other participants expressed their strong scepticism and warned against ‘tying patients to bed’ with the device. Moreover, they feared that implementing the leg press could tempt physiotherapists to replace therapy with simply administering the device which would contradict their work ethic.
Network analysis
Figure 3 illustrates all themes (legends) and subthemes (nodes) with their connections (edges). The edges connecting ‘design-related’ nodes, their weight and interpretation are presented in Table 1.
Interpretation of the edges found in the network analysis
Interpretation of the edges found in the network analysis
From the content analysis, three archetypes were identified, which are presented in Table 2.
Description of the personas, including demographic data and opinions on using a training device in regular clinical practice
Description of the personas, including demographic data and opinions on using a training device in regular clinical practice
Comparison of both clinical scenarios. Top row: credibility evaluation by five clinicians. Middle row: Scenario analysis from a patient’s perspective. Bottom row: Scenario analysis from a clinician’s perspective
To review the scenarios, one clinician (nurse) from the authors’ institution and four from the Insel Gruppe (two nurses, two physiotherapists) could be recruited. Both scenarios were considered to be credible (Table 3). Some clinicians provided comments, which were used to adapt the scenarios. The comparison of the two scenarios is presented in Table 3. In both scenarios, the patient was thought to be awake between 7 am and 8 pm. Together with the first (4.5 hours) and last day (3.5 hours), the patient spent a total of 60 hours awake (i.e. daytime). Employing the proposed device led to a shift in daytime use from ‘lying’ towards ‘moving’ activities of 1.4% (approximately 50 minutes). With an installation and removal time of 10 minutes each, employing the proposed device increased the working time dedicated to the patient by 50 minutes for the nursing staff and by 15 minutes for the physiotherapist. Detailed results are presented in Supplementary material 2.
Development goals
Based on the results, the research team agreed on targeting a design that is close to the original leg press because of its simplicity and user-friendliness. The targeted time to install and time to remove the device from the patient’s bed was set to 10 minutes. Additional functionalities were kept to a minimum, including an additional DOF to allow plantar- and dorsiflexion in the ankle joint, the possibility to feature simple exergames and provide bio- and motivational feedback. Versatile use, i.e. in a lying and sitting position, as well as the possibility to keep the device attached to the bed when not in use, were also set as development goals.
A video of a prototype developed based on these development goals with a demonstration of some of its features can be found here:
Discussion and conclusion
This study investigated clinical settings and potential end-users’ perspectives regarding exercise in hospitalized patients to define a first evidence-based development framework for subsequent UCD iterations.
In general, all participants recognize the importance of physical activity in patients to achieve targeted clinical outcomes and to prevent deconditioning. They all strive to mobilize patients out of bed and practice ADLs, as became clear from the interviews and from work shadowing. However, they also recognize that mobilizing non-autonomous patients is not always possible due to understaffing and/or complexity of patient cases. For this reason, some participants (personified as ‘Maria’) find that a device, such as the leg press, could form a good alternative for unsupervised exercise. In contrast, others (personified as ‘David’) are strongly opposed to exercising in bed if not absolutely necessary. Despite clear evidence that prolonged lying can have devastating effects on patients [27, 28], it must be considered that hospitalized patients lie in bed for an average of 70–83% of their time, even those with walking abilities [29, 30], and some of this time should be used to exercise. However, patients are often left alone [1], which makes exercising difficult, particularly in the group of non-autonomous patients (53% according to our observations). Hence, the research team believes that unsupervised exercising in a secure position, such as lying, is important.
For successful implementation, the device must be lightweight and compact to allow easy transport and handling, quick installation as well as possible storage in patients’ rooms. These aspects are considered most important due to their large impact on organizational aspects (edge weight
To further improve usability of the leg press and facilitate its implementation, it appears important to make the device more versatile (e.g. use in sitting position) and to feature motivational signals, ways to monitor progression (edge weight
In conclusion, the results showed that in-patient settings are characterized by hectic daily routines, in which some additional work time can already represent significant barriers to the use of a therapeutic method. However, if following the formulated development goals and if targeting the right patient and end-user groups, the proposed in-bed leg press may have potential in clinical practice.
Strengths and limitations
First, the main strength of the study is that several data sources building on one another were utilized to collect data. Moreover, the data were processed in different ways, allowing the exploration of diverse aspects. Second, while the study focussed on the development of a particular device, the questions used to frame the focus group discussions were formulated in such a way that the current results can be used for the development of any exercising device for most in-patient settings. It should be noted that highly specialized settings, such as neurological rehabilitation settings might have different requirements, however. The main limitation is that the samples were relatively small (4 for work shadowing, 10 for focus groups).
Funding
The authors report no funding.
Supplementary data
The supplementary files are available to download from https://dx-doi-org.web.bisu.edu.cn/10.3233/THC-240816.
Footnotes
Acknowledgments
The authors thank all participants and their institutions for their participation.
Conflict of interest
The authors declare that they have no conflict of interest.