
Abstract
BACKGROUND:
Diabetes, which is associated with cardiovascular disease and related microvascular complications, affects life expectancy and decrease quality of life. A trial reports that the risk of patients with diabetes having cardiovascular disease is 2–4 times compared with that in patients without diabetes.
OBJECTIVE:
This study aims to investigate the relationship between depth of general anesthesia in patients with diabetes mellitus
METHODS:
This clinical study totally includes 40 patients with diabetes mellitus, and these patients are divided into following two groups: diabetes mellitus deep anesthesia group and diabetes mellitus light anesthesia group, and then these patients receive general anesthesia combined with laparoscopic surgery. Preoperative patient general data and intraoperative patient general data are collected and analyzed. Calcitonin gene-related peptide (CGRP) and substance P (SP) level are determined by Enzyme-linked immunosorbent assay (ELISA)
RESULTS:
This study included a total of 40 patients. There were no significant differences in demographic and preoperative patient general data between the two groups. Measurements were taken for operative time, anesthesia time, recovery time after drug withdrawal, dwell time in the recovery room, intraoperative fluid volume, intraoperative blood loss, and intraoperative urine output between the two groups. Significant differences were observed in the recovery time after drug withdrawal between the two groups. CGRP and SP level in diabetes mellitus deep anesthesia group are evidently more than those in diabetes mellitus light anesthesia group.
CONCLUSIONS:
CGRP and SP level are involved in the diabetes mellitus and up-regulated CGRP and SP can prevent the development of diabetes mellitus. Our study extends the existing literature by addressing a gap in knowledge regarding the impact of anesthesia depth on neuropeptide levels in diabetes mellitus patients. By delineating this relationship, we aim to contribute to the advancement of perioperative care practices and ultimately improve outcomes for individuals with diabetes undergoing surgical procedures. Our study’s findings provide valuable insights into the complex interactions between anesthesia, neuropeptides, and diabetes mellitus, offering the potential for personalized perioperative care, enhanced pain management, and improved surgical outcomes. These implications highlight the clinical relevance of our research and its potential to inform future advancements in perioperative care for diabetic patients undergoing surgery.
Introduction
Diabetes, which is associated with cardiovascular disease and related microvascular complications, affects life expectancy and decrease quality of life [1]. A trial reports that the risk of patients with diabetes having cardiovascular disease is 2–4 times compared with that in patients without diabetes [2]. In addition, patients with diabetic neuropathy have risk of involving general sensation, movement and autonomic nerves. Especially autonomic nerves, and autonomic nerves involved by diabetes can weaken the protective compensatory capacity of the heart [3]. Patients with involvement of the autonomic nerves are characterized by reduced heart rate variability, orthostatic hypotension, asymptomatic myocardial ischemia, or painless myocardial infarction [4]. Currently, numerous methods of treatment for diabetes such as drug therapy, surgical treatment has been used to decrease the damage of diabetes, lower blood glucose, lower blood pressure, regulate blood lipids, antiplatelet aggregation, control body weight, improve lifestyle, decrease related complications [5]. However, some studies report that patients with diabetes treated in general anesthesia are prone to cardiovascular adverse events during surgery compared to that in patients with non-diabetes during surgery, but responding studies are still limit [4]. It is urgent to conduct related trials to investigate the effect of general anesthesia in patients with diabetes.
Given the importance of effective surgical interventions for patients with diabetes, Laparoscopic surgery, which relies on 2 K high-definition 2 K image quality, has been widely used to treat the patients with diabetes and plays an important in decreasing the damage caused by diabetes and its related complications [6, 7]. To improve the treatment effect and reduce the pain of patients. General anesthesia combined with laparoscopic surgery is utilized to treat diabetes and related complications. However, some trials show that depth of general anesthesia in patients with diabetes is associated with incidence of cardiovascular adverse events during operation [8, 9]. Calcitonin gene-related peptide (CGRP), which has been implicated in the pathogenesis of cardiovascular adverse events, may participate in the development progress of diabetes by regulating downstream responding target and pathway [10]. Nevertheless, related studies concerning SP in patients with diabetes are still insufficient.
Recognizing the gaps in existing research, further investigation into the relationship between SP and diabetes is crucial for understanding potential implications for patient care. Previous studies have suggested that levels of CGRP and SP are associated with diabetes, and down-regulating CGRP and SP levels may increase the incidence of cardiovascular adverse events in patients with diabetes [11, 12]. Some studies show that depth of general anesthesia in patients with diabetes probably lead to risk of cardiovascular adverse events by decreasing the CGRP level and SP level, but these results still lack sufficient evidence. Therefore, a clinical study about the role of depth of general anesthesia in serum CGRP and SP level in diabetes patients is conducted to clarify the relationship between depth of general anesthesia in diabetes patients and CGRP level, SP level.
Methods
Study design and participants
A total of 40 patients with diabetes from our hospital during January 2021 to January 2023 are enrolled in this retrospective observation study, and all patients are divided into following two groups: diabetes mellitus deep anesthesia (DMDA: blood samples after operation are collected) group and diabetes mellitus light anesthesia (DMLA: blood samples are collected in 30 minutes before induction) group. All patient used for this retrospective observation study are treated using different depth of general anesthesia combined with laparoscopic surgery. The hospital ethics committee have approved all protocol used for this study and written informed consent forms are obtained from all patients with diabetes.
Inclusion criteria for all patients are as follows: The patient has symptoms such as thirst, excessive drinking, urination, overeating but weight loss and meet the following requirements at the same time: patients have a
Exclusion criteria for all patients are as follows: patients used for our study suffer from neurological and psychiatric diseases; patients have taken sedative, analgesic, antidepressant, immunomodulatory and other drugs for a long time; patients have severe dysfunction of important organs; Patients have history of general anesthesia combined with laparoscopic surgery; The patient or patients’ guardians do not sign the written informed consent.
Trial design
All patients were routinely forbidden to eat and drink before being transferred to operating room. After entering the room, venous access was established and lactate Ringer’s solution was infused, and then the monitor was connected to monitor the patient’s heart rate, blood pressure, blood oxygen saturation, electrocardiogram, BIS value, and low flow oxygen inhalation was performed. Total intravenous anesthesia was used during the operation, and anesthesia induction was performed by sequential intravenous injection of sufentanil 0.5
Baseline data detection
To evaluate the baseline data between two groups. The age, BMI, blood lipid, blood glucose, HbAlc and diabetes course of patients in each group were recorded. In addition, the anesthesia time, operation time, eye opening time after drug withdrawal, recovery room stay time of patients in each group were Recorded.
Determination of CGRP and SP concentration in serum between two group by enzyme-linked immunosorbent assay (ELISA)
A total of 5 ml of blood sample from the elbow vein of the non-infusion side in each patient at two time points of 30 minutes before induction and after operation were collected, and then placed blood sample in the vacuum separation gel accelerating tube. The blood samples in two groups of patients were immediately separated by centrifugation at 3000 rpm at 4∘C for 10 min and then the serum is extracted. The serum was sub-packed in EP tubes and labeled, and stored in a refrigerator at
Statistical analysis
SPSS 20.0 statistical software was used for statistical analysis. The descriptive data were presented by
Results
Preoperative patient general data
Preoperative patient general data is shown in Table 1. The gender, age, body mass index (BMI), High-density lipoprotein (HDL), low-density lipoprotein (LDL), triglyceride (TG), preoperative blood glucose (PBG), duration of diabetes (DOD), Hb A1c from diabetes mellitus deep anesthesia (DMDA) group and diabetes mellitus light anesthesia (DMLA) group are recorded. These results indicated that there was no significant difference in the preoperative general data between the DMDA group and the DMLA group.
Demographic, preoperative patient general data
Demographic, preoperative patient general data
Note: A Chi-square test was performed for evaluation of descriptive data and measurement data was compared using
Preoperative patient general data is shown in Table 2. The operative time, the anesthesia time, the recovery time after drug withdrawal, dwell time in recovery room, intraoperative fluid volume, intraoperative blood loss, urine output from diabetes mellitus deep anesthesia group and diabetes mellitus light anesthesia group are recorded. The results indicated that there is no significant difference in the intraoperative general patient data between the DMDA group and the DMLA group.
Intraoperative patient general data
Intraoperative patient general data
Note: A Chi-square test was performed for evaluation of descriptive data and measurement data was compared using
CGRP and SP level are determined by ELISA and presented in Fig. 1. CGRP concentration in DMLA group (blood samples in preoperative 30 min) is 47.8
The levels of CGRP and SP. The CGRP levels in preoperative 30 min blood samples and postoperative blood samples are determined by ELISA, and these results are presented in Fig. 1A. The SP level in preoperative 30 min blood samples and postoperative blood samples are determined by ELISA, and these results are presented in Fig. 1B. The value is presented as means 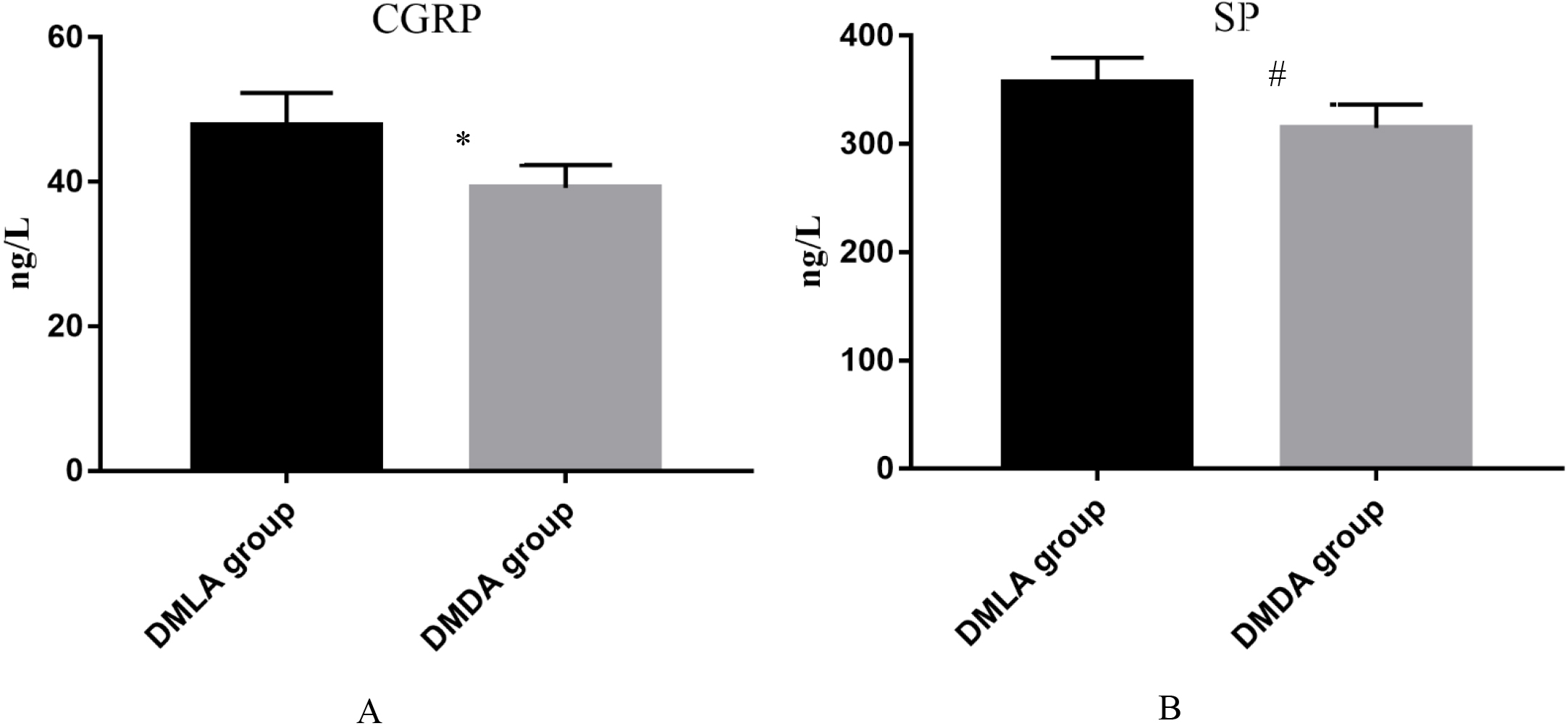
Patients with diabetes mellitus are at a high risk of cardiovascular disease because of operation and general anesthesia. To investigate the effect of depth of general anesthesia in patients with diabetes mellitus, we conduct this study to detect the preoperative patient general data, intraoperative patient general data, serum CGRP and SP level in diabetes patients induced by different depth of general anesthesia. To address these potential confounders, we employed several strategies in our study. Firstly, we collected comprehensive demographic and clinical data from the participants, including age, gender, and comorbidities, which were incorporated into our statistical models as covariates. By adjusting for these variables in our analysis, we aimed to control their potential influence on the outcomes of interest. Additionally, we conducted sensitivity analyses to assess the impact of these confounding variables on our results. This involved re-analyzing the data after excluding or stratifying by certain confounders to evaluate their effect on the associations observed in our study. By conducting these sensitivity analyses, we were able to assess the robustness of our findings and ensure that they were not unduly influenced by confounding variables. Our results show that preoperative patient general data between two groups of patients with diabetes mellitus are no significantly statistical difference. Compared to intraoperative patient general data in DMLA group, recovery time after drug in DMDA group is clearly increased, and other intraoperative patient general data between two groups of patients with diabetes mellitus are no significantly statistical difference. In addition, serum CGRP and SP level in diabetes patients are identified using ELISA. Compared to CGRP level in DMLA group, CGRP level in DMDA group is markedly decreased. The SP level in the DMDA group is significantly lower than that in the DMLA group. These findings indicate that the depth of general anesthesia in diabetic patients is linked to cardiovascular diseases by regulating the concentration of CGRP and SP level in diabetes patients.
A preliminary clinical study on effect of CGRP level in patients with diabetes suggests that CGRP level in blood serum in patients with diabetes is significantly down-regulated, but the effect of depth of general anesthesia in CGRP level in blood serum in patients with diabetes is still unclear [13]. Substance P (SP), which is a nociceptive tachykinin, may be associated with development progress of diabetes by regulating the immune inflammatory reactions [14]. A randomized controlled trial by Gong X shows that SP is involved in patients with type 2 diabetic by sympathetic inflammatory responses, and down-regulated SP level in patients with diabetes can increase the risk of having cardiovascular adverse events [14]. Calcitonin gene-related peptide (CGRP), play an important in adults with migraine, but studies relating to CGRP in diabetes mellitus remain limit. A randomized controlled trial by Iyengar S [15] point out that CGRP inhibitor monoclonal antibodies is associated with overweight, obese and diabetes by controlling insulin secretion, this study shows that CGRP is implicated in the regulation of diabetes mellitus. However, the information provided by this study remain limit. To further clarify the relationship between CGRP and diabetes mellitus, a study by Yuan LJ [16] investigate the role of CGRP in women with Gestational diabetes mellitus, and these results in this randomized controlled study suggest that CGRP concentration in serum of with Gestational diabetes mellitus is negatively with that in health women, we can conclude that CGRP concentration is also participating into development progress of diabetes [17]. General anesthesia combined with laparoscopic surgery has been widely used to treat the patients with diabetes. The relationship between the depth of general anesthesia and our study investigates CGRP concentration, and the findings from this trial indicate a negative correlation between CGRP levels and the depth of general anesthesia in diabetic patients. These results have been documented in related research fields and suggest a potential method for the prevention and treatment of diabetes mellitus.
Substance P (SP), participates in development progress of multiple disease as a nociceptive tachykinin. Several studies have also been conducted to explore the relationship between sleep paralysis (SP) and diabetes mellitus, and a randomized controlled trial conducted by Gong [14, 18] has reported that substance P (SP) is implicated in diabetes mellitus through sympathetic inflammatory responses. However, the relationship between SP concentration and diabetes mellitus remains unclear. It is urgent to clarify the effect of SP level in patients with diabetes mellitus. Therefore, we also conduct a clinical study to compare the SP level between diabetes mellitus deep anesthesia and diabetes mellitus light anesthesia, and our results by ELISA show that the SP level in diabetes mellitus deep anesthesia is obviously increased compared with that in diabetes mellitus light anesthesia. We can conclude that SP level is also negatively with the depth of general anesthesia in patients with diabetes mellitus. a randomized controlled trial by Zhu R [19] investigates the relationship between the SP level and depth of anesthesia in patients with open liver cancer resection, and their outcomes show that SP level in deep anesthesia is evidently lower than that in deep anesthesia. Our results are consistent with that reported by Zhu R. The findings from this current trial offer valuable research data for the treatment of diabetes mellitus. Nevertheless, our study has certain limitations, with the small sample size being the primary constraint. Therefore, further research with a larger sample size is necessary.
Conclusion
We can conclude that general anesthesia can affect development progress of diabetes mellitus by regulating the CGRP and SP level. Our study observed significantly higher levels of CGRP and SP in the deep anesthesia group compared to the light anesthesia group among diabetes mellitus patients. This suggests a potential association between the depth of anesthesia and neuropeptide levels in this specific patient population. However, it is essential to contextualize these findings within the existing literature on anesthesia, diabetes mellitus, and neuropeptide modulation. Previous research has demonstrated that anesthesia can have a modulatory effect on neuropeptide levels, with varying responses depending on the type and depth of anesthesia administered. Studies have also highlighted the dysregulation of neuropeptides, including CGRP and SP, in diabetes mellitus and their implications for pain perception and vascular function.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by Shanghai Municipal Commission of Health and Family Planning (202240159).