
Abstract
BACKGROUND:
Tonsillectomy and/or adenoidectomy can treat children with obstructive sleep apnea/hypopnea syndrome (OSAHS).
OBJECTIVE:
This study investigated the effects of tonsillectomy and/or adenoidectomy on cognitive function and brain structure in children with OSAHS.
METHODS:
This study included 40 obstructive sleep apnea/hypopnea syndrome children and 40 healthy children. The cognitive function and brain structure changes of OSAHS children before and after surgery and 40 healthy children were evaluated by the Swanson, Nolan, and Pelham Rating Scale (SNAP-IV) and the Integrated Visual and Auditory Continuous Performance Test (IVA-CPT), as well as brain resting-state fMRI functional magnetic resonance imaging (rs-fMRI).
RESULTS:
Children with OSAHS showed higher Swanson, Nolan, and Pelham Rating Scale and lower Integrated Visual and Auditory Continuous Performance Test scores than healthy peers, indicating cognitive impairment. Post-surgery, there was a significant improvement in cognitive function, evidenced by decreased Swanson, Nolan, and Pelham Rating Scale and increased Integrated Visual and Auditory Continuous Performance Test scores. Compared to healthy children, OSAHS children displayed altered ReHo values in certain brain regions, such as decreased values in the right angular gyrus, right precuneus, left parahippocampal gyrus, and left middle frontal gyrus, but increased values in the right posterior cerebellum. After surgery, ReHo values increased in regions like the right precuneus, right temporal lobe, right posterior cingulate gyrus, and left limbic lobe, suggesting neurological changes associated with treatment.
CONCLUSIONS:
Children with obstructive sleep apnea/hypopnea syndrome had cognitive impairment and abnormal changes in multiple brain regions. Tonsillectomy and/or adenoidectomy could improve cognitive function and contribute to the reconstruction of brain function and structure in children with obstructive sleep apnea/hypopnea syndrome.
Introduction
Obstructive sleep apnea Hypopnea syndrome (OSAHS) is a sleep disorder caused by partial upper airway obstruction and/or intermittent complete obstruction [1]. It is estimated that 425 million people worldwide suffer from OSAHS, which is a global public health problem [2]. Its characteristic is accompanied by apnea and insufficient ventilation during sleep, which is a common chronic disease in children [3]. OSAHS is highly prevalent in children aged 2 to 6 years old, with a prevalence rate of approximately 1% to 5.7% [4]. In developing countries, the prevalence can reach 10.47%, and it has increased to 50% among obese children [5].
Children are in a critical period of growth and development, and OSAHS can cause intermittent hypoxia (IH), hypercapnia, and thoracic pressure fluctuations in children, as well as intermittent awakening of sleep debris, thus affecting the operation of the central nervous system, cardiovascular and metabolic systems, and reducing the quality of life of children [6, 7, 8]. Intermittent hypoxia refers to sustained hypoxia. Any alternating occurrence of hypoxia and normal oxygen can be called intermittent hypoxia. Sleep debris will disrupt the production of growth hormones during slow-wave sleep, reduce the concentration of insulin-like growth factor
Diagnosis and treatment of pediatric OSAHS face several challenges. First, children cannot express their symptoms as clearly as adults, so the diagnostic process can be more complicated. Second, traditional diagnostic methods such as polysomnography are limited in their use in children because they may not be adequate for young patients. In terms of treatment, children may have different tolerances to some treatments, which also adds to the challenges of treatment. The clinical importance of multimodal functional magnetic resonance imaging lies in its ability to provide more comprehensive, non-invasive information that helps to more accurately diagnose pediatric OSAHS.
At present, nasopharyngeal obstruction is the main cause of OSAHS in children, and the upper airway obstruction caused by abnormal adenoid and/or tonsils is the most common [13]. At present, the diagnostic criteria for OSAHS in children are still controversial. However, polysomnography (PSG) is still generally regarded as the gold standard, and theapnea-hypopnea index (AHI) is often used to determine [14, 15]. PSG monitors continuous breathing, arterial blood oxygen saturation, electroencephalogram, electrocardiogram, heart rate and other indicators at night to understand whether the snorer has apnea, the number of pauses, the duration of pauses, and the lowest arterial blood oxygen level when pauses occur-value and extent of impact on physical health.
AHI refers to the average number of no-breathing and hypopnea events per hour. According to the guidelines, tonsillectomy and/or adenoidectomy can be used as the first-line treatment for OSAHS in children [16]. At present, research has confirmed that OSAHS patients have varying degrees of cognitive impairment. However, there is still some controversy about which aspects of cognitive impairment and the extent of cognitive impairment. In general, affected children often develop noticeable snoring at night due to blockage caused by apnea that blocks airflow. Children may experience brief pauses in breathing during sleep caused by airway obstruction or hypoventilation. Due to breathing problems, children may wake frequently at night, disrupting their sleep patterns.
The purpose of this study was to explore the effects of tonsillectomy and/or adenoidectomy on cognitive function and brain structure in children with OSAHS.
Material and methods
Patients
Forty children with OSAHS who underwent tonsillectomy and/or adenoidectomy from December 2021 to October 2022 were included in this study. Forty healthy children served as controls. All OSAHS children underwent tonsillectomy and/or Adenoidectomy and completed the evaluation of the Swanson, Nolan, and Pelham Rating Scale (SNAP-IV) and the Integrated Visual and Auditory Continuous Performance Test (IVA-CPT) and the resting-state functional Magnetic Resonance Imaging (rs-fMRI) scanning before and 3 months after the operation (Fig. 1). The same evaluation criteria were applied to the control group.
fMRI images of a typical child case with obstructive sleep apnea/hypopnea syndrome (OSAHS) before and 3 months after the operation. The fMRI results revealed that the ReHo values in the right cerebellar hemisphere, putamen, bilateral precentral gyri, parahippocampal gyrus, superior temporal gyrus, postcentral gyrus, and supplementary motor area were elevated in children with OSAHS. These brain regions are associated with sensorimotor functions, suggesting compensatory brain function in OSAHS patients. However, the ReHo values in cognitive regions, such as the left inferior temporal gyrus, bilateral cerebellar hemispheres, prefrontal cortex, precuneus, and angular gyrus, were decreased, indicating cognitive impairment in children with OSAHS.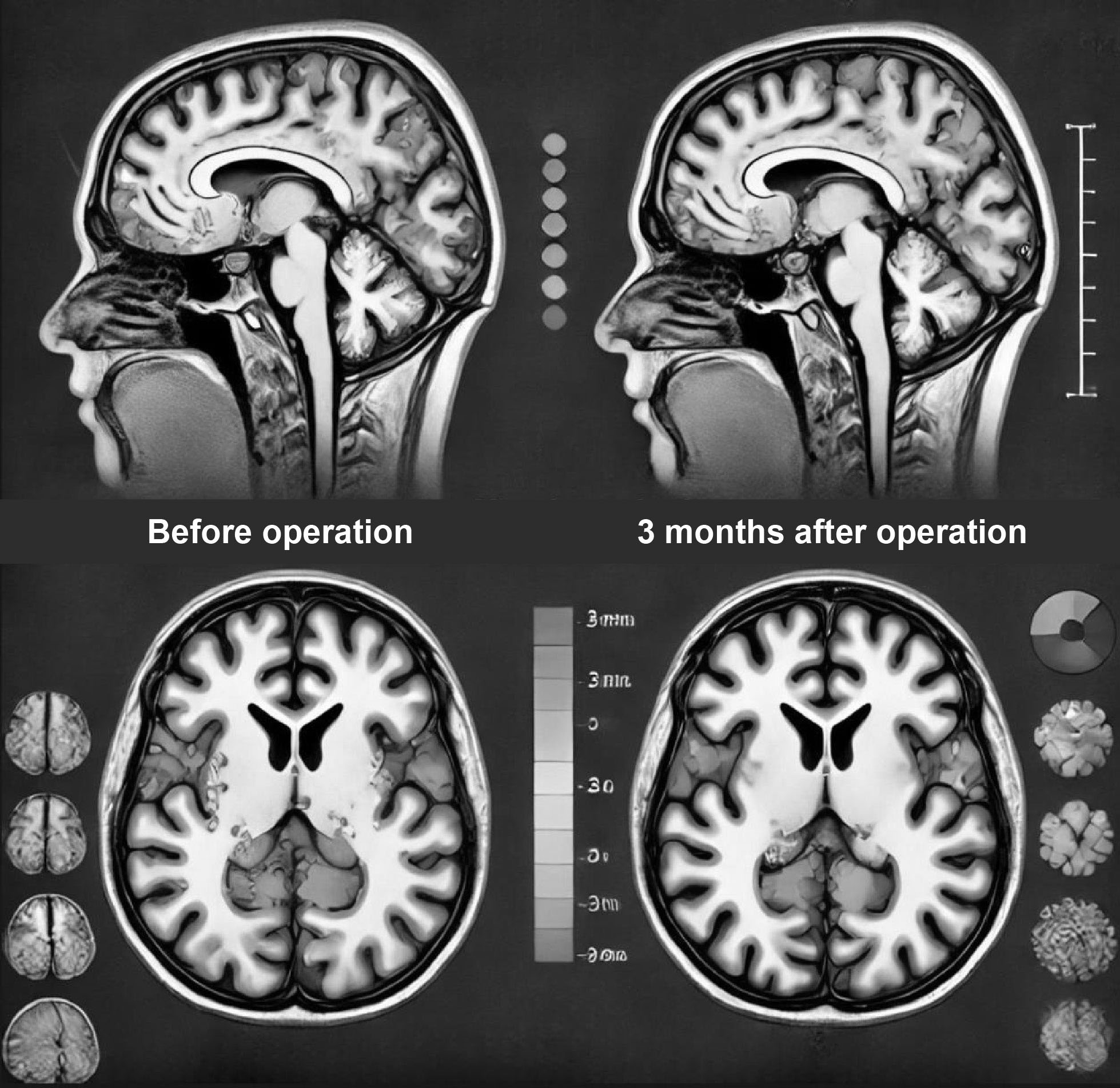
Inclusion criteria of children in OSAHS group: (1) those with clinical symptoms such as sleep snoring or mouth opening breathing; (2) those who were consistent with tonsil and/or Adenoid hypertrophy through clinical examination such as endoscopy or imaging; PSG diagnosed (3) OSAHS and tonsillectomy and/or Adenoidectomy was planned. Exclusion criteria of children in OSAHS group: (1) having a history of adenoid or tonsillectomy; (2) suffering from other diseases that may affect brain function; (3) OSAHS children whose families did not provide informed consent; (4) Those who have used sleep or sedative drugs; (5) the child has poor coordination (poor hand-eye coordination, insufficient balance, clumsy movements, unsteady gait, etc).
Inclusion criteria for healthy children: Children without OSAHS
Cognitive assessment
The neuropsychological assessment scale Wechsler Intelligence Scale, and the Montreal Cognitive Assessment Scale were commonly used in clinical practice, but they were not suitable for some young children included in this study. Therefore, the SNAP-IV scale and IVA-CPT evaluation system were used to evaluate children’s cognitive status.
The SNAP-IV scale consists of 18 items, each item having four grades, and the score is 0–3 points. The higher the score, the more obvious the cognitive impairment, and the poorer the cognitive level of attention and control.
IVA-CPT evaluated the full-scale response control quotient (FSCQ) and the full-scale attention quotient (FSAQ), with a mean of 100 points for each quotient. A score less than 85 was considered abnormal.
Collection of rs-fMRI data
Two groups of children were scanned using a magnetic resonance imaging system with unified scanning parameters: whole brain 3D T1 weighted imaging scan (TR/TE
Regional homogeneity (ReHo)
ReHo was used to process rs-fMRI data to reflect the functional state of the brain. By measuring the time dependence between adjacent voxels in brain regions, this method could evaluate the functional activities of brain neurons. With the increase of ReHo, the spontaneous electrical activity of neurons in the region gradually exhibited temporal synchronicity, and the electrical activity of neurons in this region had good consistency. On the contrary, it indicated poor activity consistency [18].
Data processing and ReHo calculation
The data were preprocessed using Matlab software for image data. The specific steps were as follows: (1) the first 10 time points of data were deleted to improve data stability, followed by correcting the remaining data time layers; (2) Correcting the head movement; (3) Spatial standardization: rs-fMRI images were registered to the specified standard MNI template; (4) A smooth kernel (6
Statistical analysis
Data are presented as mean
Results
General information
Among OSAHS children, there were 22 males and 18 females with an average age of (9.28
Baseline characteristics of the study participants
Baseline characteristics of the study participants
The SNAP-IV scores of children with OSAHS were compared with those of healthy children, as shown in Table 2. We observed that the SNAP-IV score was significantly higher in the OSAHS group (9.45
Comparison of the SNAP-IV scores of healthy and OSAHS children, as well as OSAHS children before and after treatment
Comparison of the SNAP-IV scores of healthy and OSAHS children, as well as OSAHS children before and after treatment
*p < 0.05 vs. healthy; ap < 0.05 vs. OSAHS (before treatment).
The SNAP-IV scores of healthy and OSAHS children, as well as OSAHS children before and after treatment. *p < 0.05.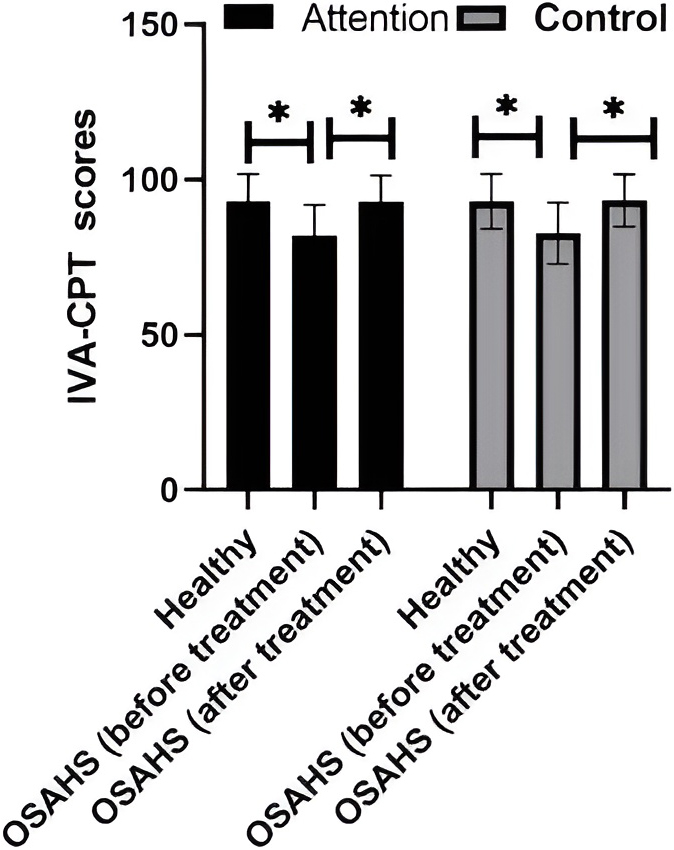
Comparison of the IVA-CPT scores of healthy and OSAHS children, as well as OSAHS children before and after treatment
*p < 0.05 vs. healthy; ap < 0.05 vs. OSAHS (before treatment).
The IVA-CPT scores of healthy and OSAHS children, as well as OSAHS children before and after treatment. *p < 0.05.
The SNAP-IV scores of OSAHS children before and after treatment were compared. The SNAP-IV score 3 months after surgery was significantly lower than before (Fig. 2). Moreover, the IVA-CPT score in children with OSAHS was significantly improved after surgery compared to before surgery (Fig. 3). These results suggested that surgical treatment could improve cognitive abilities in children with OSAHS.
Surgical treatment might reconstruct the brain structure and function of children
Rs-fMRI data was processed using ReHo and corrected through GRF to objectively reflect the functional state of the brain. In OSAHS children, there was a marked decrease in ReHo levels in the right angular gyrus, the right precuneus, the left parahippocampal gyrus, and the left middle frontal gyrus, and an apparent increase in ReHo levels in the right posterior cerebellum (Table 4). Furthermore, the ReHo value of brain regions in children with OSAHS after surgery was higher than before treatment, including the right precuneus, right temporal lobe, right posterior cingulate gyrus, and left limbic lobe (Table 5). These results showed that surgical treatment might reconstruct children’s brain structure and function.
Analysis of the differences in ReHo values between OSAHS children and healthy children (ReHo values were corrected through GRF,
0.005)
Analysis of the differences in ReHo values between OSAHS children and healthy children (ReHo values were corrected through GRF,
Analysis of the differences in ReHo values before and after surgery in children with OSAHS (ReHo values were corrected through GRF,
Cognitive function refers to the ability of the human brain to process, store, and extract information [17], and attention and control belong to the basic cognitive functions of the human brain, which can demonstrate the daily behavior of children [18, 19]. The changes in regional brain activity, such as executive function, memory, and attention, maybe the neural basis for cognitive deficits in OSAHS patients [20]. Research has revealed that atrophy in the hippocampus volume and damage to white matter can lead to cognitive impairment [21, 22]. Animal studies have confirmed that recurrent nocturnal hypoxemia is one of the causes of cognitive impairment [23]. Tonsillectomy and (or) adenoidectomy can be the first choice of treatment for OSAHS in children. Wu conducted a study on 437 children with OSAHS diagnosed by PSG (aged 4–11 years), and the results showed that up to 30% of OSAHS patients had attention deficit hyperactivity disorder (ADHD) [24]. The incidence of ADHD in children with OSAHS had increased with the elevation of age, and the incidence of ADHD in boys with OSAHS was higher than that in girls with OSAHS [25]. Landau et al. found that preschool children with OSAHS showed significant impairment in executive function, impaired attention and receptive vocabulary, and more behavioral problems. After tonsillectomy, OSAHS children significantly improved speech and motor fluency, attention and vocabulary, and reduced behavioral issues [26].
Rs-fMRI, widely used to study various diseases with abnormal brain function, is a non-invasive functional detection technique that can reflect the spontaneous neural activity of the brain [27].
ReHo, a tool for analyzing rs-fMRI, can be used as an objective indicator to reflect brain function and neural activity in various brain regions [28]. There is no unified gold standard for evaluating the degree of cognitive impairment caused by OSAHS. The severity of OSAHS in children, the presence of comorbid conditions, and the duration of symptoms may have an impact on findings of cognitive function and brain structure. This study found that preoperative and postoperative fMRI can be used as a tool to evaluate the effectiveness of surgical intervention for OSAHS in children. This finding has important implications for clinical practice. fMRI can more accurately assess the patient’s nervous system function and cognitive ability, and track changes in condition before and after surgery. Meanwhile, this study provides a theoretical basis supporting the idea that tonsillectomy and/or adenoid resection could significantly improve cognitive dysfunction and reconstruct brain function and structure in children with OSAHS.
When OSAHS allocates attention abnormally, and the processing of control does not reach the expected level, it exhibits attention deficit hyperactivity disorder, possibly manifested as attention deficit hyperactivity disorder [29]. In this study, the SNAP-IV score of OSAHS children was significantly higher than that of healthy children. However, the IVA-CPT score of OSAHS children was significantly lower than that of healthy children and fell below normal values, indicating that OSAHS might cause cognitive impairment to some extent. After surgical treatment, the SNAP-IV and IVA-CPT scores of OSAHS children were significantly lower and higher than before surgery, indicating that the patient’s cognitive ability improved compared to before surgery. In addition, post-surgery scores of SNAP-IV and IVA-CPT in the OSAHS group approached those of the healthy group, indicating a positive effect of surgery.
In our study, compared with normal children, the ReHo values of OSAHS children in the right angular gyrus, the right precuneus, and the left middle frontal gyrus of the left parahippocampal gyrus were lower. The right angular gyrus, right precuneus is related to cognitive processes such as attention, memory, and spatial perception [30]. Additionally, the hippocampus is a part of the brain structure that is closely related to physiological functions such as sleep and is the main brain structure for neuropsychiatric activities such as recalling the past to generate memories and imagining the future [31]. However, the ReHo values in the right posterior cerebellum were higher, suggesting that there might be abnormalities in the function and structure of multiple brain regions. Three months after surgery, the ReHo values of the right precuneus, right temporal lobe, right posterior cingulate gyrus, and left limbic lobe increased compared to before surgery.
The main functions of the frontal lobe are attention, executive power, decision-making, and the differences and similarities between decisions, as well as long-term memory [32, 33, 34]. Research has reported that executive dysfunction in OSAHS patients might be caused by abnormal connectivity of the dorsolateral prefrontal lobe function [35]. In this study, the decrease in middle frontal gyrus consistency in children with OSAHS may be a response to the decrease in patients’ sustained attention and cognitive flexibility. The cerebellum is an important motor regulatory center and participates in regulating various non-motor functions [36, 37]. Cerebellar gray matter atrophy has been revealed to be related to dysfunction [38].
Our data showed an increase in ReHo values in the posterior cerebellar lobe of children with OSAHS, possibly due to local hyperperfusion in the cerebellar region to adapt to abnormal sleep-wakefulness transition during apnea. The precuneus is related to the activities of advanced nervous function. The posterior cingulate is connected to the hippocampal memory system [39]. The abnormal neural activity in the above regions plays an important role in OSAHS-related cognitive impairment. The temporal lobe is an extremely complex area in the cognitive field [40]. When it has abnormal changes, patients may have symptoms such as memory loss and even seizures [41]. The current study showed an increase in the ReHo value of the temporal lobe, which might be related to the recovery of brain DMN function to a certain extent after surgery.
Limitations still existed in this study. The study included only 40 children with OSAHS and 40 healthy controls, which may limit the generalizability of the findings. A larger sample size could provide more robust and generalizable results. The follow-up period was limited to three months post-surgery. Longer follow-up is necessary to understand the long-term effects of tonsillectomy and/or adenoidectomy on cognitive function and brain structure in children with OSAHS. There may be other confounding factors such as socioeconomic status, education level, and overall health that were not controlled for, which could affect cognitive outcomes. The study used the SNAP-IV and IVA-CPT tests, which might not capture all dimensions of cognitive function. Utilizing a broader range of cognitive assessments could provide a more comprehensive understanding. Additionally, In this study, the lack of baseline characteristic data, such as BMI, is acknowledged, which might influence the results. Previous research indicates that factors like obesity (BMI greater than 30 kg/m2), mandibular or maxillary shortening, hypothyroidism, acromegaly, male gender, middle age (40–65 years), genetic conditions (e.g., myotonic dystrophy, Ehlers-Danlos syndrome), and smoking are significant contributors to the occurrence of OSAHS [42]. Given that our study focused on pediatric patients and examines the effects of surgery on cognitive function and brain structure, we did not record baseline data such as BMI. In future studies, we plan to include these factors to provide more comprehensive and accurate results. Additionally, we recommend that other researchers consider these baseline characteristics when designing similar studies to better understand the impact of OSAHS on cognitive function and brain structure.
Conclusions
In summary, OSAHS children exhibited cognitive dysfunction and multiple functional abnormalities in brain regions, and after receiving surgical treatment, their cognitive function was significantly improved, and the consistency of neural activity in some brain regions was enhanced.
This study uses fMRI technology, post-processing, and scoring systems to support changes in brain structure and function in OSAHS patients. In addition, longitudinal studies to track the long-term effects of surgical treatment on brain function and structure, or studies to explore the mechanism underlying the observed changes.
Funding
This work was supported by the Startup Fund for scientific research, Fujian Medical University (Grant number: 2020QH1275).
Ethical approval
This study was approved by the Quanzhou First Hospital ethics committee, affiliated with Fujian Medical University. Signed written informed consent was obtained from the patients and/or guardians.
Author contributions
CL and SC designed the study and performed the experiments, QL collected the data, YH analyzed the data, and CL and SC prepared the manuscript. All authors read and approved the final manuscript.
Footnotes
Conflict of interest
The authors have no potential conflicts of interest to report relevant to this article.