
Abstract
BACKGROUND:
non-small cell lung cancer (NSCLC) accounts for more than 80% of all lung cancer populations. Stereotactic radiotherapy (SBRT) is mainly suitable for early NSCLC patients who are not suitable for surgery or refuse surgery.
OBJECTIVE:
To analyze the effects of stereotactic radiotherapy (SBRT) plus immunotherapy for non-small cell lung cancer (NSCLC) patients on their immune status and survival quality.
METHODS:
NSCLC patients admitted to our hospital from 2019–2022 were divided into 61 cases in control group (SBRT) and 60 cases in observation group (SBRT plus immunotherapy) by the randomized numerical table method to compare the efficacy, the level of tumor markers in the serum, the level and activity of the immune cells in the peripheral blood and the Kahlil’s functional status (KPS) scores.
RESULTS:
The observation group had a higher efficacy rate than that of the control group (
CONCLUSION:
SBRT plus immunotherapy can reduce the level of various tumor markers, improve the immune status and quality of survival for NSCLC patients.
Keywords
Introduction
As a relatively common category of lung cancer, non-small cell lung cancer (NSCLC) accounts for more than 80% of all lung cancer populations [1, 2]. Stereotactic radiotherapy (SBRT) is mainly suitable for early NSCLC patients who are not suitable for surgery or refuse surgery. It is also an important therapy for undirected stage III lung cancer. Studies have shown that it has a good disease control effect on NSCLC patients, and the toxic reaction is milder than traditional radiotherapy [2, 3, 4]. However, it is common to have regional or distant recurrence, or a combination of both after SBRT treatment alone [4, 5]. Therefore, it is necessary to combine other treatment options to reduce disease recurrence rate and improve prognosis.
Immune cells in peripheral blood not only have a potential radiosensitization effect, but also have a clearing effect on tumor cells in the whole body [6]. Poor immune status of NSCLC patients will directly affect their quality of life and long-term prognosis. How to improve the immune function of NSCLC patients has been highly valued clinically [7]. With the changes in the treatment concept and treatment mode of NSCLC, immune checkpoint-related inhibitors have gradually been used in the treatment of this disease, which has greatly changed the treatment prospects of the disease [8]. However, clinical studies are still needed on how to choose a treatment plan for NSCLC patients, and studies on the efficacy of radiotherapy plus immunotherapy for NSCLC is still relatively limited.
This study aimed to analyze the impact of SBRT plus immunotherapy on the immune status and quality of life of NSCLC patients. Through in-depth research on the efficacy of SBRT plus immunotherapy on NSCLC, it is expected to provide a more effective and reasonable treatment plan for NSCLC patients, promote the improvement of their immune status and quality of life, and provide guidance for clinical practice.
Materials and methods
Research objects
A total of 121 patients with NSCLC were selected for the study. They were admitted to our hospital from December 2019 to December 2022, and were divided into control group (SBRT) and observation group (SBRT plus immunotherapy) by random number table method, with 61 patients in each group. Inclusion criteria: (1) All of them were confirmed to be NSCLC combined with pathological results; (2) Age was not less than 18 years old; (3) Pathological stage was I-III; (4) The estimated survival period was not less than 3 months; (5) Cartesian functional status (KPS) was not less than 50 points; (6) All were primary tumors. Exclusion criteria: (1) Severe dysfunction of liver, kidney, heart and other organs; (2) Those with immune diseases; (3) Those with cognitive abnormalities or mental illness; (4) Those who were allergic to the relevant drugs; (5) The presence of other primary tumors; (6) Those who refused to study or quit halfway. The study was approved by the medical ethics committee in the hospital, and the informed consent of patients or their families was obtained at the same time.
Methods
Control group
The control group was given SBRT. The operation steps were as follows: the patient was maintained in a supine position, and the hands needed to be in a cross-elbow state. Spiral enhancement scanning was carried out by positioning CT, and the thickness of the layer was set to 5 mm. During the scanning, it was from the upper edge of the cricoid cartilage to the lower edge of the liver. Scanning was carried out, the moving images obtained from the respiratory cycle were collected, as well as the amplitude of respiratory movement, and the target area was delineated. The gross target area of the tumor is: the planned target area obtained by extending 0.5 cm along the three-dimensional direction showing the primary tumor and local metastatic focus in CT examination, as well as the displacement of respiratory movement in different directions. The prescription dose of radiotherapy is as follows: The total dose was 50–60 Gy, and the single dose was 6–12 Gy. Treatment generally involved a 50% equidose curve wrapping around 100% of the planned target volume, a 70% equidose curve wrapping around 90% of the planned target volume, and the maximum dose level within the planned target area was between 130% and 150% of the prescribed dose. The dose calculation grid was 0.2 cm
Observation group
Immunotherapy was carried out in observation group on the basis of the former group, and the programmed death-1 (PD-1) inhibitor, namely Pembrolizumab Injection (Carlow MSD Ireland 100 mg: 4 mL registration certificate No. S20180019), was selected, totaling 100 mg. The drug was used by intravenous injection, and the dosage was fixed. Injection was carried out once at intervals of 3 weeks, and 4 treatments were carried out for a total of 12 weeks, namely 3 months.
Observational indicators
Clinical efficacy: The efficacy will be judged after the end of treatment, and complete response (CR): no lesion or duration Serum tumor markers: Before and after treatment, 3 mL fasting venous blood was extracted from the two groups. After anticoagulation treatment, they were placed at room temperature for 24 h, and centrifuged at low speed. The supernatant was selected and the contents of carcinoembryonic antigen (CEA), human squamous cell carcinoma antigen (SCCAg), neuron specific enolase (NSE) and cytokeratin 19 fragment (CYFRA21-1) were determined by enzyme-linked immunosorbent assay. The total was determined for 3 times. The average value of the 3 times was calculated as the final result, and the final result was accurately recorded. Immune status: 3 mL fasting venous blood were taken from the two groups before and after treatment, and the relative activities of CD3+, CD4+, CD4+/CD8+ and natural killer (NK) cells in peripheral blood were measured by flow cytometry. A total of 3 times were measured. The average value of the 3 times was calculated as the final result, and the final result was accurately recorded. Quality of life: Before and after treatment, the two groups were assessed by Karnofsky Performance Status (KPS). 100 points: there is no sign or symptom; 90 points: activities can be carried out normally, and there are mild signs and symptoms; 80 points: patients are able to move reluctantly, with some signs and symptoms; 70 points: patients can take care of oneself, but cannot maintain a normal state; 60 points: in most cases, patients can take care of themselves, and a few need the assistance of others; 50 points: patients need the care of others; 40 points: patients are unable to take care of themselves, special assistance is required; 30 points: patients are unable to take care of oneself; 20 points: the condition is in a relatively serious state, and should be hospitalized and receive supportive treatment; 10 points: seriously ill, close to death; 0: Already in a state of death [10].
SPSS 25.0 statistical software was used to analyze the data, and the counting data were expressed by [
Results
Comparison between two sets of baseline data
As shown in Table 1, there was no statistical difference between the two groups in baseline data such as gender, age, smoking history, family history, pathological type and tumor stage (
Comparison between two sets of baseline information
Comparison between two sets of baseline information
As shown in Table 2 and Fig. 1, the effective rate in observation group was higher than that in control group, and there was a statistical difference between the groups (
Comparison of efficacy between the two groups [
(%)]
Comparison of efficacy between the two groups [
Comparison of therapeutic effects between two groups.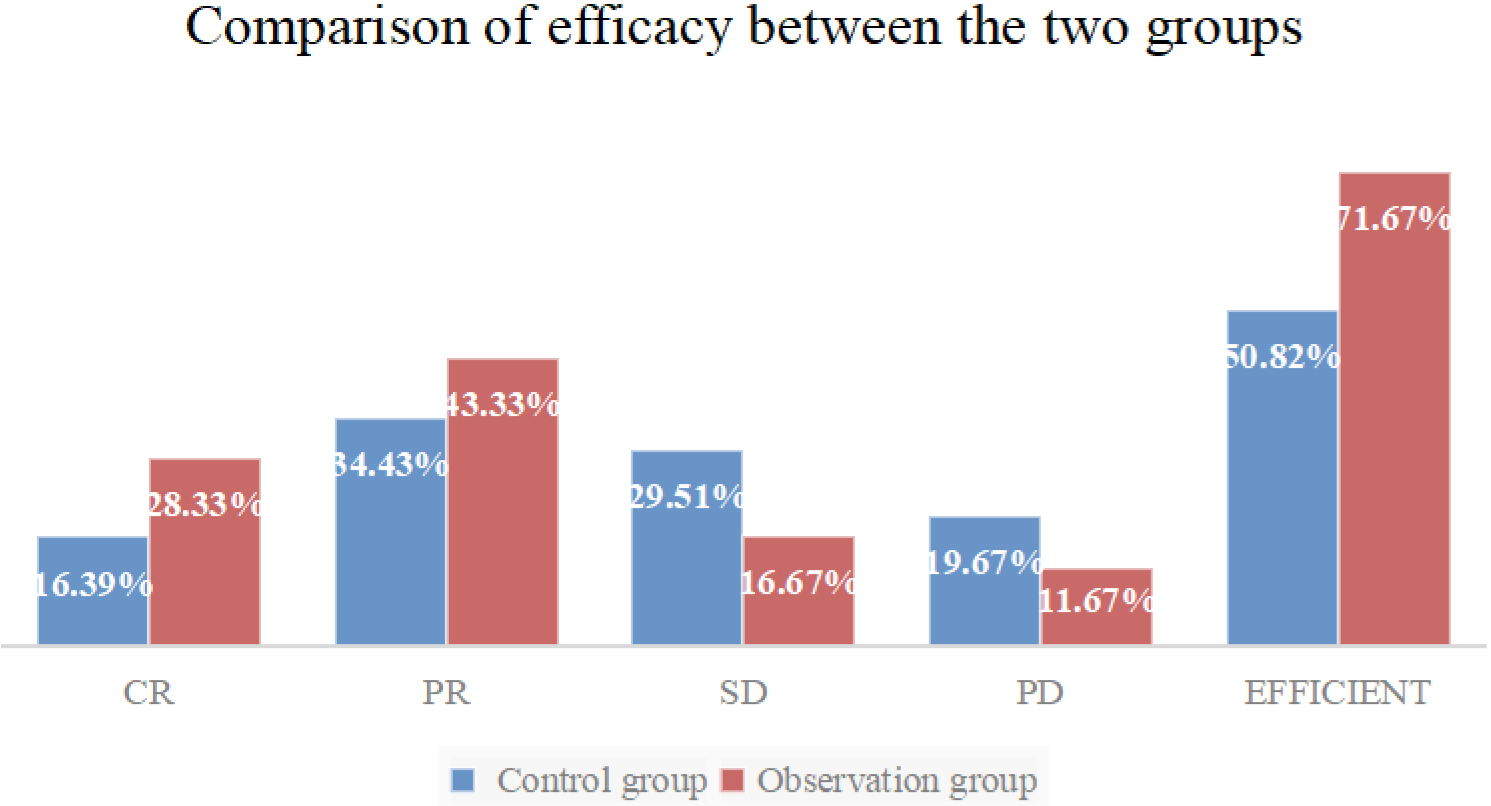
As shown in Table 4, there was no significant difference in serum CEA, SCCAg, NSE, and CYFRA21-1 levels between the two groups before treatment (
| Group | CEA | SCCAg | NSE | CYFRA21-1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before treatment | After treatment | Difference | Before treatment | After treatment | Difference | Before treatment | After treatment | Difference | Before treatment | After treatment | Difference | |
| Control group ( |
129.56 |
24.95 |
105.86 |
3.49 |
0.94 |
2.55 |
21.25 |
8.18 |
13.14 |
12.45 |
3.20 |
9.22 |
| Observation group ( |
128.78 |
58.92 |
70.34 |
3.45 |
1.52 |
1.93 |
22.04 |
11.72 |
11.04 |
12.50 |
6.05 |
6.44 |
|
|
0.275 | 37.720 | 14.658 | 0.468 | 16.245 | 9.700 | 1.534 | 10.578 | 5.946 | 0.148 | 26.156 | 12.779 |
|
|
0.784 |
|
|
0.641 |
|
|
0.128 |
|
|
0.883 |
|
|
Immune status of the two groups before and after treatment (
As shown in Table 4, there was no significant difference in peripheral blood CD3+, CD4+, CD4+/CD8+ and NK cell activities between the two groups before treatment (
Comparison of KPS scores between the two groups before and after treatment (
, points)
Comparison of KPS scores between the two groups before and after treatment (
Note: Compared with those before treatment in the same group, *P< 0.05.
As shown in Table 5, there was no significant difference in KPS scores between the two groups before treatment (
Discussion
At present, lung cancer still occupies an important position in cancer-related deaths, and the main treatment measures include surgery, radiotherapy and chemotherapy, immunotherapy and targeted drugs [11]. In the past few decades, radiotherapy technology has made great progress, and it has been popularized in the radical treatment, preventive treatment and palliative treatment of NSCLC [12]. Molecular diagnosis and immunotherapy have opened up new treatment directions for NSCLC patients, such as PD-1 related inhibitors, which significantly prolong the survival of NSCLC patients [13]. However, the treatment measures for patients with advanced NSCLC are relatively limited, the treatment is difficult, and the prognosis is poor [14]. Therefore, it is necessary to explore a more suitable treatment plan for this type of patients.
The effective rate is the main reference index to evaluate the efficacy of NSCLC. Wagner G [15] et al. found that radiotherapy plus immunotherapy can improve the efficacy of NSCLC. This study also found that SBRT plus immunotherapy is more effective in NSCLC patients. On the one hand, SBRT can affect the anti-tumor immune response caused by tumor cell DNA, making tumor cells produce immunogenic death, which plays a key role during cancer treatment [16]. On the other hand, the addition of PD-1 inhibitors can play a synergistic role. SBRT can induce a systemic anti-tumor immune response and improve the sensitivity of tumors to immunotherapy. SBRT further activates the immune system to attack tumors through its high-dose and precise radiotherapy characteristics. Meanwhile, PD-1 inhibitors enhance the immune system’s ability to recognize and kill tumor cells by regulating the immune system. This combined application not only enhances positive immune regulation, but also significantly weakens negative immune resistance, possibly by promoting immunogenic cell death of tumor cells and further activating the immune system, thus enabling patients to obtain more ideal efficacy [17].
Tumor marker determination is a common method in tumor screening and evaluation of malignancy. Combined with changes in the level of indicators including CEA, NSE, SCCAg, CYFRA21-1 before and after treatment, it can quantitatively evaluate the efficacy of patients [18, 19]. After treatment, the serum tumor markers in observation group were lower than those in control group. PD-1 is an immunosuppressive transmembrane protein expressed on the surface of T cells. It primarily limits T cell activity in chronic inflammation, infection, or cancer [20]. In the tumor microenvironment, tumor cells can express PD-L1 or PD-L2, which can bind to PD-1 on the surface of T cells, preventing T cells from detecting and attacking tumor cells. PD-1 inhibitors can regulate the immune system, downregulate its response to human cells, and inhibit T cell inflammatory activity, thereby preventing autoimmune diseases [21]. On the basis of SBRT, PD-1 inhibitors can up-regulate the PD-1 ligand of tumor cells, activate T cells in a consistent manner, and play an immune surveillance role on the lesion, fully block the PD-1 activities, so that cancer cells are eliminated, the proliferation of cancer cells is reduced, and the levels of various tumor markers in serum is finally reduced [22].
The level of immune cells and the activity of NK cells are common indicators for evaluating the immune status of the body. Because most NSCLC patients are in the advanced stage of the disease, there will be inhibition in the immune function. Immune dysfunction will directly affect the elimination effect of cancer cells [23]. Lu Wanling [24] et al. found that radiotherapy plus immunotherapy can improve the immune function of NSCLC patients. This study also found that the combination therapy can improve immune function. After treatment, the levels of immune cells and the activity of NK cells in observation group were higher than those in control group. The main reason is that PD-1-related inhibitors are added on the basis of SBRT. As an important class of drugs during immunotherapy, after use, it can relieve the inhibition of T cells, enhance the activation, proliferation and function of T cells, and improve Immune status, thereby improving the immune system’s ability to attack tumor cells.
KPS score is an important index to evaluate the quality of life of cancer patients. The lower the score, the worse the quality of life. Silvia S [25] et al. found that radiotherapy plus immunotherapy can improve the quality of life of NSCLC patients. This study also concluded that the KPS score in observation group after treatment was higher than that in control group. This is because the combination therapy can play a better anti-tumor effect, exert an ideal inhibitory effect on the proliferation of cancer cells, promote the apoptosis of cancer cells, and slow down the growth rate of lesions, thereby reducing the impact of disease progression on patient survival quality.
There are still limitations in this study. For example, all NSCLC patients who received treatment in our hospital within a specific time frame are included, which may lead to limitations in the sample. Future research can compensate for limitations through more refined design and larger sample multicenter studies. There are potential biases or uncontrollable confounding factors in the study, such as clinical characteristics of patients, treatment parameters, and potential adverse reactions to treatment. It is necessary to strictly screen patients, comprehensively evaluate their condition characteristics, and ensure that the treatment plan is suitable for a specific patient group, taking into account their overall health status, past treatment history, and possible adverse reactions, in order to develop personalized treatment plans. It is also limited by research time, lack of long-term follow-up results of indicators such as survival time and survival rate. There was no data statistics and assessment related to toxicity, the indicators obtained are not perfect. Future studies are needed in the future. Despite these limitations, this study brings substantial support to the development of treatment protocols for patients with NSCLC. This effective and feasible treatment plan is expected to be widely used in actual clinical work to improve the efficacy and prognosis of NSCLC patients.
In conclusion, there is an ideal effect of SBRT plus immunotherapy for NSCLC patients. It can reduce the level of various tumor markers, and improve immune status and quality of life, with great application value.
Funding
The authors report no funding.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical approval
The study was approved by the Ethics Committee of Zhongyi Northeast International Hospital Co., Ltd.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.