
Abstract
BACKGROUND:
Clinically, apical barrier procedure can be adopted to create an immediate artificial barrier for tooth with an open apex. Given that the quality of the barrier is crucial, the apical barrier procedure is known for its high technical sensitivity, posing significant learning challenges for dental students. Therefore, a new dental teaching model not only effectively enhances the future clinical skills of dental students but also benefits a wider range of patients.
OBJECTIVE:
A new dental model for simulating apical barrier procedure in vitro, is helpful for dental students to practice apical barrier procedure. This study aims to design, assess, and evaluate the feasibility of a three-dimensional (3D) printed apical barrier model for pre-clinical dental education.
METHODS:
A novel 3D-printed apical barrier model was developed, consisting of a tooth model and a matching blind box. Total 200 3D-printed apical barrier models were used to train dental students, and fifty fifth-year dental students participated in this voluntary hands-on course. Each student performed apical barrier procedures on four 3D-printed models. The outcome of the first model served as the representative result for the “direct barrier group”, whereas the outcome of the fourth model represented the result of the “post-training barrier group”. The quality of the apical barrier procedure was assessed through X-ray examination, and a questionnaire was used to evaluate the 3D-printed model’s benefits, with scores ranging from 1 (strongly agree) to 5 (strongly disagree).
RESULTS:
The overall rating for the 3D-printed model was 2.0
CONCLUSIONS:
Both the questionnaire feedback and the quality of the fillings confirmed the feasibility and efficacy of the 3D-printed apical barrier model for dental education. The students had the possibility to learn the correct apical barrier procedure on printed dental models.
Keywords
Introduction
Apexification, or root-end closure, is the process in which a nonvital, immature, permanent tooth is induced to form a calcified barrier at the root terminus, when the tooth has lost the capacity for further root development. During this process, the formed barrier helps to form a matrix, which is called “apical stop” in root canal treatment, against which root canal filling or restorative material can be compacted with length control [1]. As an advanced technique, apical barrier technique is a new method to fast form “apical stop” for tooth with open apex. For apical barrier technique, a 4- to 5-mm plug of mineral trioxide aggregate or iRootBP Plus is placed at the root end, and the canal space is subsequently restored with dual-curing composite resin, often accompanied by a fiber post to provide mechanical support [1]. The formation of the apical barrier is the most important step in this procedure, and it is also difficult to master, so dental students need more practice to perform this procedure proficiently.
The pre-clinical training can allow students to gain similar clinical practice experience easier and faster, not only to master the standardized operation procedures but also to have a deeper understanding of possible operation errors, and to have the ability to find and solve the problems in clinical operations. Considering the difficulty of obtaining isolated teeth, and the large individualization variability of these teeth, the evaluation of operation procedures is always subjective and thus lacks consistency between evaluators, so the usage of artificial plastic tooth models is a common option for pre-clinical training, rather than traditional isolated teeth. Currently, with the development of digital technology and three-dimensional (3D) printing technology, duplicated tooth models are designed and produced, which have been frequently used in dental education [2]. For example, the 3D-printed models used in dental pre-clinical training include crown preparation [3], access preparation [4], caries excavation, direct capping of the pulp, core build-up [5], and crown preparation [6, 7, 8], even veneer preparation [9], etc. The final aim of 3D-printed model is to simulate the real clinical situation [10], such as the three-color tooth models for crown preparation [5], veneer preparation [8], inlay preparation [11], which are chosen to simulate the three layers of tooth structure: enamel, dentin, and pulp cavity, and making students easier to control the range of clinical preparation. Robberecht et al. studied a hydroxyapatite matrix material with a porous surface and hardness similar to that of dentin. This material can be used for 3D printing, and the feel of cutting the material with endodontic files is similar to that of cutting dentin in clinical practice, making it suitable for pre-clinical practice of root canal treatment [12]. For dental education, the current studies suggest that the application of 3D-printed models facilitates the production of functional and personalized teeth models at a significantly reduced cost and allows students to gain pre-clinical training and can have a positive impact on the educational experience of dentists [10].
Apical barrier procedure is a good choice for immature permanent teeth with pulp necrosis or apical periodontitis, with few visits and a good closure effect [13]. Apical barrier procedure has high technical sensitivity and few clinical cases [14], and there is a contradiction between the missing opportunities for clinical practice and the missing pre-clinical training. So, there is a strong demand for educational teaching models for apical barrier procedure. The acquisition of isolated teeth is inherently difficult, even the isolated teeth with open root apical foramen [15]. Therefore, it is a good solution to use 3D printing technology to obtain a model of immature permanent teeth with open apical foramen and use it to train apical barrier procedure. This study aimed to design a 3D-printed apical barrier model to simulate an immature permanent tooth with an apical bony defect for dental education of apical barrier procedure, and use it to perform pre-clinical training. After that, the simulated clinical outcomes were evaluated by X-ray examination, and the benefits of endodontics education with this model were evaluated by questionnaires.
At present, it is held that utilization of 3D-printed models for training in apical barrier procedures exerts a beneficial influence on the educational journey of undergraduate students. Furthermore, it is believed that those models will also have a positive impact on the educational experience of graduate students and even general practitioners.
Material and methods
Design and production of 3D-printed apical barrier model
The Cone Beam Computed Tomography (CBCT) of a mandibular premolar with completed root development (in .dcm format) was selected and imported into Mimics 21.0 software (Materialise NV, Leuven, Belgium) (Fig. 1A) to obtain the external anatomical morphology of the mandibular premolars. This was stored in .stl format and subsequently imported into 3ds Max 2022 software (Autodesk, San Rafael, USA). Finally, the root canal shape was designed as an open, oval cylindrical root canal with a length of 17 mm. The buccolingual diameter of the apical foramen was set to 2.9 mm, while the mesiodistal diameter was 1.3 mm, based on the apical foramen data obtained from the pre-experiment (data not shown) (Fig. 1B-D). Additionally, the pulp cavity was open. The blind box model (Fig. 1E) (12 mm
Establishment and print of the apical barrier model. (A) 3D reconstruction of normal mandibular premolar; (B-D) the root canal shape was designed as an open, oval cylindrical root canal, with an open pulp cavity; (E) the designed model tooth is placed in the blind box; (F) the internal structure of the blind box, a semicircular cavity was set at the bottom of the blind box; (G) the printed tooth model; (H) the printed tooth model is placed in the printed blind box (finished apical barrier model). 
A total of 50 dental students (19 males and 31 females) in their fifth year of undergraduate study participated in this voluntary, hands-on course when they were ready for clinical training in the Department of Endodontics, West China Hospital of Stomatology, Sichuan University. All students were in the first clinical course in endodontics and were included in this voluntary hands-on course after the induction standardized training in the Department of Endodontics, including the training in dental operation microscopy and the theoretical training of apical barrier procedure. All 50 participants received informed consent to participate in this voluntary course.
Apical barrier procedure
The same instructor trained the students on the theory of the apical barrier procedure. For this course, the apical barrier material utilized was the calcium-silica cement known as iRootBP Plus, produced by Innovative BioCeramix in Vancouver, Canada (alternatively referred to as Endosequence). The detailed process proceeded as follows. Under a dental operating microscope, the iRootBP Plus was precisely inserted into the root apex with a marked vertical plugger. Subsequently, appropriate pressure was applied until the apical segment was densely filled with 4–5 mm of iRootBP Plus. Following this, a damp cotton ball was positioned in the middle and upper section of the root canal, and the pulp chamber was temporarily sealed. Lastly, the positioning and the filling quality of the barrier material in the apical area were verified through X-ray imaging captured from both buccolingual and mesiodistal angels.
Apical barrier model training
In this study, each student was afforded the opportunity to manipulate four identical apical barrier models. Initially, all the students executed the apical barrier procedure on a single model, subsequent to which X-rays were acquired. The outcomes of this initial phase were categorized as the “direct barrier group”. After that, the students underwent training sessions utilizing two additional apical barrier models. During these training sessions, the students had the flexibility to extract the 3D-printed teeth models at any point for closer inspection, enabling them to identify flaws in their filling technique and maintain meticulous control over the entire filling process. Ultimately, post-training, all the students directly applied the apical barrier procedure on the fourth model, and upon completion, X-rays were once again obtained. The results of this final phase were designated as the “post-training barrier group”.
Apical barrier quality assessment
According to the X-ray results, an analysis of the apical barrier quality was conducted. The gray value was employed as a metric to assess the density of the barrier filling by Image-Pro Plus 6.0 (Media Cybernetics, Inc.). Concurrently, the extent of the apical barrier material beyond the apex was quantified. Specifically, a distance of 0 mm was designated as “suitable-filling” (Fig. 2A), indicating optimal placement. A negative distance denoted “underfilling” (Fig. 2B), where the material did not reach the desired level. Conversely, a positive distance indicated “overfilling” (Fig. 2C), where the material extended beyond the apex. The degree of overfilling was further categorized by comparing it to the height of the cube (14.5 mm), distinguishing as
The questionnaire for the evaluation of 3D-printed apical barrier model
The questionnaire for the evaluation of 3D-printed apical barrier model
Judgment of suitable-filling, underfilling, and overfilling (representative picture). (A) suitable-filling, (B) underfilling; (C) overfilling. Left is buccolingual root angulation, right is mesiodistal angulation. The horizontal line is point to the root apex plane, as the red dotted line shown. The height of the cube is 14.5 mm, as the red double-arrow line shown.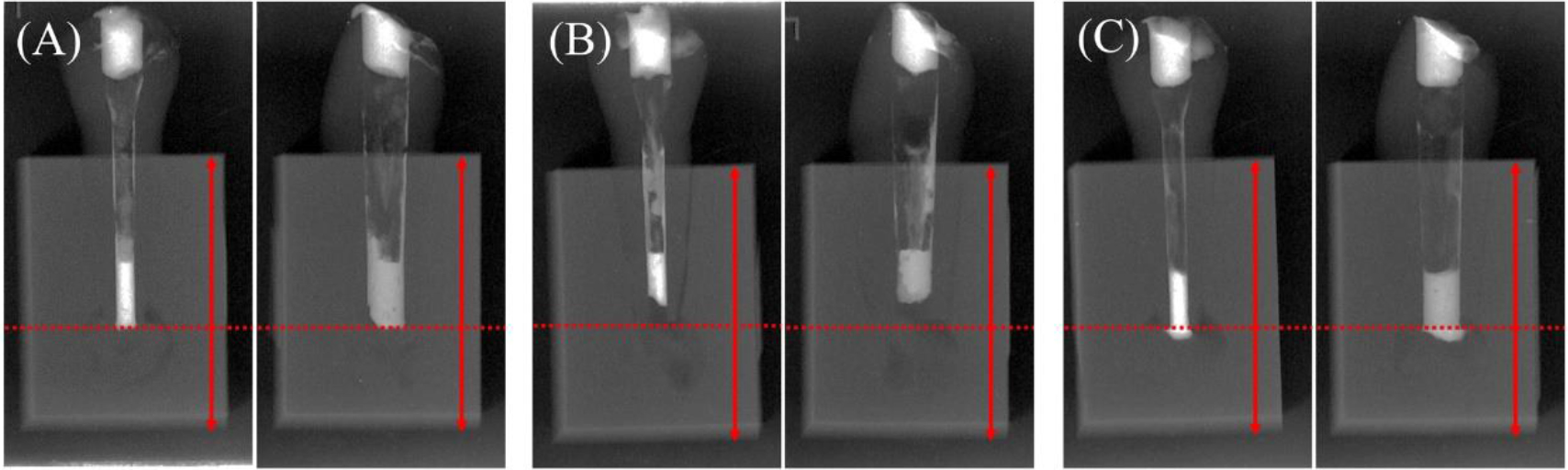
For self-assessment of clinical proficiency, 50 students engaged in an online questionnaire tailored specifically for their experience with the 3D-printed apical barrier model. This comprehensive questionnaire encompassed five distinct sections (outlined in Table 1): (1) personal information; (2) key features of 3D-printed apical barrier model; (3) assessment of learning outcomes achieved through its utilization; (4) assessment of the learning process facilitated by the model; and (5) free-text questions. Responses were graded on a 5-point Likert scale (1
Statistical analysis
To ensure the reliability of the analysis, Cronbach’s alpha was calculated. The collected data underwent rigorous examination utilizing SPSS Statistics 20.0 software (IBM Corporation). The questionnaire outcomes were meticulously determined by averaging the scores for each question and computing overall scores. The given scores were presented as percentages, accompanied by the respective mean values and standard deviations, providing a comprehensive view of participants’ responses. To compare the filling density between the first and fourth models, a paired students’ T-test was employed. Furthermore, the overall filling quality was analyzed for changes before and after training using the Chi-squared test. Statistical significance was set at
Results
The internal consistency of the questionnaire was high (Cronbach’s alpha of 0.895), and no significant impact of the age or gender of the participating students was detectable.
The students’ evaluation of the 3D-printed apical barrier model for apical barrier procedure. Note: see Table 1 for items.
The features of the 3D-printed apical barrier model were evaluated as agree (Fig. 3, items 2.1–2.3), and the total score was 2.0
Comparison of the filling density between “direct barrier group” and “post-training barrier group”
Comparison of the filling density between “direct barrier group” and “post-training barrier group”
*
Comparison of the filling quality between “direct barrier group” and “post-training barrier group”
*
Results of the statistical analysis are shown in Tables 2 and 3. There is a significant difference in the density of apical barrier filling between direct barrier group and post-training barrier group (
A similar result is the learning outcome assessment of the questionnaire, rated as strongly agree to agree (1.06
Assessment of the learning process with the 3D-printed apical barrier model
The last part of the questionnaire assesses the student’s learning process. The printed apical barrier model not only met the expectations of the students (Fig. 3, items 4.1) but also satisfied the student’s desire to use the training model before the actual patient treatment (Fig. 3, items 4.2), both were rated as strongly agree to agree (2.16
Free-text questions
Fifty students were asked to give their opinions on the 3D-printed apical barrier model used in this hands-on course. The results of the free-text questions were analyzed, and similar answers were combined and counted.
Firstly, the suggestions for improving the 3D-printed apical barrier model include: (1) it is hoped that it can be installed on a dental teaching head model to further simulate the intraoral environment (
Secondly, the advantages of the model mainly include: (1) the translucency and detachable design, which make it possible to directly observe the filling status, which is conducive to the targeted improvement of filling operation (
Discussion
For students who are new to clinical practice, there are few clinical hands-on opportunities to approach apical barrier procedure in clinical practice. To acquire basic apical barrier manipulation skills, pre-clinical training is required. The pre-clinical training in endodontics mostly focuses on caries removal, pulp opening, root canal preparation, root canal filling, inlay preparation and full crown preparation [2, 5, 6, 7, 8, 16], but lacks of pre-clinical training for revascularization, apexification, and apical barrier procedure. The possible reason is due to the lack of corresponding teaching models. First, it is hard to obtain isolated immature permanent teeth, and secondly, if the normally developed isolated teeth are used to prepare into immature permanent tooth-like apical foreman, it is easy to cause thin walls and fractures or micro-cracks [15]. Therefore, it is necessary to construct a 3D-printed apical barrier model to carry out pre-clinical training of apical barrier procedure, improve students’ cognition, and enrich pre-clinical training programs in dental school.
In this hands-on course, the 3D shape of the tooth was reconstructed according to the Digital Imaging and Communications in Medicine (DICOM) format obtained by CBCT scanning, and the apical barrier model was designed with a parallel root canal. The tooth models are uniformly designed as an opened pulp chamber, which reduces the possible errors due to inconsistent pulp opening, as this model is focused on training apical barrier procedure rather than pulp opening procedure. In this 3D-printed model, referring to the division of the apical foreman diameter for pulp regeneration [17] and the largest size of commercial vertical plugger [18], the apical foreman diameter was designed to be 2.9 mm
When treating immature permanent teeth, the difficulty focuses on the closure of the apical area, so the filling density, underfilling rate, and overfilling degree could have a great impact on the outcome of treatment [19, 20]. That is why the quality of filling outcomes was evaluated through these aspects by X-ray examination. The hands-on course results also showed that the filling density was significantly improved, the underfilling rate and overfilling range were significantly decreased. These assessments help to show the functions of 3D-printed apical barrier model in pre-clinical training.
To ensure the consistency of the students participating in the voluntary course, students were selected from the same grade with the same clinical experience, education level, and teacher. Although there were more female students, the questionnaire evaluation showed that there was no difference between males and females. To prove that the 3D-printed apical barrier model can improve students’ cognition and operation skills of apical barrier procedure, the “direct barrier group” and “post-training barrier group” were specially designed, which is good to demonstrate the importance of model training.
The 3D-printed model evaluation questionnaire is designed as closed format rating scale questions, referring to the questionnaire preliminarily developed and validated by the “Institute for Medical Teaching and Medical Educational Research" of the university [16]. The questionnaire has been tested in endodontic clinical training by 3D-printed tooth models, with high consistency and reliability [5, 6], and could modified to meet the needs of another course [11] and our course. Combined with results of the questionnaire analysis, the students recognized that the model could improve their understanding and operation skills of apical barrier procedure, and they could see the filling quality more intuitively.
In the questionnaire, the total score of the apical barrier model was 2.0
Given that this study was solely conducted within our dental school’s confines, the findings may not be universally applicable to students pursing other disciplines or attending other institutions. The mechanical properties of existing materials differ greatly from those of dental tissues, and the cost of mass-producing three-dimensional models is relatively high. Furthermore, there is a shortage of professionals specializing in creating 3D models. However, the AI-driven one-click design model is expected to simplify the design process of dental education models through full intelligence, and our hypothesis has been confirmed that a 3D-printed apical barrier model holds significant educational merits for the training of apical barrier technology.
Conclusion
A whole new model was created for training in apical barrier procedures and the functions of this 3D-printed apical barrier model were evaluated during the training process. The questionnaires and filling quality proved that the teaching concept of the 3D-printed apical barrier model was feasible and the training was probably efficient. The printed model enabled students to learn how to perform apical barrier procedure, recognize their shortcomings, and support their self-education and learning. In addition, the proposed method can be adapted to different treatment training in immature permanent teeth like apical barrier, apexification, or pulp revascularization. We hope that the 3D-printed apical barrier model will be routinely used in laboratory courses for dental students and in daily practice for dental practitioners, to promote their operation skills shortly.
Ethical approval
The study was approved by the Institutional Review Board (WCHSIRB-D-2021-244), which is the ethics committee of West China Hospital of Stomatology, Sichuan University, and received an exemption.
Author contributions
Haojie Zou, Lei Wang and Xiaolu Zhou contributed to acquisition, analysis and interpretation of data and drafting and revising the manuscript. Ling Zhang, and Shida Wang have made substantial contributions to acquisition of data and revision the manuscript. Qinghua Zheng and Ling Ye were involved in the conduct of the experiment and revising the manuscript. Chenglin Wang contributed to design of the study and revise the manuscript critically.
Data availability
Data are available on request from the authors.
Footnotes
Acknowledgments
Thanks for the support of Sichuan Natural Science Foundation Project (2024NSFSC0551), Exploration and Research Projects (LCYJ-2022-YY-2, LCYJ2019-18), Soft Science Research Project (RD-01-202201, RD-01-202302) of West China Hospital of Stomatology, Sichuan University, and the 10th Higher Education Teaching Reform Project of Sichuan University (SCU10381). The authors thank dental students from Sichuan University participating in the study.
Conflict of interest
The authors have no conflict of interest to disclose.