
Abstract
The primary goal of the vestibular implant is to restore the vestibular function in patients with a disabling bilateral vestibular loss for whom there is currently no available treatment. The prototype developed by our team is a hybrid system consisting of a modified cochlear implant incorporating additional vestibular electrodes. Therefore, in addition of delivering sound information it is also capable of delivering motion information to the central nervous system using electrical stimulation. To date, thirteen patients have been implanted with such vestibular implant prototypes. For ethical reasons, only deaf ears were implanted and all patients experienced a clinical benefit from the hearing rehabilitation. The recent demonstration of partial restoration of the vestibulo-ocular and the vestibulo-collic reflexes in implanted patients suggests that gaze stabilization and postural control, fundamental functions of the balance system, can be artificially restored using a vestibular implant. This allows us to glimpse a useful clinical application in a near future. In parallel, we show how the vestibular implant provides a unique opportunity to explore the integration of the vestibular sensory input into the multisensory, multimodal balance system in humans, since it is able to selectively stimulate the vestibular system.
Introduction
In general, the society recognizes that the loss of sensory function is an important handicap. However, certain conditions are better recognized and understood than others. Good examples of well recognized, disabling conditions are blindness (loss of sight) and deafness (loss of hearing). In these cases, important efforts in the management of affected patients have been undertaken. Unfortunately, the picture is completely different for other conditions. The handicap suffered by patients with a complete loss of the vestibular function is significantly underestimated and the pathway to diagnosis is full of hurdles [46, 64]. However, recent studies have unambiguously revealed that the complete loss of the vestibular function has a dramatic impact on the quality of life of affected patients [22]. It also represents significant economic burden for patients and society [58].
The clinical management of patients with bilateral vestibular loss remains difficult as there is no clear evidence for an effective treatment. Physical therapy showed no [68] or limited benefit [18]. Other treatment options such as sensory substitution with auditory or vibrotactile feedback have shown contrasting results and are still under clinical investigation [30, 43]. Recent spectacular results showing the successful differentiation of stem cells into functional hair-cell-like cells and auditory neurons that are similar with the vestibular neurosensory cells, allow the wildest hope for the future [9]. However, it might still be long before this promising therapeutic pathway can be successfully translated to the clinic.
These important facts support the vestibular implant research efforts that have been launched more than 15 years ago primarily to rehabilitate patients with a bilateral vestibular loss. Promising results have been obtained in animal models and humans and partial restoration of the vestibular function has been demonstrated [12, 51]. Moreover, awareness among the medical community, funding agencies, and specialized industry (in particular the cochlear implant companies) has substantially increased in the last years. Hopefully, this rising interest will boost research in the field allowing, in the near future, the availability of a vestibular implant able to restore useful vestibular function and help “normalize” balance in patients with a severe bilateral vestibular loss. Another interesting aspect of vestibular implant research is that this device constitutes a unique opportunity to develop fundamental knowledge in the vestibular research field, in particular by providing unprecedented, selective, and direct access to the vestibular endorgans.
Vestibular function
The peripheral vestibular organ is located in the inner ear and is composed of five special sensory organs (i.e., endorgans) dedicated to sensing head movements. The three pairs of semicircular canals are sensitive to angular acceleration, providing cues about three-dimensional head rotations. The otolithic organs (saccule and utricule) are predominantly sensitive to linear acceleration, providing cues about 3D head translations, including gravity. This motion information allows unambiguous real time monitoring of head position and movement. Unlike other sensory organs, vestibular input quickly becomes multimodal (i.e, multisensory) in subcortical structures, at the level of the second neurons. A direct consequence of this is that there is no clear conscious or distinct sensation coming from the vestibular endorgans alone. Yet, vestibular information is involved in a large variety of subcortical and cortical functions, which is illustrated by the multifocal brain activation observed to different vestibular stimuli [42].
Vestibular information is fundamental for a variety of functional aspects. Vestibular reflexes play a central role in the balance system. The vestibulo-ocular reflex (VOR) mediates gaze stabilization in dynamic conditions, while the vestibulo-spinal (VCS) and vestibulo-collic reflexes (VCC) are important for postural control. Motion perception is another function that relies on complex integration of vestibular input. For example, integration of canal and otolithic information in an internal model is necessary to solve the ambiguity between a tilt and a translation in the horizontal plane [45]. We also know that motion related information affects the activity of hippocampal place cells which are essential for spatial navigation [8, 33]. Moreover, the vestibular input interacts with the autonomic system for the regulation of arterial blood pressure during gravity changes [21], or during head-up tilt [59]. There is even some evidence that vestibular dysfunction could play a role in orthostatic hypotension [2]. Other authors have shown interactions with the respiratory system [67] and with sleep patterns [10]. Finally, the multiple vestibular projections are known to influence emotions, memory, cognition [16, 57] and even personality [56].
Bilateral loss of the vestibular function
In patients with a bilateral vestibular loss, imbalance is probably the predominating symptom. However, the global clinical picture involves functional impairments at different levels inducing a variety of symptoms which are not necessary flagrant. Additionally, as previously mentioned, there is no clear conscious sensation of the vestibular endorgans. This makes it often difficult for patients to understand and describe their symptoms and, consequently, clinicians face confusing anamnesis.
Vestibular testing
Despite significant progress in vestibular testing, it remains a clinical challenge to assess and quantify the vestibular function in its entirety. We still mostly rely on the evaluation of vestibular reflexes (i.e. VOR measurement to a variety of stimuli for canal function and vestibular evoked myogenic potentials recording for otholithic function). However, various other diagnostic approaches are being explored. Assessment of multisensory tasks such as visual acuity in dynamic conditions (i.e. while walking or during unpredictable passive head movements) is a sensitive test of the integration of vestibular input into the balance system [24, 65]. The measurement of motion perception thresholds is another strategy to assess the functionality of the vestibular system with a long history in vestibular research. Significant progress and interesting results have been achieved with these tests [53], and some experts in the field envision them to soon become part of the standard vestibular testing battery. However significant remaining drawbacks of the method are the necessary heavy and expensive equipment (i.e. hexapod), the duration of the test (many hours) and the fact that it is not possible to completely rule out the effect of somatosensory cues. Posturography has also been extensively studied and is used by many clinicians. However, a group of experts in the field recently concluded that there is no generally applicable posturography test providing reasonable sensitivity and specificity for the diagnosis of balance disorders currently available [34]. They also concluded that perturbation techniques are most likely needed to enhance the diagnostic yield of this technique.
In summary, significant challenges still need to be overcome in the field of vestibular testing and evaluation. In addition, the quantification of the “artificial” vestibular information provided by a vestibular implant is a recent endeavor. This is why one of the main challenges in the vestibular implant field will be the development of meaningful tests to objectively determine its clinical benefit. In this paper we attempt to summarize the milestones of our group in this direction.
Methods
The concept of the vestibular implant
The concept is similar to that of the cochlear implant except that instead of sound, motion information is captured using head-fixed sensors and fed to a special processor [50] where it is converted into an appropriate neural pattern. This pattern is is in then transmitted to the implanted stimulator via telemetry. The stimulator consists of a modified cochlear implant with 1 to 3 “vestibular” electrodes taken out of the cochlear electrode array and put into separate branches designed to be positioned closely to the ampullary branches of the vestibular nerve (Fig. 1). Finally, the neural patterns of processed motion information are provided to the central nervous system in the form of electrical currents delivered via the vestibular electrodes.
In this concept, the vestibular implant aims at transmitting “artificial” neural patterns to the central nervous system similar to those coded by the normally functioning vestibular system. In a healthy subject, the vestibular nerves fire spontaneously at a rate of about 90 action potentials/s in the absence of movement [19]. Motion is then coded by the modulation of this spontaneous firing rate. For example, for the horizontal semicircular canal a head rotation in the direction of the canal (i.e., rightwards for the right ear and leftwards for the left ear) will result in an increase of the firing rate. Conversely, a horizontal head rotation in a direction opposite to the canal (i.e., leftwards for the right ear and rightwards for the left ear) will result in a decrease of the firing rate. This motion-controlled modulation of the spontaneous firing rate results in a compensatory horizontal eye movement in the direction opposite to the head movement. Therefore, in patients with a bilateral loss of the vestibular function, a prerequisite to reestablish bi-directional eye movements with unilateral electrical stimulation is to restore an artificial “spontaneous” firing rate so that it can be increased (up-modulated) for generating eye movements in one direction and decreased (down-modulated) for generating eye movements in the opposite direction.

A multichannel version of the vestibular implant prototype, consisting in a modified cochlear implant (Medel, Innsbruck, Austria) with 3 vestibular electrodes to be implanted in the 3 semicircular canals close to the corresponding ampullary nerves and the main array with cochlear electrodes.
A fundamental step was the development of appropriate surgical techniques to allow for stable and safe implantation of electrodes in the vicinity of the vestibular nerve branches. However, this surgical access presents significant risk of inducing hearing loss [20]. As the majority of BVL patients has a normal or residual hearing, hearing preservation represents a major issue. Therefore, an extralabyrinthine surgical approach was initially developed based on the known surgical approach to the posterior ampullary nerve developed by Gacek who showed results with a high rate of hearing preservation (>95%) [17]. A first series of 100 temporal bones were dissected, showing a procedure success rate of 98% in accessing the posterior ampullary nerve [14, 35]. The need to elicit eye movements in other “orthogonal” directions led to the development of similar extralabyrinthine surgical approaches to the superior and lateral ampullary nerves. In a second series of 80 temporal bones, both structures could be reached in 71 temporal bones. Nevertheless, in most of the cases (64/71) the ampulla was opened [15]. All the above mentioned approaches are transmeatal (through the external auditory canal) and can be done in local anesthesia which allowed acute intra-operative testing in the awake patient which was essential to demonstrate the feasibility of the project.
As already mentioned, the extralabyrinthine approaches were thought to be safer and were initially favored. Nevertheless, all the promising results reported by research groups working in the same field on animals were obtained by using more classical intralabyrinthine approaches [11, 38]. Therefore, our group also developed an intralabyrinthine surgical approach [62]. A mastoidectomy is performed, each semicircular canal is exposed and a micrometric labyrinthotomy close to the ampulla is performed. While a certain degree of hearing and vestibular function preservation was obtained in animal experiments after intralabyrinthine electrode insertion, this could not be confirmed in human experiments [4, 61]. Therefore, the risk of impairing hearing by using an intralabyrinthine approach remains unknown. Nevertheless, promisingly, it has been shown that it is possible to preserve hearing during canal plugging, which is a similar surgical procedure performed for intractable benign paroxysmal positional vertigo or for severe Menière’s disease [1, 41].
Ethical considerations
All experiments were designed and conducted in accordance with the 1964 Declaration of Helsinki. Local ethical committees of the Geneva University Hospitals (NAC 11-080) and of the Maastricht University Medical Centre (NL36777.068.11/METC 11-2-031) approved this experimental protocol. All participants gave their informed consent prior their inclusion in the study.
Results
Acute intra-operative stimulation trials
After having developed the surgical routes to reach the ampullary branches of the vestibular nerve, the first step was to show that vestibular responses could be elicited in human patients in acute stimulation trials during surgeries where the vestibular nerves were accessible. To do this, 3 deaf patients, candidates to a cochlear implantation, were selected. Two patients had a bilateral Menière’s disease and one patient had a concomitant unilateral vestibular loss. In all 3 cases, the posterior ampullary nerve was accessed (extralabyrinthine approach) in local anesthesia. An electrode was positioned in its contact and maintained manually in place to allow for acute electrical stimulation. Robust nystagmic responses reflecting the activation of the vestibular system were elicited and were recorded using a standard 2D video-oculography system. Those nystagmic responses showed a threshold effect and were predominantly in the vertical plane. For a given pulse rate, a monotonic, fairly linear correlation between current amplitude (μA) and slow phase velocity of the nystagmus was found. In a second stage, current amplitude was kept constant and its pulse rate was progressively increased. The observed nystagmic responses also showed a threshold effect. The amplitude of the nystagmus slow phase velocity showed an almost linear rise with a peak at an “optimal” pulse rate followed by a progressive decline.
During the acute stimulation trials, the patients described a feeling of surprise, then a sensation of rotatory motion without nausea or motion sickness. At the end of the experimental procedure, general anesthesia was induced and a regular cochlear implantation was performed [66].
A similar procedure targeting the lateral and superior ampullary branches of the vestibular nerve (extralabyrinthine) was done in three patients with unilateral intractable Menière’s disease prior to a transmeatal labyrinthectomy. Hearing was non serviceable in the operated ears. The recorded nystagmic responses were predominantly in the horizontal plane without concomitant stimulation of the facial nerve [28].
Using the intralabyrinthine surgical approach described by van de Berg et al. [62], the first acute intra-operative intralabyrinthine electrical stimulation trials of the different ampullary branches of the vestibular nerve were performed in 3 deaf patients with a bilateral vestibular loss prior to cochlear implantation [62]. Note that the procedure was performed under general anesthesia which is known to impair nystagmic responses, especially the fast phase of the VOR [5, 47]. Particularly propofol (2,6-diisopropylphénol), a short acting hypnotic agent used to induce and maintain general anesthesia, has been shown to decrease significantly the vestibular nuclei activity in rats [6]. Therefore, prior to electric stimulation trials, propofol was stopped and anesthesia was maintained with remiphentanil, a short-acting synthetic opioid, similar to fentanyl. As fentanyl selectively suppresses the fast phase of the nystagmic response [31], only the slow phases of the VOR could be electrically elicited, resulting in a tonic deviation of the eyes. The observed tonic deviations were predominantly in the plane of the stimulated semicircular canal. As the electric stimulation was stopped, the eyes returned to the neutral position, presumably driven by elastic restoring forces of the eyeball. No complications were reported in the follow up.
Chronic implantations and adaptation to electrical stimulation of the vestibular system in humans
The first implantation of a vestibular implant prototype in a human was performed in Geneva in 2007. The patient suffered from bilateral deafness and concomitant idiopathic bilateral vestibular loss. This first vestibular implant prototype incorporated only one vestibular electrode together with the cochlear array. The posterior ampullary nerve could not be visually identified during surgery, but the vestibular electrode was positioned in its vicinity according to the known landmarks. As the surgery was done in general anesthesia, no attempt of generating vestibular responses upon intra-operative stimulation trials was made. Postoperative electrical stimulation delivered via the vestibular electrode elicited robust nystagmic responses with a dominant horizontal component, indicating a possible current spread to other branches of the vestibular nerve. During stimulation, the patient reported a high frequency sound and a sensation of dizziness, both of which increased with increasing current intensity.
Since the concept of the vestibular implant is to mimic the physiology of the vestibular system, the next step consisted of attempting to restore an “artificial” baseline or “rest” activity in the vestibular nerve. After approximately 27 minutes of constant electrical stimulation the nystagmic responses induced at the sudden onset of stimulation almost completely vanished. This was the first demonstration of adaptation to constant electrical stimulation of the vestibular nerve in a human subject. Moreover a reversed nystagmic response, lasting less than 10 minutes, was observed when the stimulation was suddenly turned off. After several repetitions of such on/off stimulation sequences, the adaptation time required for nystagmic responses to disappear fell down to less than 5 minutes. This ”adaptation” lasted close to 24 hours after the device has been turned off [23] and was much faster than what had been reported in similar animal experiments [44]. These findings had crucial implications for the clinical application of the concept, significantly reducing concerns that a vestibular implant had to be permanently activated to avoid long-lasting adverse symptoms when turning the device on or off. Finally, another fundamental finding was the demonstration of the ability to generate smooth, controlled eye movements by up- and down- modulating the baseline stimulation using a virtual motion sinusoidal profile. Although both amplitude and frequency modulation were effective, larger responses were recorded with amplitude modulation [29].
Since this first-of-its-kind experiment performed in 2007, a group of 12 additional patients (i.e., 13 successful implantations in total) have been implanted with 3 incremental generations of vestibular implant prototypes incorporating 1, 2, or 3 vestibular electrodes (see Table 1). All patients suffered from severe bilateral vestibular loss and were deaf on the implanted ear (details on the inclusion criteria can be found in [51]). Diverse etiologies and different deficit durations were deliberately chosen in order to assess efficacy in a wide patient population. To date, we have no surgical complications or adverse events related to the implantations to report. All details regarding implantations and results obtained with the 11 first implanted patients have been recently reported [25].
Demographic details and implantation characteristics of the implanted patients
Demographic details and implantation characteristics of the implanted patients
*PAN – posterior ampullary nerve; LAN – lateral ampullary nerve; SAN – superior ampullary nerve. •EL – extralabyrinthic; IL – intralabyrinthic.
The VOR can be considered a very useful window to the functionality of the peripheral vestibular endorgans. Although it only represents a single aspect of the vestibular function, it is the most accessible method to its quantitative assessment. Therefore, most preliminary work on vestibular implants, including ours, initally focused on the VOR to establish feasibility.
In 3 vestibular implant recipients, the VOR resulting from motion modulated electrical stimulation via the electrode positoned in ampulla of the lateral canal was assessed [51]. Patients were rotated around an earth vertical axis using a rotatory chair in complete darkness. The rotation profiles of the rotatory chair were of sinusoidal form, with a peak velocity of 30 °/s and frequencies ranging from 0.1 Hz up to 2 Hz. The VOR was measured using a 2D video eye-tracker in two conditions: (1) when the device was turned on (system ON) and (2) when the device was not activated (system OFF). With the system ON, the VOR gain significantly increased at rotation frequencies of 0.5, 1 and 2 Hz, but not at the lower frequencies of 0.1 and 0.25 Hz. This frequency-dependency of the “artificial” VOR was similar to that observed in a group of normal controls [63]. Increasing the modulation depth (i.e., stimulation intensity) up to 75% of the available dynamic range further increased the VOR gain. In the best case, the “artificial” VOR was practically normalized (see example in Fig. 2). Although these experiments were carried out in only a small number of patients and were limited for a small range of motion profiles, these results represented a fundamental milestone, being the first demonstration of functional rehabilitation of the vestibular system with a vestibular implant prototype.

Patient with a bilateral vestibular loss, fitted with a vestibular implant prototype, rotating around an earth vertical axis (f = 1 Hz, ωmax = 30°/s). A: “system off”, B: “system on” (motion modulated stimulation via the electrode positioned close to the lateral ampullary nerve).
The functional implications of the “artificial” restoration of the VOR were additionally measured using visual acuity measurements during electrical stimulation of the posterior or the superior ampullary nerves with a virtual sinusoidal motion profile. In other words, in these experiments the patients were sitting static on a chair while the vestibular implant was activated. In this condition, we observed pathological decreases of visual acuity of similar magnitude to dynamic visual acuity drops reported for patients with bilateral vestibular loss [27]. Deteriorating visual acuity is obviously not the goal of the vestibular implant, but this result is important since it demonstrates that the “artificial” VOR can significantly impact visual acuity. Therefore, if the “artificial” VOR is appropriately fine-tuned, it could provide useful motion information to improve visual performance in simple, everyday dynamic tasks such as during walking. This was further corroborated in pilot measurements of dynamic visual acuity with the vestibular implant prototype, where results clearly showed that the performance of implanted patients became close to normal when coherent motion information was delivered by the device [26].
Substantial efforts have been devoted to vestibular implant research in animal models. In particular, innovative psychophysical methods have been developed in order to assess vestibular percepts beyond the VOR (e.g., tilt and head perception perception in primates [37, 40]). However, these assessments remain limited in animals, especially because subjective descriptions cannot be obtained from them for obvious reasons. Therefore, research in human patients fitted with a vestibular implant represents a unique opportunity to bring the exploration of the vestibular system to another level.
In a recent paper, the percepts elicited by electrical stimulation of the ampullary branches of the vestibular nerve in 11 patients fitted with a vestibular implant were reported [25]. Only a few electrodes elicited motion percepts, despite the fact that it would have been the most intuitive guess. In the meantime, two additional patients have been implanted. One suffered a bilateral vestibular loss following trauma with bilateral intraotic temporal bone fractures (BVL12 in Table 1). This patient in particular is a clever physicist who understands very well the ongoing experiments and provides very precise descriptions of the effects of electrical stimulation. For example, as the current amplitude of the stimulus delivered to the superior ampullary nerve was gradually increased (25–50μA increments, stimulation profile identical to previous reports [25, 51]), he described: “I have never experienced something like this before, I can feel it is there but I cannot explain exactly, I can say it is like a frequency, 20 Hz, but I cannot say this is it. The closest I can get, is in fact, if you suddenly remember something you have forgotten.” ... However, as soon as a cochlear electrode was activated he described: “I can hear, it is a sound!” He was then asked if the sensation he experienced during activation of the “vestibular” electrode had anything to do with sound, he replied without ambiguity: “no it was not a sound!” Given all these unexpected descriptions, it could be questioned whether vestibular nerves had really been activated in our implanted patients. However, the placement of electrodes under visual control using known surgical approaches, the radiologic control of the electrode position, and the presence of a VOR during electrode activation are all strong arguments in favor of activation of the vestibular system.
Additional evidence of activation of the vestibular system using our vestibular implant prototypes could be obtained by activation of the vestibulo-collic reflex demonstrated by the recording of cervical vestibular evoked myogenic potentials (cVEMPs). Cervical VEMPs are thought to reflect the functionality of the saccular part of the otolithic organ [54]. Few groups reported successful measurements of cVEMPs elicited by electrical stimulation of the promontory in local anesthesia prior cochlear implantation [48] or by direct electrical stimulation of the inferior vestibular nerve in patients undergoing a surgery of the cerebello-pontine angle in general anesthesia [3]. In this second study there were no recordable cVEMPs when stimulating the superior vestibular nerve, which is in accordance with its probable saccular origin. In a recent pilot study conducted in 5 implanted patients, cVEMPs with its classical characteristics could be successfully elicited (see example in Fig. 3) using a standard recording protocol, except for the stimulus, which consisted of 100 trials of single, cathodic-first, biphasic, and charge balanced pulses delivered at a rate of 5 pulses per second via the electrodes positioned in the lateral or the superior canals (intralabyrinthine). P1 and N1 latencies were in average 9.8 s (±1.0 s) and 16.9 s (±1.7 s), respectively. These findings indicate that it is possible to artificially restore the vetibulo-collic reflex in a patient with a complete bilateral vestibular loss and thus that useful motion information could potentially be delivered via the vestibulo-spinal pathways.
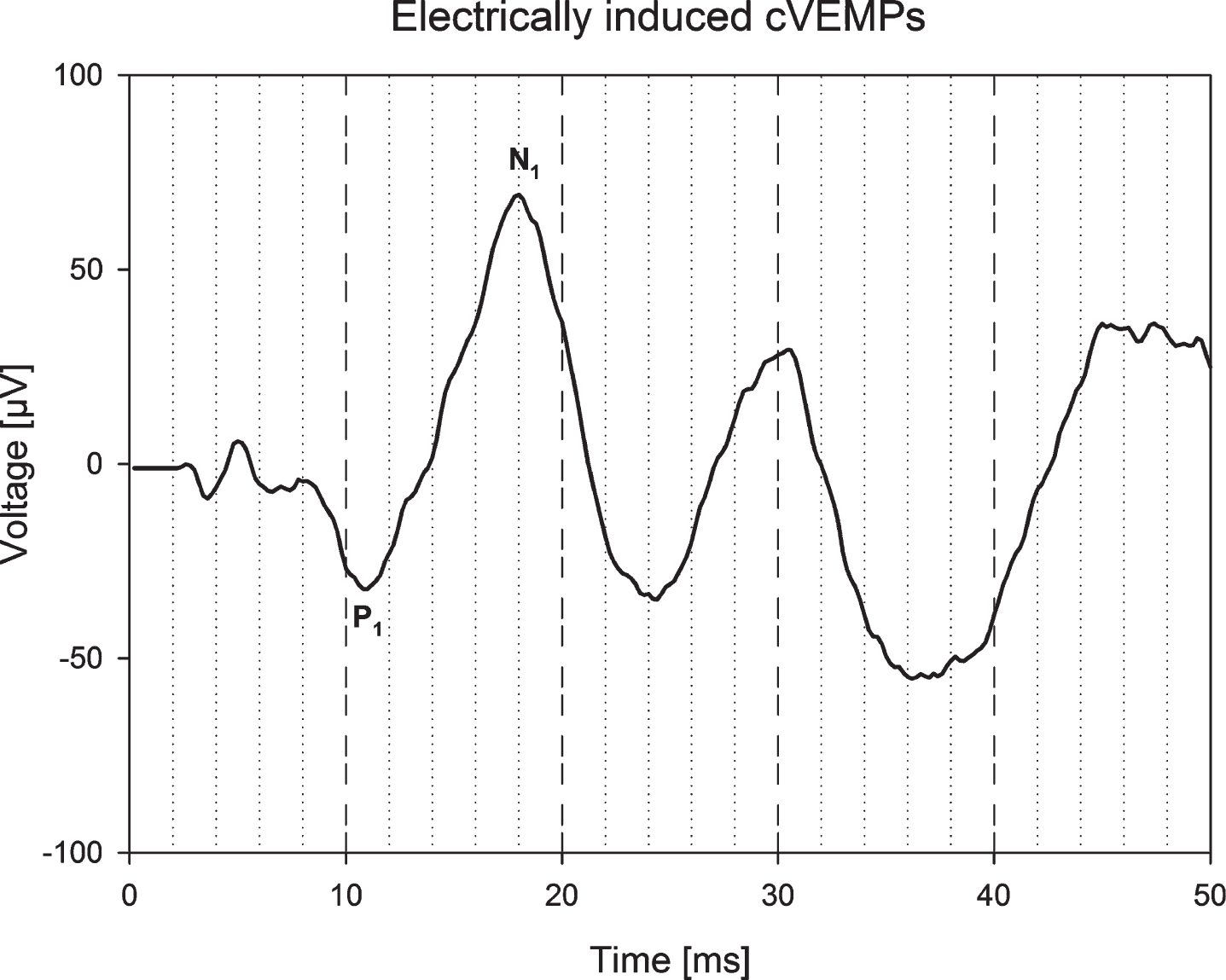
Morphology of cVEMPs recorded according to a standard protocol, except for the stimulus, which consisted of 100 trials of single cathodic first, biphasic, charge balanced pulses delivered at a rate of 5 pulses per second by the vestibular implant electrode positioned in the superior canal.
The Geneva-Maastricht team is the first (and practically the only one) to work with human patients fitted with a vestibular implant aimed at restoring vestibular function in cases of bilateral vestibular loss. Within the last 10 years, 13 patients have received single- and multi-channel vestibular implant prototypes. No medical complication has been observed. It is worth mentioning that, except for one patient who has normal hearing on the controlateral ear, all patients benefit fully from their cochlear implant and are fully satisfied with the device.
We have demonstrated that vestibular reflexes can be at least partially restored using a vestibular implant prototype. Besides the extensively studied VOR, here we show that the vestibulo-collic reflex can also be successfully activated. Average latencies of the cVEMPs response were however substantially shorter than those classically described with acoustic stimuli (P1 = 13 ms/N1 = 23 ms). Similar short latency cVEMP responses have been recently reported using electrical stimuli delivered with cochlear implants [49]. These results could be explained by the fact that electrical stimulation directly activates the vestibular afferents, thus bypassing the mechanoelectrical transduction. However, the precise origin of these responses (canal afferents, otolithic afferents or a combination of both) still remains unclear. Finally, in order to evaluate whether the restoration of vestibular reflexes could be useful in a task representative of every-day difficulties faced by patients, we implemented a simple dynamic visual acuity protocol that could be performed with and without activation of the vestibular implant [24]. The pilot results are striking, demonstrating that the implant significantly improves the ability to stabilize gaze in a dynamic condition such as walking. Altogether, these results represent a major step towards a useful device potentially addressing several major complaints of patients suffering with a bilateral vestibular loss (e.g., oscillopsia, postural control) and open the door for a clinical application in the near future.
Another research team reported results obtained in patients implanted with a modified cochlear implant with a trifurcating array incorporating 3 electrodes per array inserted into the ampullas [20, 52]. Their device was purely vestibular and did not have any cochlear electrodes. Their initial concept was also different from ours: their vestibular device was concieved to act as a pace maker that could be activated during a Menière’s crisis to regulate vestibular function in patients suffering from intractable Menière’s disease. Only one patient experienced a typical Menière’s crisis after implantation. In this case, activation of the device led to a subjective improvement. Although this result is promising, the fact that no other Menière’s crisis has been reported after implantation is compatible with the loss of the vestibular function observed after implantation in all 4 of them. Moreover the pre-operative residual hearing could not be preserved either in any of the 4 subjects participating in this study. Despite this negative results, in can not be ruled out that the principle of a specific vestibular pacemeker developed to control the fluctuation of the vestibular function in patients suffering handicapping Menière’s disease, can still be a potential therapeutic application of the principle of electrical stimulation of the vestibular nerve.
Future work
As preservation of the vestibular and hearing function will be a crucial issue, substantial efforts are put into the design of new electrodes and surgical approaches to allow atraumatic implantation with preservation of the membraneous labyrinth. Particular attention is put into increasing the specificity of stimulation by optimally targetting the different branches of the vestibular nerve, inculding the saccular and utricular branches. Indeed canal and otolithic function are complementary and rehabilitation of both functions could be necessary to reach a higher level of functional rehabilitation.
The other main area of interest is improving and extending the rehabilitation prospects of the device, particularly regarding imbalance and postural control. Finally, in parallel to this fundamental clinical developments our current and future research will also be devoted to gathering fundamental knowledge on the vestibular system and its interactions with extra-vestibular mechanisms. Indeed, the vestibular implant offers the unique opportunity to selectively deliver a vestibular stimulus to the central nervous system. This opens an unprecedented door for the study of the integration and perception of vestibular input in the multisensory, multimodal system of balance.