
Abstract
Introduction
Cerebellopontine angle (CPA) is an anatomical region of a complex interaction between vascular and neural structures. This region covers three fissures,the cerebellomesencephalic, cerebellopontine, and cerebellomedullary fissures, which are located at the superior, medial, and inferior positions, respectively. The corresponding vasculature in these fissures are the superior cerebellar artery and cerebellomesencephalic vein, the anterior inferior cerebellar artery (AICA), the cerebellopontine fissure vein, and the posterior inferior cerebellar artery (PICA) and cerebellomedullary fissure vein. The vestibulocochlear nerve (VCN) enters the region beneath the cerebella floccules [19]. This cranial nerve is accompanied primarily by AICA en route [11], which may originate from basilar (98.1%) or vertebral (1.9%) arteries as a single (92.3%) or duplicate (7.7%) branch [8]. The disturbances in close localization of these anatomical structures sometimes yield to some clinical situations, which can be grouped under the term “vascular compression syndrome.” This term refers to diseases caused by direct contact of a vessel with a cranial nerve stem [9]. Vascular compression syndrome associated with the VCN is mostly caused by the AICA [10]. This syndrome may clinically present as vertigo, tinnitus, and hearing loss [6, 20], and it may be screened by abnormal results in neuro-otologictests [18].
Because the aforementioned syndromes are primarily consequences of anatomical aberrations, imaging of the CPA is highly valuable in diagnosing the etiology of this group of diseases. Magnetic resonance imaging (MRI) is a widely-used technique for visualizing the internal auditory canal (IAC) and the CPA in patients with auditory symptoms [7]. This technique provides critical clues about the anatomical relationships between VCN and surrounding vasculature in the temporal bone [19], which substantially contributes to the diagnoses of these patients.
The aim of the present study was to elucidate the clinical relationship of vertigo symptoms with vascular loop compression syndrome by evaluating the neurovascular contacts of VCN and AICA at the CPA and IAC via high-resolution MRI.
Materials and methods
Patients
The present study included 417 patients who underwent MRI for various clinical causes. The images were evaluated regarding the relationships of VCN with AICA and PICA at the CPA and IAC. A high-resolution 3-dimensional (3D) T2-weighted (T2W) MRI device was used for the MRI scans, and the images were assessed by an experienced radiologist specialized in head and neck radiology. The vascular loops were classified according to the coursing patterns of the AICA and PICA and their relationships with the VCN as: 1) Type 1: vascular loop at the CPA level, 2) Type 2: vascular loop proximal to the IAC, 3) Type 3: vascular loop distal to the IAC, 4) Type A: contact with the VCN, 5) Type B: indentation to the VCN. Type 1 is schematized in Fig. 1.

Display of vascular loop type 1–3 with a scheme.
The patients were assigned into two study groups according to the presence/absence of vertigo. Patients who were admitted with the complaint of dizziness and those in whom diagnosis of benign paroxysmal positional vertigo (BPPV) was excluded were classified as having vertigo. Demographic and clinical findings were compared between these groups.
A 32-channel head coil was used for 1.5 T scanners (Siemens Magnetom Aera, Germany). Pre-contrast technical parameters were as follows: a repetition time (TR) of 400 ms, echo time (TE) of 8.6 ms, a field of view (FOV) of 256×320 mm, a FOV phase of 100, a slice thickness of 3 mm, a NEX of 1 for T1-weighted images; a TR of 3,820 ms, a TE of 96 ms, a FOV of 256×320 mm, a FOV phase of 100, a slice thickness of 3 mm, a NEX of 2 for T2 images; and a TR of 1,000 ms, a TE of 266 ms, a FOV of 180×230 mm, a FOV phase of 80, a slice thickness of 0.7 mm, and a NEX of 1.4 for 3D Turbo spin echo T2 images (t2 spc-tra-p2 iso-0.6).
After 0.1 mmol/kg of IV contrast injection, the technical parameters were as follows: a TR of 400 ms, a TE of 8.6 ms, a FOV of 240×320 mm, a FOV phase of 100, a slice thickness of 3 mm, and a NEX of 3 for T1 axial images and a TR of 471 ms, a TE of 12 ms, a FOV of 224×320 mm, a FOV phase of 100, a slice thickness of 3 mm, and a NEX of 3 for T1 coronal images.
Statistical analysis
Descriptive statistics were presented as mean and standard deviation for numerical variables and as frequency for categorical variables. Student’st-test and chi-square test were used for comparisons between independent groups of numerical variables and categorical variables, respectively. A statistical significance level of 5% was determined as a Type-I error limit in the study. All statistical analyses were performed two-sided using the Predictive Analytics Software (PASW) Statistics version 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
The present study included 417 patients with a mean age of 45.5±18.6 years, of whom 182 (43.6%) were males and 235 (56.4%) were females. Of the patients, 178 (42.7%) had vertigo symptoms. The demographic characteristics of the study groups are presented in Table 1. The mean age of the patients with and without vertigo were 50.1±17.3 years and 42.1±18.9 years, respectively, and there was a significant difference between the age distributions of the study groups (p < 0.001). The gender distribution also significantly differed between the study groups (p = 0.003).
Demographic characteristics of the study groups
Demographic characteristics of the study groups
SD, standard deviation.
The distribution of MRI findings in the entire group and in the patients with and without vertigo is presented in Table 2. According to these findings, for the right side, the most frequent localization of the vascular loop was at the CPA level (Type 1, 37.9%), and there was a contact with the VCN (Type A) in 61.4% of the patients. For the left side, Type 1 vascular loops were observed in 38.4% of the patients and Type A vascular loops were observed in 61.2% of the patients. Comparisons of the patients with and without vertigo revealed no significant difference in terms of MRI findings (p > 0.05 for all parameters). The MRI images for the patients with vertigo according to the vascular loop classification are demonstrated in Figs. 2–5.
Magnetic resonance imaging findings in the entire group and in the patients with and without vertigo
*Cases where the vascular structure is not at the same section with the nerves.
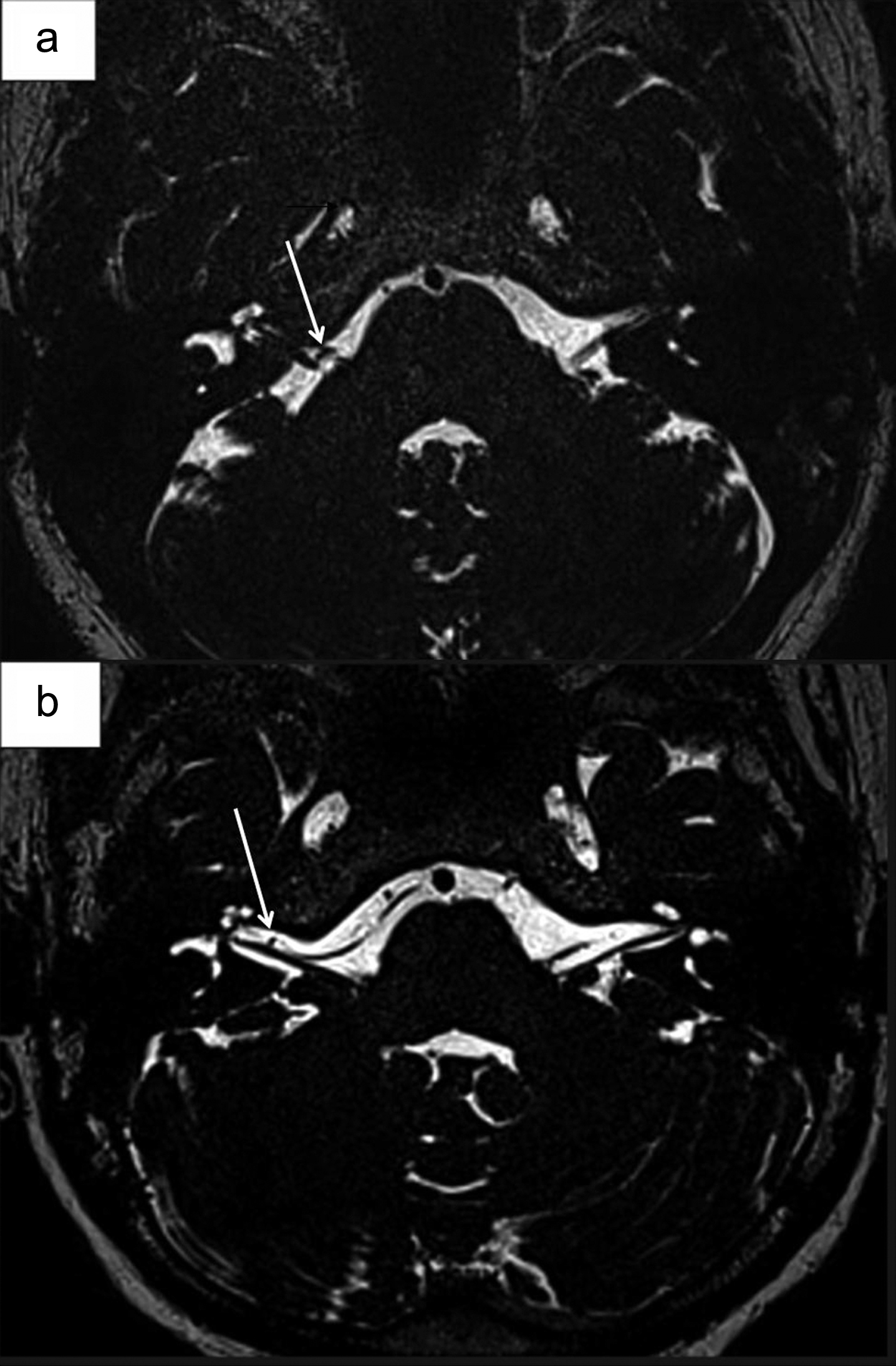
Magnetic resonance images of a) right-sided type 1A in a 47-year-old patient with vertigo and b) right-sided type 2A in a 28-year-old patient with vertigo.
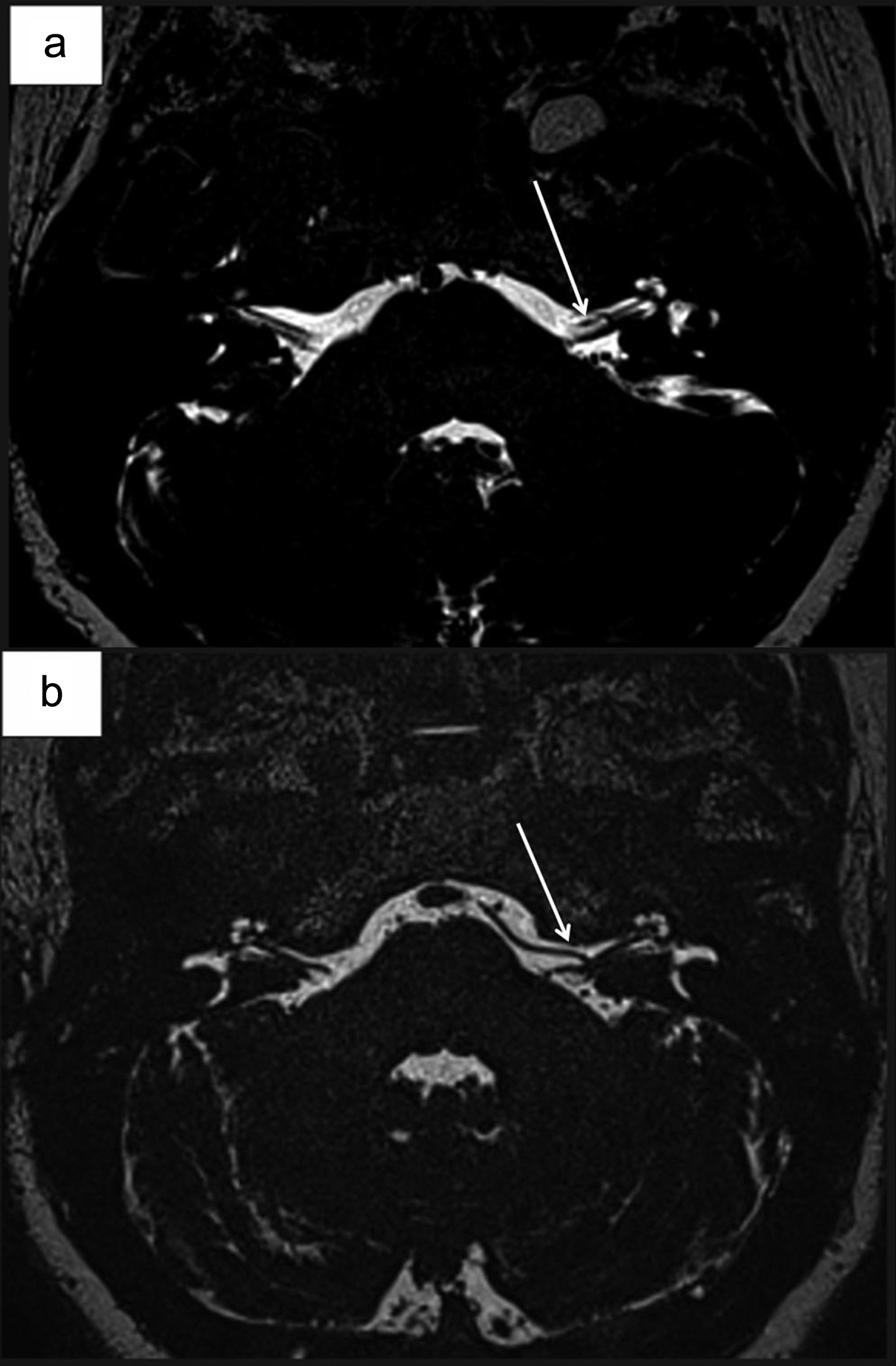
Magnetic resonance images of a) left-sided type 2A in a 40-year-old patient with vertigo and b) left-sided type 2B in a 46-year-old patient with vertigo.
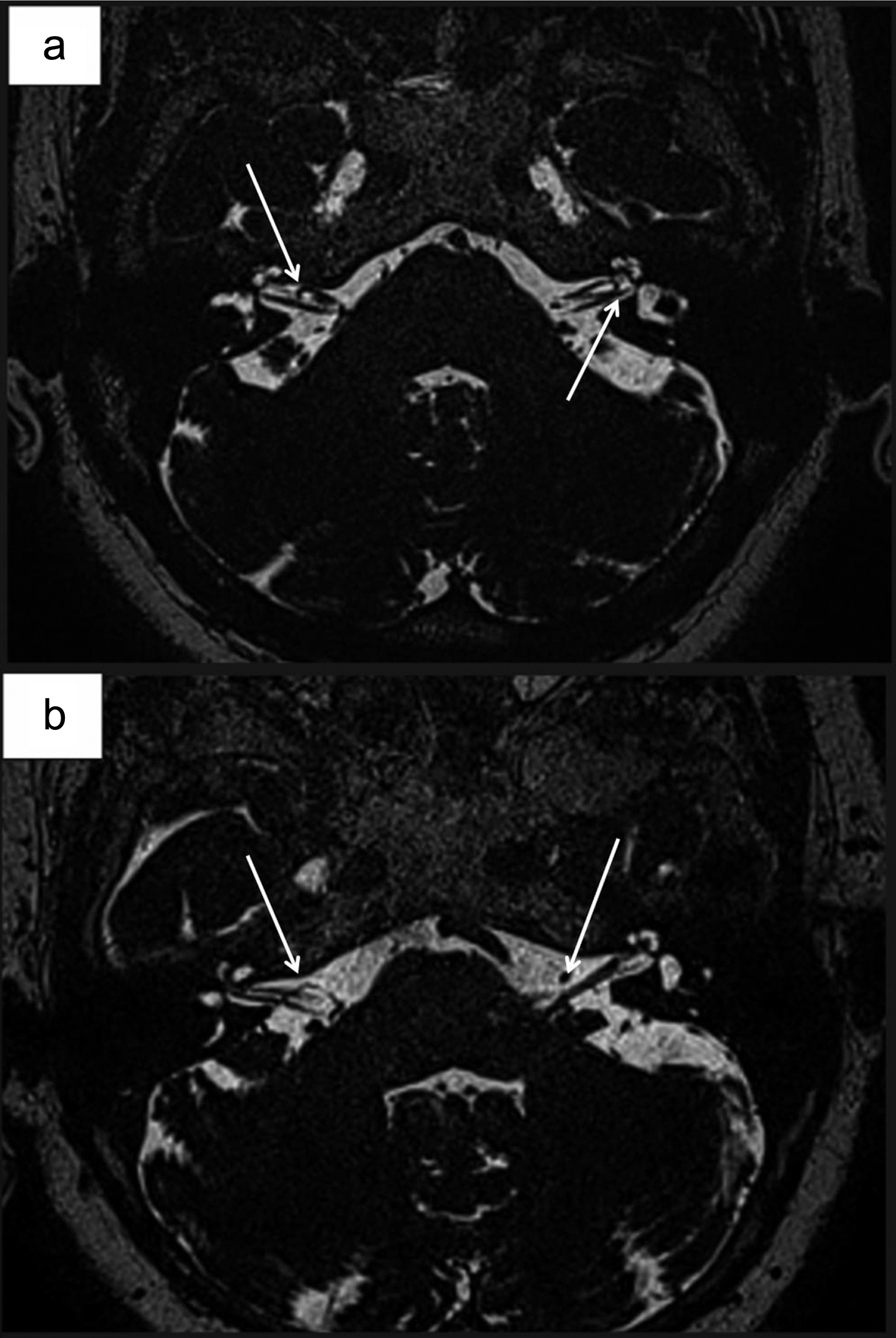
Magnetic resonance images of a) right-sided type 2A and left-sided type 3A in a 48-year-old patient with vertigo and b) right-sided type 2A and left-sided type 1A in a 75-year-old patient with vertigo.
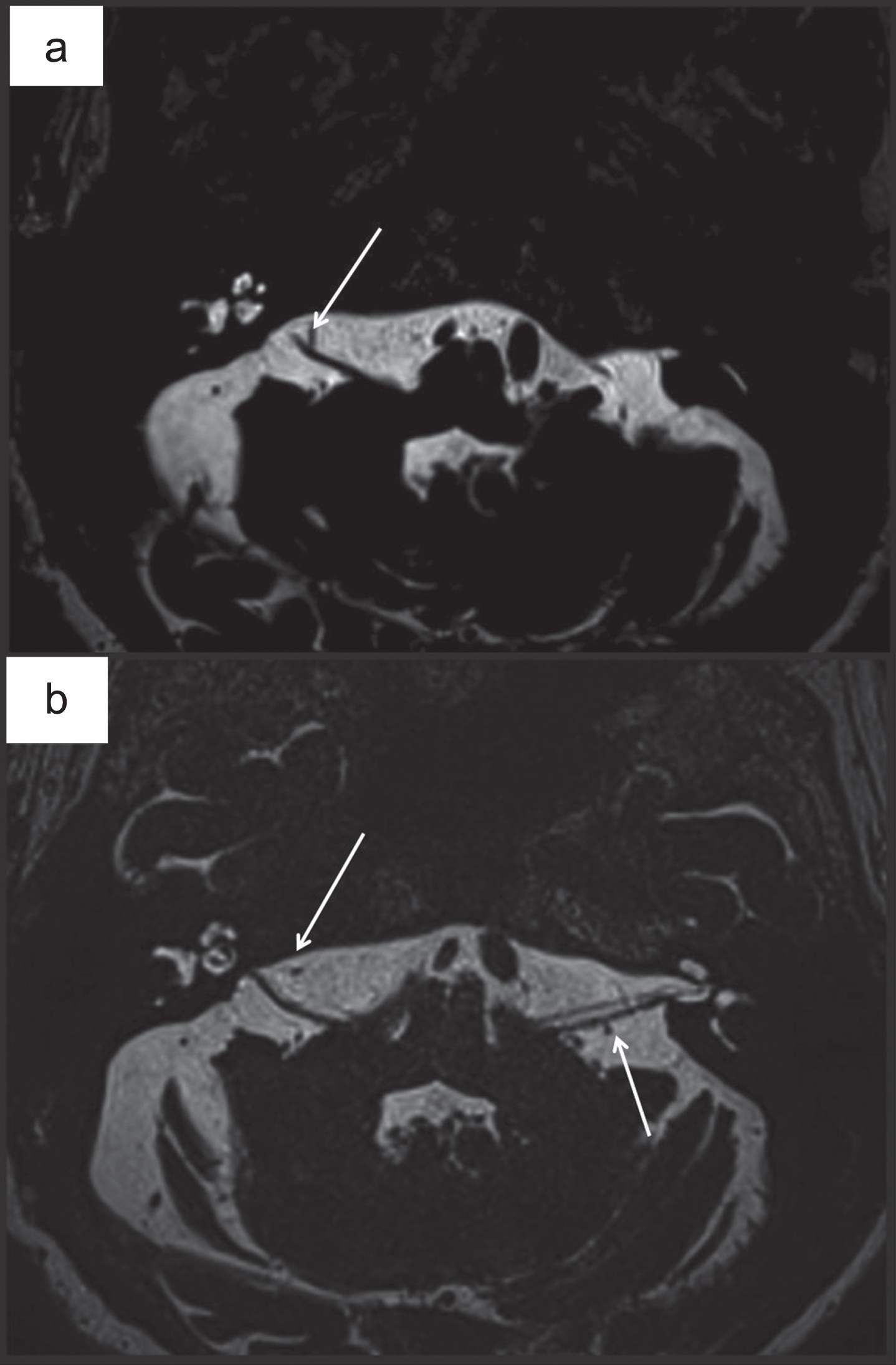
Magnetic resonance images of a) right-sided type 1B in a 62-year-old patient with vertigo and b) right-sided type 1B, left-sided type 1A arch in a 62-year-old patient with vertigo.
Current literature data suggests that microvascular compression of the VCN may result in vertigo, tinnitus, and hearing loss [21]. The most common anatomical structures that cause compression of the VCN are AICA, PICA, and/or their branches [1, 8]. Previous reports about the vascular cross-compression of the VCN, particularly by AICA, have indicated that symptoms other than vertigo in these cases might include continuous disequilibrium and motion intolerance [18]. Additionally, some authors have suggested that audiovestibular symptoms could be observed not only by direct contact of the vascular structures to the VCN but also due to pulsation of the relevant artery that is in contact with the VCN [19]. In fact, there is a debate in the literature about the exact explanation of neuro-otologic symptoms in cases with vascular compression of the VCN. Because some studies have reported that vascular loops may be present at birth [3], this leads to confusion about whether vascular compression is the etiological factor in vertigo-like symptoms or it is only an incidental finding in these cases [19].
The answer to this debate is unclear. Whereas some studies have reported that there is no association between vascular loops of the AICA and patient symptoms [4, 18], some authors have reported that unilateral hearing loss is significantly related to the presence of AICA loops in their series [12, 13]. Moreover, some studies have argued that aging is another important factor in this debate because aging can contribute to stiffness of the arterial walls, which eventually increases the pressure on nerve structures, and aging can cause stretched nerves due to decreased cerebrospinal fluid and cerebral atrophy, leading these nerves to make contact with arteries due to stretching [19]. Similarly, in our cases, the mean age of the patients with vertigo symptoms was higher than that of those without symptoms. This might be interpreted to mean that aging can be associated with increased severity of symptoms, which is a plausible explanation consistent with the suggestions of earlier studies. On the other hand, it might also be interpreted to mean that vertigo develops in advanced age groups; however, younger patients might have more early-symptoms prior to development of vertigo, which should be evaluated by MRI scans, as in our cases.
When the epidemiological data about the prevalence of vascular loops of the AICA are researched in the literature, widely varying facts and figures can be found. The major cause of this wide range of numbers is the modality used to determine the vascular aberrations of the AICA in the IAC and CPA. Radiological studies have reported the prevalence of vascular compression of the VCN between 21% and 50% [4, 14], anatomical studies on cadavers have reported the prevalence of vascular loops in the AICA as 12.3% [16], and pneumatic computerized tomography (CT) cisternography of patients with auditory-vestibular symptoms have revealed a vascular compression rate of 30% [6]. In the present study, we identified Type 1 vascular loops in almost 40% of our patients, and we observed direct contact of the VCN and vascular structures in more than 60% of the cases. These rates were relatively higher than those found in the literature, which might be related to the performance of the high-resolution 3D T2W MRI device.
The 3D turbo spin-echo is a variant of the turbo spin-echo sequence that allows extremely large turbo factors greater than 100. The stimulated echoes require longer effective TEs to be used for a similar contrast as with a conventional T2-weighted turbo spin echo sequence. Therefore, a TE of approximately 350 ms should be seen in the context of this variable flip angle design, which means that the sequence behaves like a conventional T2-weighted turbo spin-echo sequence setup with a TE of approximately 100 ms.
During the last decades, MRI has been the preferred imaging method for the diagnosis of vascular compression syndrome in patients with auditory-vestibular symptoms due to its high sensitivity and specificity rates [2, 4]. In fact, CT and MRI scans are complementary to each other for evaluating the CPA. MRI can also visualize leptomeningeal disease more accurately, whereas CT optimally defines associated bone changes [17]. A previous study on MRI evaluation of the IAC for determining the AICA loops in patients with tinnitus reported that all patients with tinnitus and only 5% of asymptomatic controls had AICA loops [15]. In another study conducted on 100 patients undergoing surgery for hemi-facial spasm, it was reported that the false negative rate of MRI in predicting the pathology was only 1/100 [5]. These studies show that recent improvements in imaging techniques have made visualization of complex neurovascular interactions in the CPA and IAC possible [4]. Nevertheless, despite the high accuracy of MRI for vascular-neural structures, physicians should keep the high anatomical variability of this anatomical region in mind.
The present study included patients who had any ear problems, including tinnitus, hearing loss, etc., even if they did not have vertigo symptoms. We did not identify a significant difference in terms of variations at the CPA. One of the possible explanations of this insignificance might be the presence of auditory disturbance of any kind in our patients. Thus, these findings should be confirmed in studies that also include control groups without any kind of auditory disturbance. Nevertheless, it should be noted that, to the best of our knowledge, the present study is a large-scale study relative to the other studies in the same category in the literature.
The most important factor restricting the effectiveness of our study is the lack of evaluation of whether there is a relationship between the differential diagnosis (such as Meniere’s disease, vestibular neurinitis, vertebrobasilar insufficiency, etc.) of these patients with vertigo symptoms and the vascular variations. The reason for this deficiency is that, because this the study is retrospective, the tests used for the differential diagnosis and the records of diagnostic methods cannot be standardized. Thus, in this study, apart from the sub-diagnostic groups, only the relationship between vascular variations and vertigo symptoms was examined. However, these vascular variants found in our study did not cause any severe symptoms that would require surgical intervention in the evaluated patient group.
Conclusions
Analysis of the prevalence of the vascular loops of the AICA primarily depends on diagnostic technique, and our results indicated a slightly higher prevalence than those of previous studies. This may be partly related to the very high sensitivity of 3D T2WI MRI, but it may also reflect ethnic differences between the study populations. Another important finding was the higher mean age of the patients with vertigo, which might be suggestive of the effect of aging on the emergence of neurovascular symptoms. The contradictory reports, both from anatomical and clinical studies, about the prevalence and role of vascular loops in the etiology of vertigo symptoms suggest that diagnosis should not be based on a single imaging methodology and must be supported by clinical and laboratory findings.