
Abstract
BACKGROUND:
A recent study has shown variability on the perception of verticality during unilateral centrifugation among patients with type 2 diabetes mellitus; it is yet unknown if it is related to symptoms of unreality.
OBJECTIVE:
In patients with type 2 diabetes mellitus compared to age matched healthy volunteers, to assess depersonalization/derealization (DD) symptoms before and after unilateral centrifugation, according to the subjective visual vertical (SVV).
METHODS:
47 patients with type 2 diabetes mellitus and 50 age matched healthy volunteers participated in the study. They replied to standardized questionnaires of symptoms related to balance, depression, and anxiety. Then, after neuro-otological evaluation, they completed a DD inventory before and after unilateral centrifugation (300°/s, 3.85 cm) with SVV estimation.
RESULTS:
Right/left asymmetric SVV during centrifugation was identified in 17 patients (36%) and no SVV change during centrifugation was identified in 6 patients (13%). Before centrifugation, patients with asymmetric SVV already reported some of the DD symptoms, while patients with no SVV change reported almost no DD symptoms. Unilateral centrifugation provoked an increase of DD symptoms in both healthy volunteers and the entire group of patients (repeated measures ANOVA, p < 0.01), except in the 6 patients with no SVV change. Before centrifugation, the DD score showed influence from the SVV subgroup and the evidence of depression (MANCoVA, p < 0.01); after centrifugation, which provoked asymmetry of the right/left utricular input, only the influence from depression persisted. No influence was observed from the characteristics of the subjects, including retinopathy, peripheral neuropathy (assessed by electromyography) or weight loss, or from the total score on the questionnaire of symptoms related to balance.
CONCLUSIONS:
In patients with type 2 diabetes mellitus and healthy volunteers, utricular stimulation by unilateral centrifugation may provoke DD symptoms, with an influence from depression. The results support that the aphysiological utricular input given by unilateral centrifugation may contribute to create a misleading vestibular frame of reference, giving rise to ‘unreal’ perceptions.
Introduction
To interact effectively with the environment, adequate updating of the frame of reference is required. Evidence suggests that sensory dysfunction could provoke distress as well as discrepancy between the multi-sensory frame given by experience and the actual perception [35]. In the general population, symptoms of unreality (depersonalization/derealization symptoms) are common, independently of socio-economic status, sex, education, religion, or place of birth [32]. Transient depersonalisation is frequent [15, 32], with a lifetime prevalence rate between 26% and 74% [15].
Altered perceptions of the self and the environment are termed dissociation phenomena. Depersonalization is defined as the subjective experience of unreality and detachment from the self, and derealisation is defined as the experience of the external world appearing strange or unreal [1]. Although, depersonalization/derealization disorder is a psychiatric diagnosis with specific criteria [1]; symptoms of depersonalization/derealization (DD) have been described in patients with a variety of psychiatric, neurological and sensory disorders [6, 27].
In patients with vestibular disease, DD symptoms can be related to spatial disorientation [11, 22]; while in the general population, depersonalization symptoms may be an independent predictor for dizziness [37]. Additionally, in healthy subjects, DD symptoms can be provoked by vestibular stimulation, either of the semi-circular canals [4, 33] or the utricles [2]. The vestibular discrepancy may disturb the multisensory mechanisms involved with perceiving orientation in space [22].
Impairment of the otoliths has been recognized in adult patients with type 2 diabetes mellitus, either by vestibular evoked myogenic potentials or by unilateral centrifugation, with or without semi-circular canal dysfunction [17, 39]. The physiopathology of such disarray is yet unknown. On the other hand, even though, evidence has shown that unilateral centrifugation may provoke DD symptoms in healthy subjects [2], there are no studies on the possible association between the perception of verticality during unilateral centrifugation of patients with type 2 diabetes mellitus and DD symptoms. The present study was designed to assess DD symptoms according to the subjective visual vertical (SVV) during unilateral centrifugation, in patients with type 2 diabetes mellitus compared to age matched healthy volunteers.
Methods
Participants
After approval of the research protocol by the Institutional Research and Ethics Committees (IMSS; R 2017-785-007), informed consent was obtained from all participants and the study was performed according to the Declaration of Helsinki and its amendments.
A total of 100 subjects gave their informed consent to participate in the study. However, 3 patients with diabetes mellitus were excluded, because they became sick during unilateral centrifugation. Those who participated in the study were:
Forty seven patients (28 to 83 years old; 12 women/ 35 men), with type 2 diabetes mellitus (8.6±6.8 years elapsed since diagnosis), of whom 27.6% had peripheral neuropathy and 31.9% had retinopathy. They had no clinical history of vestibular disease and they denied ever experiencing vertigo. During a preliminary neurotology evaluation, they showed no abnormality during oculo-motor, postural or caloric tests. The most frequent medication for the diabetes mellitus was metformin (55.3%), though 34% of the patients were receiving insulin treatment.
Fifty healthy volunteers (29 to 83 years old; 25 women/25 men), with confirmed adequate vestibular function by neuro-otology evaluation, which included oculo-motor and postural tests, as well as sinusoidal rotation and unilateral centrifugation.
All the participants denied having a history or medical record of otology, neurology or psychiatry disorders (submission to psychiatric care or psychopharmacy), or exposure to ototoxic medication or unsafe noise levels. All the patients had similar access to health care, but none of them were seeking medical care due to sensory or balance decline.
According to the selection criteria, patients were consecutively invited to participate when attending their clinical follow-up for diabetes care. After acceptance, fulfilment of the selection criteria was verified. None of them had evidence of middle ear disease or caloric test asymmetry (range from 1% to 12%); only 10 patients showed an average threshold for middle frequencies ≥25 dBnHL (range from 25 to 46 dB nHL) due to sensori-neural hearing loss. All patients were intentionally assessed for retinopathy, and clinical evidence of polyneuropathy was confirmed by electromyography (Nihon Kohden MEB 9400, Tokyo).
Procedures
All participants completed the following questionnaires: A standardized questionnaire of symptoms related to balance, which was validated on a similar population (Kurder Richardson 20 = 0.75, intra-class rank correlation coefficient = 0.9) [19], which includes 9 items with no/ yes responses (Fig. 1); where a “no” response is scored 0 points and a “yes” response is scored 1 point, except for the report of vertigo which is scored 2 points. For the item “frequent falls “, a “yes” response is considered when reported to occur ≥1 / month, and for “frequent” stumbles” when occurring ≥1 / week. A total score is obtained by adding-up all the points, with a range from 0 to 10, where a score ≥4 may be related to balance disorders [18, 19]. The 17 item-Hamilton Depression Rating Scale [13], rated on a 5-point scale as 0 = absent; 1 = doubtful to mild; 2 = mild to moderate; 3 = moderate to severe; 4 = very severe. The total score range from 0 to 48, where a score between 0 to 7 points is considered in the normality range. The Zung Instrument for Anxiety Disorders [40], which is a 20-item scale with some items keyed positively and some negatively; it is scored on a four-point scale ranging from 1 “none or a little of the time” to 4 “most or all of the time”. The total score range from 20 to 80, where a score between 20 and 44 is considered in the normality range.
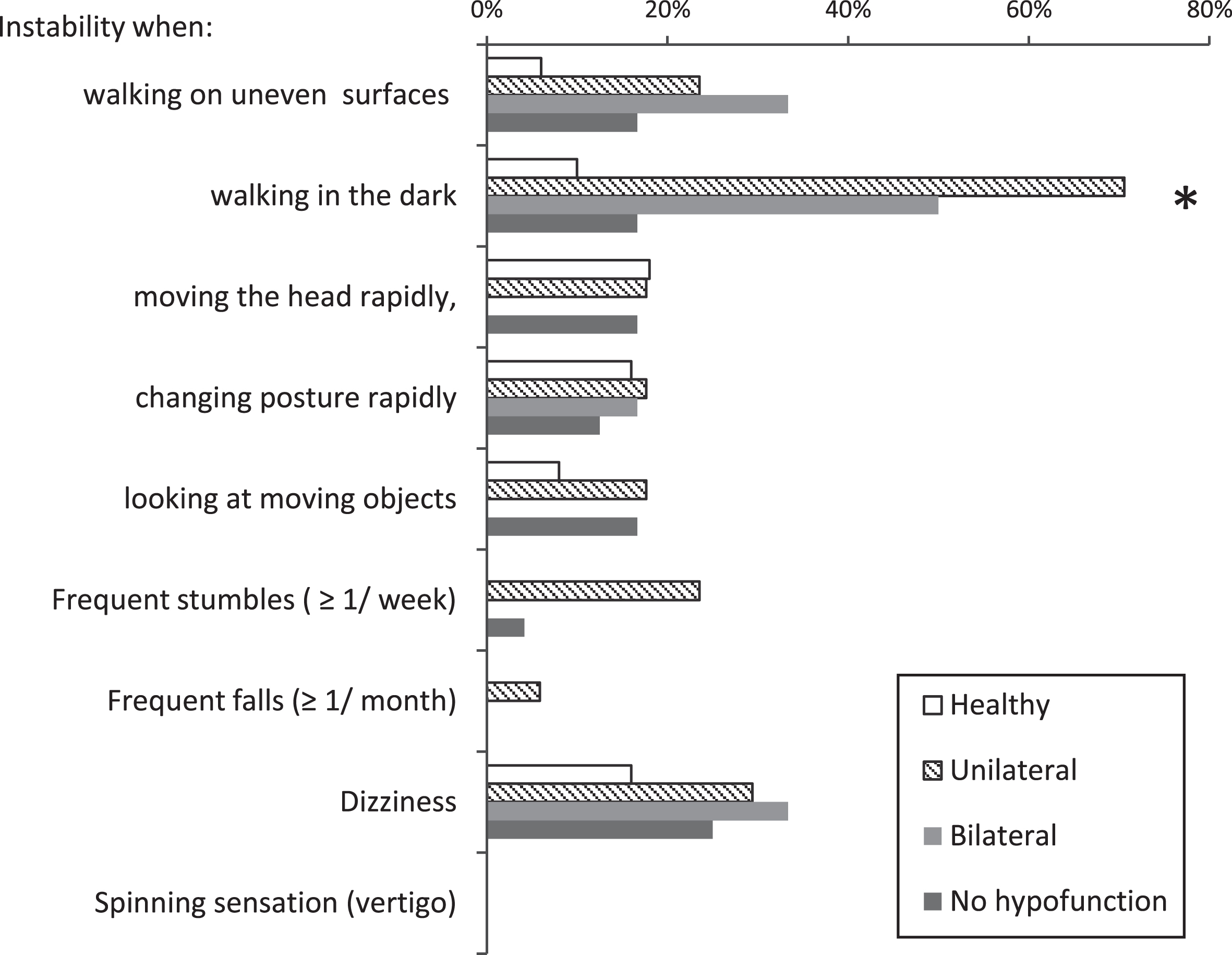
Frequency of symptoms related to balance reported by 47 patients with diabetes mellitus, 24 with SVV similar to healthy subjects & 23 with SVV different from healthy subjects, and 50 healthy volunteers. *Marked differences by using ANOVA (p < 0.05).
Neuro-otology evaluation included eye movement recordings, sinusoidal rotation at 0.16 Hz and at 1.28 Hz (60°/s peak velocity), static visual vertical (average of 10 trials) and dynamic visual vertical during unilateral centrifugation (I-Portal-NOCT-Professional with VEST operating and analysis software, Neuro-Kinetics, Pittsburgh) [for review see 7, 10]. Since the study was designed to assess a perceptual effect of unilateral centrifugation, the subjective visual vertical during unilateral centrifugation was selected because it requires additional processing of otolithic information in higher brain centers [for review see 7].
Unilateral Centrifugation was performed according to the protocol of the manufacturer: at 300°/sec peak velocity and 3.85 cm linear translation to the right and afterwards to the left, with 2 sec start dwell, 60 sec ramp up time, 375 sec peak time, 60 sec centrifugation start time and 60 sec ramp down time. Asymmetric SVV during centrifugation was considered when right/left asymmetry was out of 3 standard deviations from that of healthy volunteers. No SVV change is reported when no SVV change was evident during either right or left centrifugation. Accordingly, patients were classified in 3 subgroups (Table 1): 17 patients with asymmetric SVV during right/left centrifugation, 6 subjects with no SVV change during right/left centrifugation and 24 patients with similar SVV to healthy subjects during right/left centrifugation.
General characteristics of the 47 patients with type 2 diabetes mellitus and 50 healthy volunteers who participated in the study. Comparisons between the entire group of patients and healthy volunteers were performed using “t” test (either for proportions or for means)
Before and after unilateral centrifugation to the right and to the left, an inventory of DD symptoms [8] was administered (<5 minutes, to come out from the rotating chair). The DD inventory by Cox and Swinson [8] is a self-report measure of DD symptoms for use with clinically anxious patients, rather than in the context of dissociative disorders. Repeatability of responses in healthy subjects, 21 to 81 years old (with a General Health Questionnaire 12 score≤2), within the same day, has shown that the total score is repeatable in 91% of the cases (repeatability coefficient of 2), while responses to each item are repeatable in 91% to 100% of the cases [11]. In comprises 28 items rated on a scale from 0 to 4, where 0 = does not occur, 1 = mild, 2 = moderate, 3 = severe and 4 = very severe. The total score range from 0 to 112, no cutoff score to consider normality has been suggested.
Statistical analysis was performed using “t” test, Wilcoxon test, Chi-square, repeated measures analysis of variance analysis of covariance (ANCoVA), and multiple analysis of covariance (MANCoVA) to include repeated measures analysis. The significance level was set at 0.05, for two tails.
Results
Characteristics of the participants
The characteristics of the patients and healthy volunteers are shown in Table 1. The two groups had similar age. The group of patients with diabetes had lower education level than the group of healthy volunteers (“t” test, p < 0.001), except for the patients with no SVV change during centrifugation who reported the highest education level among the patients (Table 1). Tobacco and smoking habits were infrequent in the 2 groups. The number of sleep hours per week was also similar between the 2 groups. However, recent weight loss was more frequent in patients with diabetes than in healthy volunteers (“t” test, p < 0.05).
In patients with diabetes mellitus, retinopathy was diagnosed in 29% (n = 5) of those with asymmetric SVV during centrifugation; 16% (n = 1) of those with no SVV change during centrifugation and 37% (n = 9) of those with SVV similar to healthy subjects; while peripheral polyneuropathy was confirmed in 35% (n = 6) of those with asymmetric SVV during centrifugation; 16% (n = 1) of those with no SVV change during centrifugation and 24% (n = 6) of those with SVV similar to healthy subjects.
A score > 7 on the Hamilton Depression Rating Scale [13], suggesting depression, was observed on 51% (n = 24) of the patients and 20% (n = 10) of the healthy volunteers. Among the patients a score > 7 was observed on 53% (n = 9) of those with asymmetric SVV during centrifugation, 33% (n = 2) of those with no SVV change during centrifugation and 54% (n = 13) of those with SVV similar to healthy subjects.
A score > 44 on the Zung Instrument for Anxiety Disorders [40], suggesting anxiety, was observed on 4% of the patients (n = 2, with asymmetric SVV during centrifugation) and none of the healthy volunteers. The total score for each group and subgroup is described in Table 1.
Vestibular function
Apart from decreased SVV change during centrifugation, compared to healthy volunteers, patients with diabetes mellitus showed decreased gain to sinusoidal oscillation in the dark (“t” test, p = 0.003), just at 0.16 Hz, with adequate responses during sinusoidal rotation with visual suppression and with visual enhancement (Table 1).
Symptoms related to balance
The report of symptoms related to balance is shown in Fig. 1. None of the participants reported vertigo, while dizziness was reported by circa one third of the patients of any subgroup and 16% (n = 8) of the healthy volunteers. In patients with SVV during centrifugation different from healthy subjects, the most frequent symptoms were “instability when walking in the dark”, mainly in patients with asymmetric SVV during centrifugation, and “instability when walking on uneven surfaces”, mainly in patients with no SVV change during centrifugation (Fig. 1). However, the healthy volunteers and the patients with SVV during centrifugation similar to healthy subjects reported few symptoms (Fig. 1). Analysis of covariance showed that the report of “instability when walking in the dark” had influence from both the SVV subgroup and the evidence of peripheral neuropathy (ANCOVA, whole model R2 = 0.2, p < 0.001).
Depersonalization/derealization symptoms
The frequency of each symptom is described in Table 2. Prior to unilateral centrifugation, the number of symptoms reported by the patients in the DD inventory ranged from 0 to 26 (median 6), and in healthy volunteers the range was from 0 to 25 (median 2). Comparison between the 2 groups showed that, among other symptoms, patients reported “Difficulty focusing attention” more frequently than healthy volunteers (60% versus 18%, “t” test, p < 0.05) as well as “Body fells numb” (36% versus 12%,“t” test, p < 0.05).
Frequency and severity (score range) of DD symptoms reported before and after centrifugation by 47 patients with diabetes mellitus, according to SVV during centrifugation, and 50 healthy volunteers; significance of <0.05 (in black) is given for “t” test for proportions
Frequency and severity (score range) of DD symptoms reported before and after centrifugation by 47 patients with diabetes mellitus, according to SVV during centrifugation, and 50 healthy volunteers; significance of <0.05 (in black) is given for “t” test for proportions
After centrifugation, the number of symptoms reported by the patients ranged from 0 to 28 (median 8), and in healthy volunteers the range was from 0 to 28 (median 7). The entire group of patients showed an increase on the report of 10 of the DD symptoms (Wilcoxon test, p < 0.05), while healthy volunteers showed an increase on the report of 14 of the DD symptoms (Wilcoxon test, p < 0.05). However, in the group of patients, the increase was mainly related to the responses from patients with SVV similar to healthy subjects (Wilcoxon test, p < 0.05), since patients with asymmetric SVV during centrifugation showed an increase on the frequency to report just 5 of the symptoms (Wilcoxon test, p < 0.05), and patients with no SVV change during centrifugation showed no significant increase on the report of any of the symptoms (Wilcoxon test, p > 0.05). Even more, patients with no SVV change during centrifugation completely denied 15 of the DD symptoms (Table 2). Repeated measures analysis of variance showed that the increase of the total score was significant for the 2 groups (ANOVAr, p < 0.0001). Although patients with asymmetric SVV during centrifugation showed variable responses while patients with no SVV change during centrifugation showed no change.
Comparison of the total score of patients with no SVV change during centrifugation and those of an age matched subgroup of healthy subjects (mean age 64.5±11 years old) showed similar results for each evaluation, but divergence on the score change after centrifugation, since patients with no SVV change during centrifugation showed a small decrease while healthy subjects showed a small increase (Chi-Square, p < 0.02).
The most frequent symptoms reported by all participants were “Body feels strange or different in some way”, which was reported by 71% of the patients with/ without asymmetric SVV during centrifugation and by 48% of the healthy volunteers; and “Surroundings seem strange and unreal” which was reported by 45% and 47% of the patients with either similar or different SVV from healthy subjects, respectively, and by 42% of the healthy subjects (Table 2).
In all participants, multiple analysis of covariance showed that, before centrifugation, the total score of the DD questionnaire had an influence from the subgroup of SVV during centrifugation and the evidence of depression (MANCoVA, whole model R2 = 0.3, p < 0.0001), with interaction between these two variables (β= 0.28, 95% C.I. 0.05–0.52). However, no influence was observed from the general characteristics of the subjects, including retinopathy, peripheral neuropathy and weight loss, or from the total score on the questionnaire of symptoms related to balance. Nevertheless, after asymmetric utricular input was induced by unilateral centrifugation, the total score of the DD questionnaire had influence just from the evidence of depression (MANCoVA, whole model R2 = 0.18, p < 0.01).
The results show that the perception of unreality may be related to the perception of verticality during utricular stimulation, by unilateral centrifugation, with influence of depression.
The results are consistent with previous studies, using the same DD inventory, in which healthy subjects have reported an increase of DD symptoms during asymmetric vestibular stimulation, either of the semi-circular canals or the utricles, with no influence of their general characteristics [2, 33]; while patients with unilateral vestibular dysfunction have reported DD symptoms with a higher frequency and severity than patients with bilateral dysfunction [33]. The findings support that both, vestibular input asymmetry and the clinical evolution of a vestibular dysfunction, may have an influence on the perception of unreality. However, since the multivariate analysis showed that just a third of the variance could be explained by the variables selected for the study, additional factors should be considered to understand the clinical meaning of this influence.
In this study, after centrifugation, healthy subjects and patients with SVV during centrifugation similar to healthy subjects reported some DD symptoms that patients with asymmetric SVV during centrifugation have already reported before centrifugation (Table 2), while patients with no SVV change during centrifugation denied those symptoms before and after centrifugation (Table 2). In addition, the high variability of responses from patients with asymmetric SVV during centrifugation suggests variable clinical evolution within that subgroup. This finding is consistent with the decrease of DD symptoms at recovery from vestibular failure [11]. Then, the variability of DD symptoms could be related to a reweighting of the sensory information available during the evolution of the disease, which in turn is in agreement with the plasticity of the multisensory integration required to maintain the interaction with a variable environment [28, 38].
Transient depersonalization is commonly described accompanying a variety of psychiatric disorders, including depression. In this study, a consistent relationship between the report of DD symptoms and depression symptoms was evident both, before and after centrifugation. This finding is in agreement with previous studies supporting a relationship between mood disorders and depersonalization [24, 34]. However, in this study no influence from anxiety symptoms was observed. Although the relationship between anxiety and depersonalisation remains controversial, this finding cannot deny a possible relationship between the report of DD symptoms and anxiety, since it may be related to the low prevalence of anxiety observed in the source population [5, 30], or even to the inventory used to assess anxiety [40]. In adults (18–65 years old) from urban areas of the source population of this study, a national survey on psychiatric epidemiology showed a prevalence of 3.4% of any anxiety disorder [30].
The most frequent symptom related to balance reported by the patients was “instability while walking in the dark”, which prevailed in patients with asymmetric SVV during centrifugation. This result is consistent with an increased prevalence of postural instability and swaying/rocking sensation in patients with isolated unilateral utricular dysfunction, who can report no vertigo [31]. Remarkably, in such conditions, patients would have to rely more on somatosensory and vestibular inputs [29]. Since just one third of the patients had peripheral polyneuropathy, the high frequency of “instability while walking in the dark” among patients with SVV during centrifugation different from healthy subjects suggests some utricular contribution to the instability [3, 26]. However, further studies are required to assess the influence of utricular dysfunction (assessed by utricular reflexes) with preserved canal function in patients with/without multisensory compromise.
Although, a number of patients with diabetes mellitus showed subclinical balance decline, none of the participants had vertigo, and dizziness was reported just by circa one third of the patients. This finding is consistent with previous evidence showing that patients with diabetes mellitus may have subclinical sensory decline, including balance [14, 21]. In a previous study, patients with type 2 diabetes mellitus who were enrolled at primary health care showed unilateral utricular hypofunction with no evidence of semi-circular canal dysfunction [17]. In this study, apart from SVV during centrifugation different from healthy subjects, the patients showed decreased horizontal semi-circular canal gain to sinusoidal stimulation at 0.16 Hz, with no clinically significant asymmetry. However, they were receiving secondary health care, and a third of them required insulin treatment. These findings also supports that patients with type 2 diabetes mellitus might have slow progressing vestibular dysfunction, related to the clinical evolution of the disease and aging, which could be subclinical [for review see 16].
The main limitation of this study is its cross-sectional design, which prevented us to discuss any causal relationship and allowed us to identify just the most marked relationships. In addition, since patients reported no history of previous vestibular disease, it was not possible to estimate the time frame of the dysfunction or its clinical progression, increasing the variability of responses. Longitudinal studies are needed to understand the vestibular influence on the perception of unreality. However, the finding of patients with no SVV change during centrifugation allowed us to contrast a full range of responses. In addition, the expected influence of retinopathy and peripheral neuropathy on the report of DD symptoms [20, 27] was not observed, probably because only about one third of the patients had retinopathy and a similar percentage had peripheral neuropathy, which were evident mainly in patients with SVV similar to healthy subjects. Another limitation of the study was the rely on self-report without psychiatric evaluation; as well as the failure to identify a possible relationship between the report of DD symptoms and anxiety, due to the low frequency of anxiety symptoms reported by the patients using the Zung Instrument for Anxiety Disorders [40]. Then, the results should not be translated directly into the clinical setting.
In the last decade, there has been a rapid growth of knowledge concerning utricle function. Grant and Curthoys have suggested that the utricular macula operates both as an accelerometer at low frequencies and as a seismometer at high frequencies [12]. However the design of this study just considered the perceptual responses to unilateral centrifugation (low frequency stimulation), without taking into account the responses to high frequency stimulation, which are evaluated by the vestibular evoked myogenic potentials. Future studies may distinguish the effect of distinct utricular stimulation on the perception of unreality.
In this study, in order to assess SVV, patients were asked to focus on the perception of verticality. Then, a bias was introduced in the insight, since evidence suggest that attention processes play a major role in coordinating the integration of inputs into a coherent mental representation [36].
The design of this study was mainly focused on the perceptual responses to aphysiological utricular input, and further studies would be required to unravel its repercussion on multisensory integration processes. However, the results are consistent with a predictive coding perspective [for review see 9]: mental representations of the external environment are actively constructed by brain processes, where congruent stimuli may result in a consistent internal model, with a low prediction error; when the information presented is incongruent across modalities, this may result in an inconsistency in the internal model, with a greater error signal and a weaker internal representation.
Conclusions
Aphysiologic utricular input, given by unilateral centrifugation, may arouse symptoms of unreality, with an influence from depression symptoms. The results support that distorted utricular signals may create a misleading vestibular frame of reference, giving rise to ‘unreal’ perceptions.
Footnotes
Acknowledgments
The study was supported by Fondo de Investigación en Salud: FIS/IMSS/PROT/G17-2/1733.