
Abstract
BACKGROUND
Vestibular dysfunctions result in a wide range of impairments and can have debilitating consequences on a person’s day-to-day activities. Conventional vestibular rehabilitation is effective but suffers from poor therapy compliance due to boredom. Virtual reality technology can make training more engaging and allow precise quantification of the training process. However, most existing technologies for vestibular rehabilitation are expensive and not suitable for use in patients’ homes and most clinics. In this pilot study, we developed and evaluated the usability of a smartphone-based head-mounted display (HMD) for vestibular rehabilitation and quantified the simulator sickness induced by the system.
METHODS
Two adaptive training games were developed to train discrete and rhythmic head movements in the pitch and yaw planes. The usability and simulator sickness associated with the system were evaluated in a single testing session on healthy subjects and patients with unilateral vestibular dysfunction. Additionally, the head movement kinematics measured during training was also analyzed using different movement quality measures.
RESULTS
A total of 15 healthy subjects and 15 patients underwent testing with the system. Both groups found the system to be highly usable (>80 score on the system usability scale). Following 20–30 min training with the system, healthy subjects reported minimal simulator sickness symptoms. On the other hand, patients reported a higher incidence rate for symptoms, which could have been the result of their vestibular condition.
CONCLUSION
The current study demonstrated the usability and safety of a smartphone-based system for vestibular rehabilitation. The system is compact, and affordable thus has the potential to become an excellent tool for home-based vestibular rehabilitation.
Keywords
Introduction
Unilateral peripheral vestibular dysfunction results in a wide range of problems such as dizziness, visual blurring, vertigo, postural instability, and imbalance during walking [24]. Peripheral vestibular diseases are the third most common cause of dizziness in elderly patients [20]. Vestibular conditions also significantly increase the incidence of fall, which has high associated health care costs and severely limits personal independence [13]. Patients with peripheral vestibular dysfunction often reduce or avoid head movements to prevent aggravating their symptoms, which also leads to secondary complications such as muscle tension, fatigue, neck pain, etc. [15]. Although pharmacological interventions are commonly used in the acute phase, vestibular rehabilitation plays a significant role in the recovery process.
Vestibular rehabilitation exercises are aimed at addressing the associated symptoms and functional impairments following vestibular dysfunction. Current rehabilitation exercises are a combination of four different components [13]: (1) gaze stabilization; (2) habituation of symptoms; (3) balance; and (4) walking. Conventional exercises are highly effective in the management of vestibular hypofunction, in particular reducing symptoms and improving function [21]. In general, regular training for 4 to 8 weeks can improve a patient’s condition with 20–40 min of therapy per day [14, 21]. Vestibular rehabilitation strongly relies on vestibular adaptation for the recovery of lost functions [5]. Horizontal (yaw plane) and vertical (pitch plane) head movements are the most commonly used exercises to induce vestibular adaptation and to increase vestibulo-ocular-reflex (VOR) gain [5]. It has been observed that the VOR gain reduces by 20–50% in patients following a vestibular lesion [1]. Repeated periods of retinal slip, induced by head movements, can induce vestibular adaptation and thus change the VOR gain.
Although effective, conventional vestibular rehabilitation exercises are repetitive and boring, and thus have poor compliance [24]. This prevents their effective implementation in the target population. Pavlou et al., reported a 40% increase in drop-out rate when exercises were not supervised and concluded that supervision promotes adherence and improves postural stability [27]. Furthermore, when training is unsupervised, it is non-progressive. Progressive grading of exercise difficulty is believed to be an essential requirement for effective recovery [14].
Technology-based exercise tools, in particular, virtual reality (VR), can overcome the drawbacks of conventional vestibular rehabilitation. The current literature reports a wide range of tools, such as the wide field-of-view (FOV) screens [9, 28], computer-based platforms [11], commercial gaming platforms [5, 23], and also head-mounted displays [7, 32]. Many of these devices have undergone preliminary evaluation in patients with vestibular dysfunction and also elderly subjects. A list of existing technologies for vestibular rehabilitation in the current literature, reported between 2000 and 2015, is listed in Table 1. The technologies listed in this table were identified through a Google Scholar search using the keywords – “virtual reality”, “vestibular rehabilitation”, “visual vertigo”, “optokinetic simulation”, and “balance rehabilitation”. Overall, there is reasonable evidence that technology-based interventions result in better compliance and are at least as effective as conventional therapy [16, 23].
Summary of different technologies for vestibular rehabilitation in the current literature. The table consists of the list of all devices reported between 2000 and 2015, searched using Google Scholar with the keywords – “virtual reality”, “vestibular rehabilitation”, “visual vertigo”, “optokinetic simulation”, and “balance rehabilitation”
Summary of different technologies for vestibular rehabilitation in the current literature. The table consists of the list of all devices reported between 2000 and 2015, searched using Google Scholar with the keywords – “virtual reality”, “vestibular rehabilitation”, “visual vertigo”, “optokinetic simulation”, and “balance rehabilitation”
Among the different existing systems, the head-mounted display (HMD) is the most suited for clinical and home use, because it is compact, portable, and requires little additional infrastructure. HMDs are also relatively cheaper than most of the other VR systems for an immersive 3D experience. However, current commercial HMDs are still expensive for most patients to afford for home-based training. Fortunately, with the recent developments in smartphone technology and VR headsets (such as Google Cardboard [10]), it is now possible to develop affordable HMDs for everyday use. Given the ubiquitous nature of smartphones and the availability of affordable commercial HMD headsets, a smartphone-based HMD for vestibular rehabilitation would be easy to use, economical, portable, and allow easy implementation of home-based therapy.
The current work was aimed to develop and study the usability of a smartphone- based VR HMD for vestibular rehabilitation on patients with unilateral vestibular dysfunction. We carried out a pilot usability study with 15 patients and 15 healthy subjects, undergoing a one-off testing session. The goal was to evaluate the system’s usability and simulator sickness (SS) following up to 30 min of training with the HMD. The two primary outcome measures were the system usability scale (SUS) [2] and the simulator sickness questionnaire (SSQ) [18]. A preliminary analysis of head movement quality was also carried out using the kinematic data recorded by the smartphone during training.
The vestibular rehabilitation system that was developed is called the VEstibular GAming System (VEGAS). VEGAS is a smartphone-based 3D VR headset, along with a set of VR games developed for vestibular training and assessment. The choice of a smartphone-based headset for VEGAS was motivated by (a) the increasing popularity and reducing prices of powerful Android smartphones; (b) the availability of affordable smartphone headsets; and (c) the availability of a set of open source tools for developing software for smartphone-based HMDs. In the current study, the VEGAS (Fig. 1) used an LG Nexus 5X smartphone (OS version: Android M; Sensors: BMI160 accelerometer, BMI160 Gyroscope, BMI150 Magnetometer) and a Convergence VR headset (Convergence VR Tech Labs Pvt. Ltd).
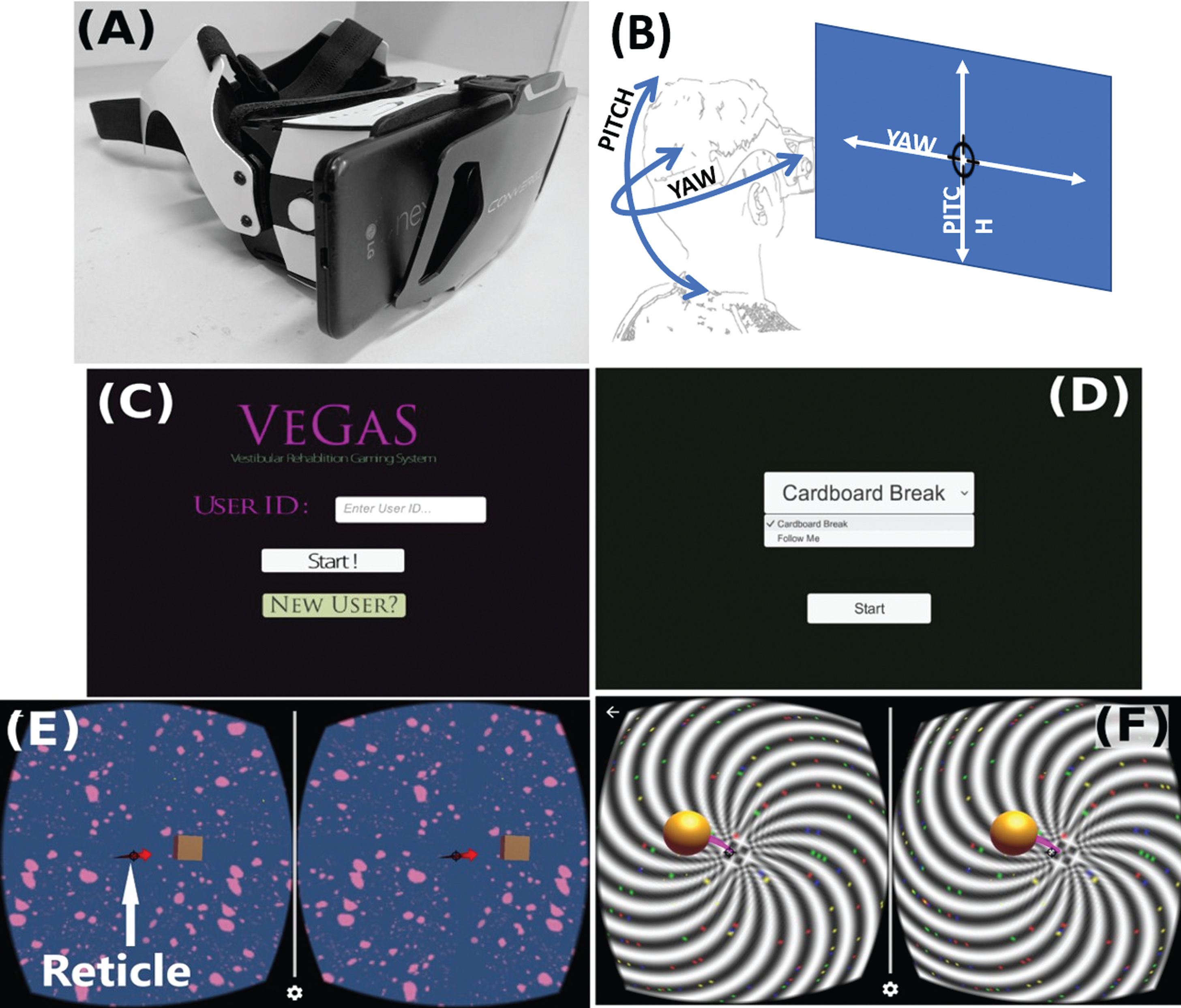
Picture of the VEGAS HMD and screenshots of the two games. (A) Image of the Nexus 5X phone in the Convergence headset; (B) The head movements of the subject is sensed by the phone and is mapped to the movements of the reticle in the virtual environment. The pitch is mapped to up-down motion of the reticle; the Yaw is mapped to the left-right movement of the reticle (C) Screenshot of the user selection/creation page in the VEGAS app; (D) Screenshot of the game selection page; (E) Screenshot of the “Cardboard Break” game with vivid and static background; and (F) Screenshot of the “Follow Me” game with a vivid and moving background.
The VR games for VEGAS were developed as an Android app using the Unity ® Game Engine (Unity Technologies). The VEGAS app consists of a graphical interface (Fig. 1) for user information management, which allows a clinician to create and manage patient accounts and choose the game of interest for either training or assessment. All relevant patient-related information is stored on the phone in individual folders for each patient, with individual subfolders to store data from each game.
The current version of the VEGAS has two training games with graded levels of difficulty: (a) “Cardboard Break”, and (b) “Follow Me”. Both games were designed based on exercises used in conventional rehabilitation to encourage head movements/gaze stabilization. Head rotations were measured using the phone’s in-built inertial measurement unit to measure the pitch and yaw angles. These angles controlled the subject’s movements in the virtual game: pitch controlled the vertical (up-down) movements, while yaw controlled the horizontal (left-right) movements. During training, the game’s difficulty level is automatically chosen using an adaptive performance-based algorithm. The data from the device was sampled at 35 Hz frame-rate for graphics update on the Nexus 5X phone, running the VEGAS and Chromecast application. A demo video of the VEGAS is provided as a Supplementary Video S1.
Cardboard break
The “cardboard break” (CB) game aims to induce retinal slip by having subjects perform discrete head movements in the pitch and/or yaw planes (Fig. 1). This exercise is a modified version of the two target gaze exercise [33]. The subject plays the game through head movements that control the position of the reticle1 in the virtual environment (Fig. 1). The reticle is in the center of the visual field, and the goal of the subject is to position this reticle on a cardboard box that appears at some spatial location in the virtual environment. When the target cardboard box appears, the subject performs a head movement to move the reticle to the box; this induces a retinal slip. When the subject places the reticle on the cardboard box for 500 ms the box explodes (and the patient scores a point), and another box appears at a different location. Patients continue to move and break these boxes for 30 s, and their goal here is to break as many boxes as possible within the stipulated time of 30 s.
The CB game has twelve different difficulty levels, corresponding to different combinations of range of movements (near and far), movement direction (pitch, yaw or both), and visual field backgrounds (plain, vivid and dynamic). The details of the different game levels are provided in Table 2. The difficulty levels are arranged based on the assumption that:
The different difficulty levels of the “Cardboard Break” game
The different difficulty levels of the “Cardboard Break” game
‘Far targets’ require relatively larger head movements than ‘near targets’ targets. Since the goal in the CB game is to break as many boxes as possible, targets located at larger distances would require faster head movements, which would induce larger retinal slips. Thus, making farther targets more difficult to attain.
Combined pitch (vertical) and yaw (horizontal) movements, where the subjects move diagonally towards the target, are more difficult than simple pitch or yaw movements [30], and
A dynamic, and vivid visual background is more difficult than a vivid or plain one [27]. The plain background is a uniformly colored background on which the game is displayed. The vivid background consists of a static optokinetic stimulus, while the dynamic background consists of a rotating optokinetic stimulus. These backgrounds can be seen in the Supplementary video S1. The difficulty rating of these different backgrounds is based on the observation that optokinetic stimulation, combined with vestibular exercises, has been shown to improve vertigo-like symptoms in patients with vestibular dysfunction [27].
The “follow me” (FM) game requires subjects to perform continuous or rhythmic movements in pitch, yaw, or both directions. In this game, the subject sees a red ball (target) which moves in the virtual environment following a specific trajectory. The objective is to track this target by placing the reticle on the moving target for the entire game duration. When the subject places the reticle within the target, continuously for 1 sec, he/she scores a point. A single trial of the game lasts for 30 s. The target trajectory was generated using windowed sinusoids in the pitch and yaw planes (Equation 1).
The FM game has six different difficulty levels corresponding to different combinations of range of movements (A x , A y ), target speed (ω x , ω y ), and visual field background (please refer to Table 3 for details). This game only used two of the backgrounds from the CB game – ‘vivid stationary’ and ‘vivid moving’ (Table 3); the ‘normal’ background was not used since we did not want to have too many difficulty levels in FM game.
The different difficulty levels of the “Follow me” game. A x and A y are the amplitudes of the target movement in the pitch and yaw directions, respectively, in game units. One game unit corresponds to 45deg of movement. ω x and ω y (rad/sec) are the angular rates for the sinusoidal trajectories in the pitch and yaw directions
The vestibulo-ocular reflex (VOR) cancellation is likely to be minimal in the FM game because of the use of complex target trajectories (combination of sinusoids) and the short duration for the game trials. These two factors will hinder patients from learning and predicting the target trajectory pattern, thus making the target trajectory appear random or pseudo-random to the patients. Thus, in order to play the game, patients would have to continually update their gaze and head movements to follow the target visually, which will induce retinal slip.
The CB and FM games used an adaptive algorithm to automatically select the game level during training. The adaptation was based on patient performance on the recently completed trials of a particular game. Performance p [n] in a given trial n was +1 if the game was successfully completed, else it was -1. Success in a given trial for the CB game was defined as 20 or more cardboard breaks and for the FM game a score of at least 15, i.e., the patient was able to track the target for at least 15 s of the stipulated 30 s trial duration. These success criteria were based on a pre-pilot study that was carried out on healthy subjects; we chose values that were roughly 70% of healthy performance. Adaptation of game level was based on continued success or failure represented by P [n], which is defined as the following,
The following adaptation rule was used to choose a game level for the (n + 1)
th
game trial,
As a first step towards evaluating VEGAS, a usability study on healthy subjects and patients with unilateral vestibular dysfunction was carried out in a single testing session lasting up to 30 min. The system usability was evaluated using a validated subjective measurement tool called the system usability scale (SUS) [2]. Additionally, the SS was also tested using the SSQ [18].
Study participants
The current study was approved by the institutional review board (IRB) of the Christian Medical College (CMC) Vellore (IRB registration number: 9774). The study included a convenience sample of 15 patients with unilateral dysfunction and 15 healthy subjects. This sample size was chosen based on the existing evidence that a sample size of at least 12 was required to estimate system usability using the SUS [23] reliably.
The healthy volunteers recruited in this study were between 18 to 60 years of age with no reports of middle ear pathology and had never suffered from dizziness, vertigo, and imbalance.
The patients in the study were recruited from the ‘Audio vestibular clinic’ of the Ear, Nose and Throat (ENT) department at CMC Vellore. An experienced otolaryngologist assessed all patients who were recruited for the study. Patients detected with unilateral peripheral hypo-function using an electronystagmogram via caloric testing were included in the study. The inclusion criteria for recruitment were: (a) age between 18 to 60 years with a minimum best-corrected vision of 6/6; (b) a clinical diagnosis of peripheral unilateral vestibular dysfunction (confirmed via electronystagmogram tests), and no other neurological deficit; (c) have one of the following complaints indicating incomplete vestibular compensation: disequilibrium, imbalance while walking, vertigo/dizziness, or head movement induced dizziness; and (d) score zero on the SSQ carried out before the start of the VEGAS training session, indicating that patients had not been experiencing any symptoms associated with their vestibular dysfunction or SS prior to the start of the study. This is an essential requirement to prevent excessive aggravation of vestibular/SS symptoms. Even in conventional vestibular rehabilitation, patients are advised not to train or perform activities when they are experiencing such symptoms [13]. Patients were excluded from the study if: (a) they were unwilling or unable to use the smartphone-based system. This was identified through a short orientation session where patients used the system for about 5 min, trying the CB and FM games; or (b) non-zero score on the pre-SSQ scored before the start of VEGAS training.
All potential study participants were provided with an information sheet regarding the study and were recruited upon providing informed consent. There were no patients with Meniere’s disease, and the cause of vestibular dysfunction in all patients, the duration of symptoms in patients, and baseline characteristics of the patients are provided in the Table S6 in the Supplementary file.
Protocol: Patients
After obtaining informed consent, patients trained with VEGAS for 20–30 min, playing the CB and FM game, in a seated position on a chair. We recruited patients with a pre-SSQ score of zero and patients who were able to tolerate the system after a short 5 min pre-test. Patients were given extra time to play the games if they wanted to play a little longer. However, if patients complained of uneasiness, headache or any symptom related to SS, the training was immediately stopped. For each of the two games, patients always started from the lowest level and played the game with the adaptive algorithm that automatically changed the difficulty level. Patients were given rests, whenever needed, in between the game trials.
Protocol: Healthy
Healthy subjects were tested in the current study for two primary reasons: (a) to evaluate the level of SS induced by VEGAS; and (b) to obtain normative data for the different games, which could serve as a benchmark for assessing patient performance in the different games. After a healthy subject gave informed consent, he/she underwent a one-off testing session with VEGAS. Each subject played all the 12 and 6 levels of the CB and FM games, respectively, in a seated position; the levels were presented in random order. After the completion of each level, subjects were allowed to rest for as long as they required. The testing sessions for each healthy subject lasted approximately 20 min.
Outcome measures and statistical analysis
The two primary outcome measures for the study were the SUS and the SSQ. The SUS is a simple questionnaire-based assessment tool for capturing the subjective assessment of the usability of a system [2]. The SSQ is currently the standard method used for assessing SS [18]. It is used in the current study to evaluate SS induced by the VEGAS HMD and the games, in both healthy and patient subjects. The SSQ was administered at the time of recruitment (pre-SSQ) to ensure none of the participants had any complaints related to SS before the start of the testing session. The pre-SSQ scores for all participants was zero. Immediately after playing the games with VEGAS, subjects filled out the SSQ (post-SSQ), followed by the SUS. A Mann-Whitney U test was carried out on the post-SSQ scores of patients and healthy subjects to test for differences in the two populations when using the VEGAS. The secondary outcome of the study was a set of movement quality measures estimated from the raw head movement data recorded by VEGAS during gameplay. The details of the analysis carried out on movement quality are provided in Section 1 of the Supplementary file.
Results
The usability of VEGAS was evaluated on 15 patients with unilateral vestibular dysfunction and 15 healthy subjects in a single testing session. All patients that satisfied the inclusion criteria were allowed a 5 min pre-test session with VEGAS. All patients tolerated the 5 min pre-test session, and all of them went through the full 20–30 min training session. In this section, we first present the results from the SUS and SSQ, followed by the analysis of head movement quality using the data collected by VEGAS.
Usability of VEGAS
The summary of the SUS obtained from patients and healthy subjects at the end of VEGAS training session is provided in Table 4. Overall, the system was found to be highly usable by patients (88.33±11.44) and healthy subjects (91.5±4.41), a score of 85 and above indicates excellent usability [18]. The details of the subjects’ response to the different SUS components is provided in Table S3 in the Supplementary file. Twelve of the 15 patients reported an overall score of 80 and above, with three patients P02, P06 and P08 reporting scores of 65, 77.5 and 67.5, respectively. Patient P02 found the system too complex to use, while P06 experienced neck pain and felt the smartphone screen was too bright (Table S6 in in the Supplementary file).
Summary of SUS and post-SSQ scores for patients and healthy subjects that participated in the usability study
Summary of SUS and post-SSQ scores for patients and healthy subjects that participated in the usability study
Immersive VR systems, in particular, HMDs supporting the stereoscopic 3D view, have been shown to induce SS [12]. The SS-induced by VEGAS was evaluated on healthy subjects and patients immediately following the completion of the testing session. Overall, the healthy subjects reported a mean total SSQ score of 5.41±12.43, and mean scores of 0.64±2.46, 3.02±6.24, and 1.76±4.64 for nausea, oculomotor, and disorientation SSQ subscales, respectively. Out of the 15 healthy subjects, only 4 (≈ 27%) reported any form of SS (Table 4). Ignoring the severity of rating for the different symptoms, if we only count the number of non-zero responses for the different symptoms (indicating its presence or absence), we observe an incidence rate of 0.95%, 5.71%, and 2.67% for nausea, oculomotor and disorientation symptoms, respectively (Table S4 in the Supplementary file).
On the other hand, the patients reported an average of (53±40.98) as their total SSQ score; a Mann-Whitney U test indicated that this score was significantly higher than that of healthy subjects (p = 2.296 × 10-5). Patients reported mean scores of 7.63±8.98, 21.61±18.22, and 23.76±18.13 for the nausea, oculomotor and disorientation SSQ subscales. Out of the 15 patients, 14 (≈ 94%) patients had reported some form of SS following training (Table 4). The incidence rates for nausea, oculomotor, and disorientation symptoms were 10.48%, 31.43%, and 22.67% respectively (Table S5 in the Supplementary file). No differences in the SSQ were observed between males and females in the healthy and patient groups, unlike a recent study that found females to be more susceptible to SS following VR training using a HMD [25].
Adaptation of game difficulty
Only the patient group trained with the adaptive algorithm for automatic adjustment of game difficulty. A representative plot of the game level adaptation for the two games for a particular patient is shown in Fig. 2. The top row depicts the game level chosen for the next trial at the end of the current trial; for example, at the end of trial number 7 for the CB game, the level for the 8th trial is increased from 1 to 2. We can see that the game adapted to the patient’s performance, ensuring the patient’s performance score was around the threshold (grey line in the bottom row of plots), thus continually challenging the patient during training.

The plot of game levels (top row) and game scores (bottom row) as a function of the trial number for the CB (left column) and FM (right column) games for a patient. The game levels shown in the top row correspond to the game level for the next trial. The grey line in the bottom row indicates the score threshold that defines a successful or failed trial. Three consecutive successful trials will increment the game level by 1, while three failed trials will decrement the game level by 1.
The plot of head movement kinematics during training for a patient and a healthy subject is shown in Fig. 3; these plots show the target and actual pitch/yaw angles for level 1 of both games. For the CB game (top two rows of Fig. 3), the patient’s movements (left column) were slower, resulting in lesser number of cardboard breaks (number of back and forth movements). In the FM game (bottom two rows of Fig. 3), the graph of the patient’s actual yaw angle was jerkier than that of a healthy subject. The summary of the movement performance for healthy subjects for all levels of the CB and FM games is shown in Figure S1 and Figure S2 in the in the Supplementary file, respectively. This normative data distribution can serve as a benchmark to evaluate patient performance in the differentgames.

Raw movement data for the CB and FM games. The grey traces in these subplots are the target angles,while the black traces are the actual pitch and yaw angles.
A comparison of the normative data with that of the patient data is depicted in the boxplots in Fig. 4 and Fig. 5; these boxplots use healthy subjects’ data only from the first three and four levels of the CB and FM games, respectively; the patient data had several outliers not displayed in the boxplots. Overall, the movement measures were all statistically different between patients and healthy subjects, except for “root mean square error” measure for the FM game.

Comparison of movement quality for the CB game between healthy subjects and patients. The comparison is made only using the first three levels of the CB game as the maximum level reached by patients was level 3. (‘**’ implies p < 0.001).

Comparison of movement quality for the FM game between healthy subjects and patients. The comparison is made only using the first four levels of the FM game as the maximum level reached by patients was level four. (‘*’ implies p < 0.05).
There is an increasing interest in the use of VR for the rehabilitation of vestibular disorders [5, 35]. Unlike all existing systems for vestibular rehabilitation, the VEGAS – a smartphone-based HMD – is affordable, compact, portable, and well suited to train a wide range of exercises (gaze, habituation, balance and also gait) in both clinics and patients’ homes. To the best of our knowledge, the VEGAS is the first smartphone-based HMD developed and tested for vestibular rehabilitation. Thus, the current study was focused on testing the usability of the VEGAS in a sample of healthy and patient populations.
Usability of the VEGAS
Overall, the results from the current study indicate that both healthy subjects and patients found the system to be highly usable, reporting an average SUS score of around 92 and 88, respectively. These results are very encouraging even though the current system is a preliminary lab prototype using: (a) a mid-range Android smartphone; (b) an affordable off-the-shelf headset; and (c) a set of fairly simple games. Given the increasing popularity of smartphone-based VR HMDs for gaming and entertainment, the coming years will see improved, highly customizable, and lightweight headsets; this will address the concerns related to the weight of the headset (P01 and P04 in Table S6 in the Supplementary file).
The current system has only two training games, which were played with an adaptive algorithm for automatic game difficulty adjustment. In general, patients did not have any complaints about the games, and some had verbally conveyed that they enjoyed the games and were interested in having the system for training at home. The game level selection algorithm adapted the game difficulty to keep the patient’s performance around the threshold for success/failure (Fig. 2), thus making the games challenging but achievable [6]. Based on the current study, one cannot draw any conclusions on whether patients will find the system engaging for long-term training (6–8 weeks). However, we strongly believe that with a more ergonomic headset, additional training games with appropriate feedback and progress tracking features, patients will find the system engaging even for longer unsupervised training.
Simulator sickness after VEGAS Training
Immersive VR environments are known to induce SS in healthy subjects [4, 17], whose after-effects can last a few hours following exposure. SS can lead to poor compliance, and the associated safety concerns can impede the acceptance of immersive VR systems for training. Thus, it was essential to evaluate the level of SS induced by VEGAS in both patient and healthy populations.
Following VEGAS training, the incidence rate for overall SS in healthy subjects was quite low (≈27%), indicating that the system and training were well tolerated by healthy subjects. On the other hand, patients reported a significantly higher incidence of SS (≈94%) following their training session. Given that the SS and vestibular dysfunction related symptoms overlap, the increased incidence rate is likely due to (a) the simulator, i.e., the nature of the VEGAS hardware and the VR environment; and (b) the head movement performed by the patients during training. The current study, however, does not allow us to identify the relative contribution of these two factors to the final SSQ score. One way to estimate the effect of the vestibular exercises on SSQ is to have the same group of patients train similar conventional exercises (without HMD) for 20 min in a single session. Changes in SSQ scores before and after conventional training would allow us to get an idea about the contribution of the exercises in inducing SS symptoms. Although this was not carried out in the current study, we plan to investigate this as part of our future work.
The VEGAS hardware, nature of the VR games, and the adaptive game algorithm, all play an important role in inducing SS or vestibular dysfunction related symptoms. Understanding the effect of all these factors can ensure the development of a safe and usable system for patients. Furthermore, understanding patients’ conditions and individualizing training can also ensure that therapy is challenging, well-tolerated, and safe.
Movement performance of healthy subjects and patients
Head kinematics was used to quantify the movement performance of healthy subjects and patients, which can help understand patients’ movement problems and monitor training. As expected, we observed that patients moved slower than healthy subjects in the CB game; their movement times were longer and had scored a lower number of cardboard breaks (third and fourth plots from the left in Fig. 4). Interestingly, patients appeared to have smoother and straighter movements than healthy subjects in the CB game; the absolute difference between the median values of movement smoothness are, however, quite small. We believe that this difference is due to a more cautious head movement strategy opted by patients, leading to slower, straighter, and smoother movements.
On the other hand, healthy subjects had focused on making fast movements to the different targets which could have slightly compromised their movement straightness and smoothness, because of overshoots and endpoint corrections. This is seen in the top row of Fig. 3, where the healthy subject appears to be making ballistic movements to the targets with overshoots. While the patient’s movements appear to have a “movement phase” towards the target, followed by a “slowing down” phase (the plateaus close to the target); the patient never overshoots the target, unlike the healthy subject. Such results have also been observed in other studies, where head movements of healthy subjects have more overshoots than that of patients for discrete movements [3, 19].
Limitations of the current system
The current version of the VEGAS is a preliminary prototype with several features that can be improved. Following are some of the major drawbacks identified for the system and the current study, which will be addressed by our ongoing work:
Conclusion
The current study presented the development and evaluation of the usability of an affordable smartphone-based HMD for vestibular rehabilitation. Based on a single session of testing on a sample of 15 healthy subjects and patients, we found the system to be highly usable. We also observed that a 20–30 min testing session with the system was well tolerated by healthy subjects, as evidenced by the low incidence rate of SS. Patients reported relatively higher rates of SS than healthy subjects. This could be the result of their condition, the nature of the HMD and/or the vestibular training with the system. Overall, we strongly believe that the smartphone-based HMD approach has significant potential to become an affordable, portable, and safe tool for vestibular rehabilitation. Future studies are essential to evaluate the long-term usability, therapy compliance, and efficacy of the system.
Declaration of interests
The authors declare that they have no competing interests. This research was funded by the Fluid Research Grant, Christian Medical College, Vellore, India.
Footnotes
Acknowledgments
Firstly, we would like to thank Arun Nehrujee for suggesting the idea for a vestibular rehabilitation device. We would like to thank the Institutional Review Board of the CMC Vellore for funding the project under the Fluid Research Grant scheme. We would also like to thank the clinicians in ENT Unit 4 at CMC Vellore for helping us to carry out the study at their outpatient facility. Finally, we thank Sadhana Yadav for proofreading the manuscript.
The reticle is the plus sign with a circle which is like the markings built into the eyepiece of a telescope, microscope, etc.