
Abstract
BACKGROUND:
Low success and high recurrence of benign paroxysmal positional vertigo (BPPV) after home-based self-treated Epley and Barbeque (BBQ) roll maneuvers is an important issue.
OBJECTIVE:
To quantify the cause of low success rate of self-treated Epley and BBQ roll maneuvers and provide a clinically acceptable criterion to guide self-treatment head rotations.
METHODS:
Twenty-five participants without active BPPV wore a custom head-mount rotation monitoring device for objective measurements. Self-treatment and specialist-assisted maneuvers were compared for head rotation accuracy. Absolute differences between the head rotation evaluation criteria (American Academy of Otolaryngology guidelines) and measured rotation angles were considered as errors. Self-treatment and specialist-treated errors in maneuvers were compared. Between-trial variations and age effects were evaluated.
RESULTS:
A significantly large error and between-trial variation occurred in step 4 of the self-treated Epley maneuver, with a considerable error in the second trial. The cumulative error of all steps of self-treated BBQ roll maneuver was significantly large. Age effect occurred only in the self-treated BBQ roll maneuver. Errors in specialist-treated maneuvers ranged from 10 to 20 degrees.
CONCLUSIONS:
Real-time feedback of head movements during simultaneous head-body rotations could increase success rates of self-treatments. Specialist-treated maneuvers can be used as permissible rotation margin criteria.
Introduction
Benign paroxysmal positional vertigo (BPPV) is a disease that affects the vestibular labyrinth of the inner ear due to the presence of loose canaliths migrating into semicircular canals [1]. Patients with BPPV experience brief episodes (5–30 seconds) of spinning dizziness, mostly after a sudden change in head posture [9, 21]. The Dix-Hallpike test and supine head roll test are common maneuvers to identify BPPV. Canalith repositioning procedures (CRPs) are performed depending on the canalith location in the three semicircular canals to reposition it back in the vestibule [6 , 18]. BPPV involving the posterior semicircular canal is the most prevalent type and is effectively treated with the Epley maneuver, a CRP [4]. The barbeque (BBQ) roll maneuver is used in BPPV to reposition canaliths of the horizontal semicircular canal, the second most common type of BPPV [11]. The success rate of CRP performed by physicians in clinics is over 90%; with a one-year recurrence rate of up to 30% [7 , 23]. Multiple treatment visits (up to 7) are required for complete symptomatic relief in > 25% of patients with BPPV [12, 16]. Maneuver repetition also shortens the duration of dizziness [15, 20]. Home-based self-treatment CRP may play a novel role in treating patients with BPPV [19], but its efficacy is questionable, with a much lower success rate compared to that of specialist-performed CRP in clinics [22]. Accurate CRP can be difficult for BPPV patients similar to new medical graduates [2], and wrong treatment can sometimes lead to emergency room visits for patients with BPPV [22].
The American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) guidelines recommend a standardized CRP based on our best anatomic understanding [3]. The guidelines specify arbitrary head rotation angles as 45-degree horizontal rotation and 20-degree head hanging during CRP [4]. Most recently, assistive systems based on these guidelines are proposed to improve the accuracy of self-treated Epley maneuver [6, 22]. However, the cut-off ranges of a clinically acceptable head rotation are still unclear, and there is a lack of quantitative analysis of head rotations performed during self-treated CRP. The present study aimed to find the characteristic patterns of inadequate treatments and to identify the causes of low treatment efficiency in self-treated CRP. The second aim was to set a geometrically measured clinically acceptable range of head rotation for each step of the Epley and BBQ roll maneuvers, which is especially important for building a device that can guide self-treated CRP, our proposed next study. It was assumed that the absolute mean error range of the specialist-treated CRP in the present study could be applied as the clinically acceptable range of the assistive device.
Methods
Participants
This prospective single-institution study was ap-proved by the institutional review board of Seoul National University Hospital (IRB No. H-1412-012-630). Twenty-five adults (24 females, 1 male) with a mean age of 54.2 (range: 23–66) years were enrolled between June and December 2018. Written informed consent was obtained from each participant, and the recruited participants had not experienced any disease or surgery that could induce positional vertigo. None of the participants had prior knowledge about BPPV or CRP. For analysis of the age effect, participants were divided into an older group (age ≥60 years, N = 15) and a younger group (age < 60 years, N = 10). The mean age [SD] for both groups was 63.7 [1.6] years and 39.9 [7.5] years, respectively.
Interventions
Participants sat on a bed after wearing the head motion tracking (HMT) device. We provided the handout describing the Epley maneuver, and the participants were allowed as much time as required to understand the maneuver. Once a participant fully understood the procedure, they performed the maneuver twice by themselves. They were also allowed to refer to the handout anytime as required. An instructor provided a brief explanation and demonstration of incorrect steps during the first trial. The head movements during the self-treated Epley maneuver were quantitatively recorded in 3-dimensional rotation angles (roll, pitch, and yaw) using the HMT device. After finishing the self-treated Epley maneuver, a specialist (otologist or vestibular technician with > 10 years’ experience) performed the standard Epley maneuver in the participant twice. The head movements during specialist-treated Epley maneuvers were also recorded with the same HMT device. The above procedure was followed for the BBQ roll maneuver.
Head motion tracking device
We developed a head-mounted device enabling HMT, as shown in Fig. 1a. The HMT device was small and lightweight, measured 36 mm×39 mm×14 mm and weighed 16 g. The size enabled it to be attached to the forehead on a head-mounted strap. An attitude heading reference system (AHRS) (EBIMU-9DOFV4; E2BOX, Korea) was adopted to provide the head rotation angles in three axes. The AHRS comprised an inertial measurement unit (IMU) with 9-axis degrees of freedom (a 3-axis accelerometer, a 3-axis gyroscope, and a 3-axis magnetometer). An attitude heading reference system that we implemented guaranteed 0.2 degree for roll and pitch and 0.5 degree for yaw in terms of the maximum error of static accuracy. The sampling rate was set to 250 Hz, and the data was transmitted to a laptop via Bluetooth.

(a) Laboratory-Developed Head Motion Tracking Device, (b) Rotational Matrix.
To calculate the 3-dimensional rotation angle for each step of the maneuver, we applied the rotation matrix providing the coordinate transformation with the Euler angles in terms of three moving axes [13]. As shown in Fig. 1b, this 3×3 matrix can represent sequential rotations of three axes with the actual rotation axis and its rotation angle. The rotation matrix
The angle of head rotation for each step mentioned in the AAO-HNS guidelines was set as the gold standard [4]. The actual head rotation angle for each step was calculated with respect to the final position in the previous step. The definition of mean error (in degree) was the average of all differences (i.e., errors) between the gold standard and the actual head rotation angle calculated by the IMU sensor data and the rotational matrix. The “absolute mean error” was defined as the average of absolute values of all differences (i.e., errors). The absolute mean error was mainly applied as the metrics for the performance evaluation to prevent that the positive and negative errors cancel each other when comparing the mean values. In addition, the mean error with the standard deviation was calculated to observe how the self-treatment leads to errors of angles when comparing to the specialist-treatment.
In the Epley maneuver (treating the right ear), participants sat on a bed and turned their head 45 degrees to the right, which was the starting position (Fig. 2a). Next, they laid back keeping their head turned and reclined the neck 30 degrees over the edge of the bed (step 2). They held this position for one minute. The third step involves turning their head 90 degrees to the left without raising it (step 3) followed by a one minute wait. In the fourth step, participants rolled their head and body 90 degrees to the left side (step 4) and waited for another one minute. The face was directed toward the ground diagonally in this step. Finally, they sat up on the left side (step 5). The accuracies of the second to fourth steps were evaluated by the criteria of the rotation angles and directions, which were 120 degrees backward (step 2), 90 degrees leftward (step 3) and 90 degrees leftward (step 4), respectively.
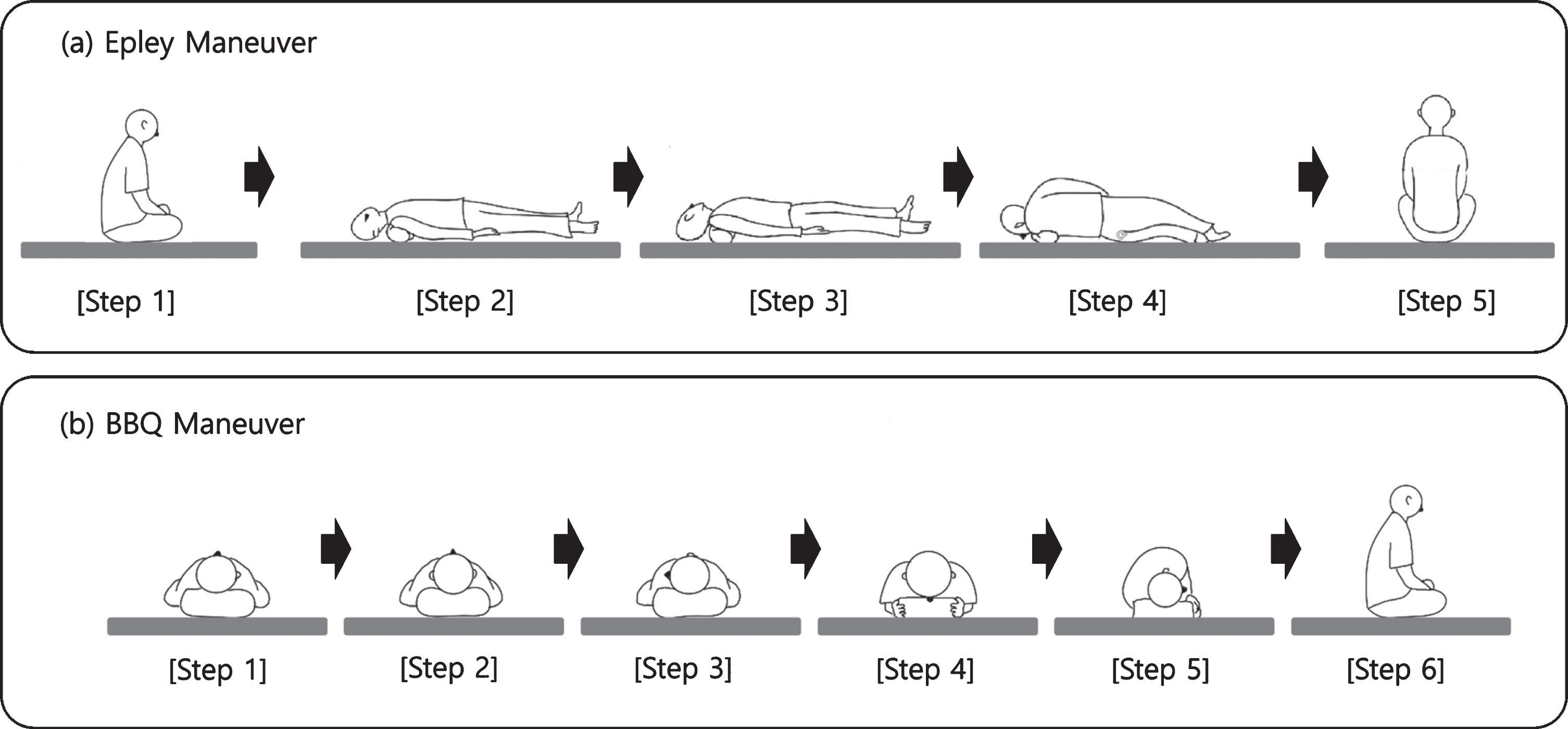
(a) Epley Maneuver Procedure, (b) BBQ Roll Maneuver Procedure.
In the BBQ roll maneuver (treating the right ear), participants started in the supine position turning their head 90 degrees to the right on the pillow (Fig. 2b). Because the horizontal canals are tilted upward by 25.12±5.62 degrees from the horizontal plane [5], a solid pillow was used to align the horizontal canals vertically with the ground. The participants then turned their head 90 degrees to the left maintaining the supine position (step 2). Subsequently, they turned their head another 90 degrees to the left (step 3). In the fourth step, they laid their face down by turning the head 90 degrees and rolling their body 180 degrees to the left (step 4). Next, they rolled their head and body another 90 degrees to the left and lay on their right shoulder (step 5). They were back to the supine position in the final step. The evaluation criteria of the rotation angles and directions were 90 degrees leftward for all steps.
To prevent neck hyper extension, we designed three different heights (7, 9, and 11 cm) of pillows that can be prescribed specifically for each participant (Fig. 3). That is, if the participant is tall and/or skinny, a 11 cm high pillow can be prescribed to put under his or her shoulders. If the participant is short and/or obese, a 7 cm high pillow can be prescribed to put under his or her shoulders. Regardless of the patient’s physical condition, the participant’s head will be supported on the floor (or bed) so that extending the neck more than the planned angle is not possible.
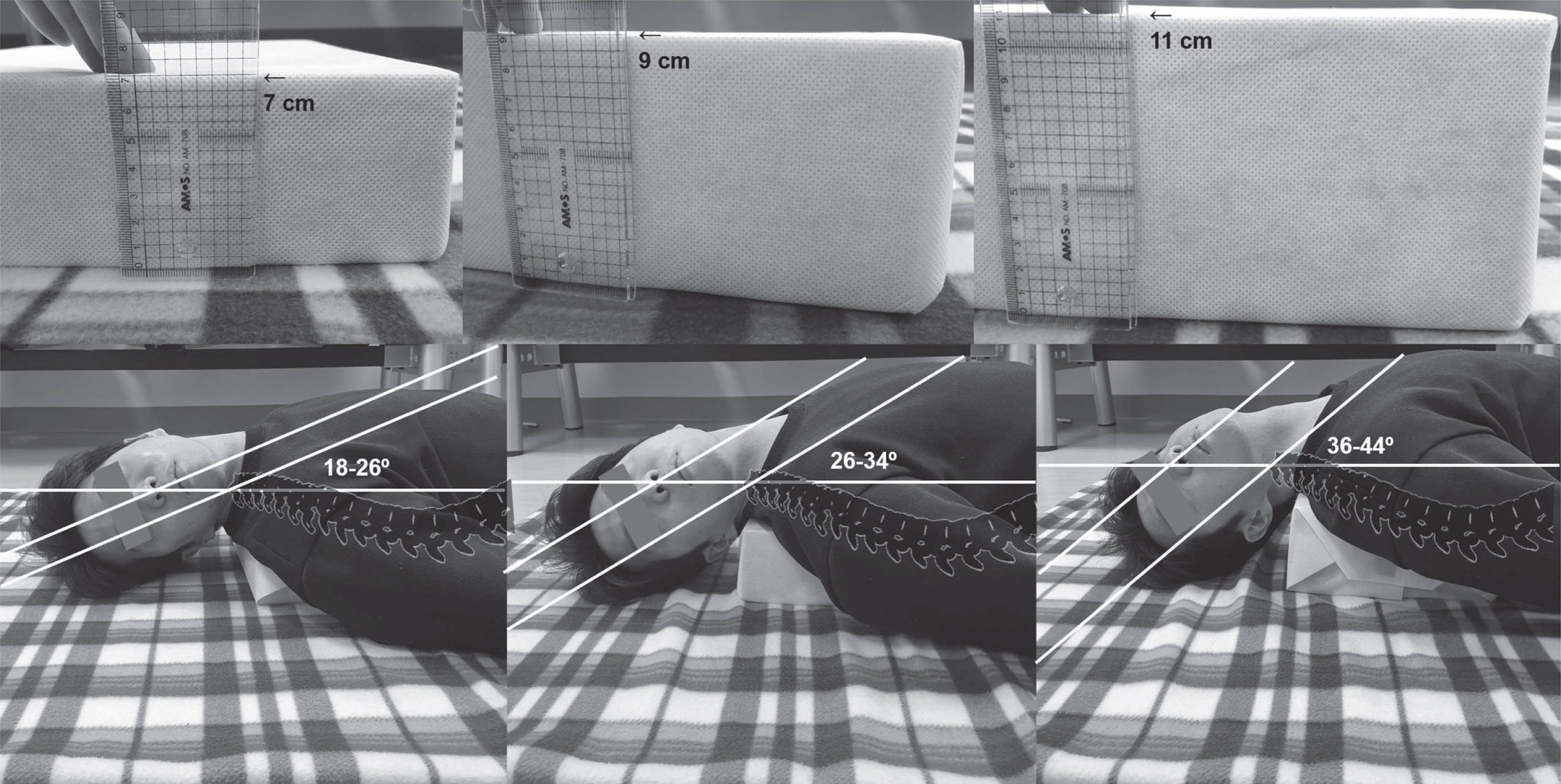
Three pillows under the shoulder with different heights (7, 9, and 11 cm) for the device-guided Epley maneuver.
Independent t-tests using SPSS Statistics 24.0 (SPSS Inc., Chicago, IL) were performed to compare the accuracy between self-treated and specialist-treated maneuvers using the absolute mean errors of two trials. Moreover, independent t-tests between self-treated and specialist-treated maneuvers using the mean errors were performed to observe how the self-treatment leads to rotation angles. We also conducted independent t-tests between first and second trials to evaluate the effect of trial order on the performance, especially for self-treated maneuvers. For analysis of the age effect, a one-way ANOVA was performed for three groups (self-treated young, self-treated old, and specialist-treated group) following which independent t-tests were used for post hoc pairwise comparisons with Bonferroni’s correction.
Results
Self-treated vs. Specialist-treated canalith repositioning procedures
Figure 4 shows a scatter plot of all measured angles with the nominal angle for each step in Epley and BBQ maneuvers. The mean errors in step 2, 3, and 4 of the self-treated Epley maneuver were –8.4 [24.1], –35.5 [27.8], and –39.8 [38.7] degrees, respectively. The mean errors in step 2, 3, and 4 of the specialist-treated Epley maneuver were –5.2 [23.6], –19.0 [20.3], and 7.1 [15.8] degrees, respectively. The mean errors in step 2, 3, 4 and 5 of the self-treated BBQ maneuver were –20.8 [24.5], –27.8 [19.8], 20.2 [21.4], and 21.0 [19.5] degrees, respectively. The mean errors in step 2, 3, 4, and 5 of the specialist-treated BBQ maneuver were –10.6 [12.7], –6.9 [11.5], 14.7 [10.6], and 4.5 [10.7] degrees, respectively. There was a significant difference in Epley maneuver step 3 (95% CI –26.1% to –6.8%; P < 0.05) and 4 (95% CI –58.7% to –35.1%; P < 0.001). In the case of BBQ maneuver, there was significant difference in step 2, 3, and 5 (95% CI –18.0% to –2.4%; 95% CI –27.3% to –14.4%; 95% CI 10.2% to 22.7%; all P < 0.05).

A scatter plot of all measured angles in Epley and BBQ maneuvers. The solid lines indicate the nominal head rotation angle based on American Academy of Otolaryngology guidelines [4].
Figure 5 displays the absolute errors of self- and specialist-treated maneuvers. When comparing the self- and specialist-treated Epley maneuvers, there was a significant difference in step 3 and 4 (95% CI 8.7% to 22.5%; 95% CI 31.5% to 44.2%; all P < 0.001). The absolute mean errors [SD] in step 3 and 4 of the self-treated maneuver was significantly larger (40.0 [20.5] and 51.5 [20.1] degrees respectively) than that of the specialist-treated maneuver (24.4 [13.1] and 13.7 [10.4] degrees respectively). The absolute mean errors of the self- and specialist-treated maneuvers in step 2 were 21.9 [12.9] and 18.3 [15.6] degrees, respectively. Smaller absolute mean errors were found in the specialist-treated maneuver, but the differences were not statistically significant in steps 2.
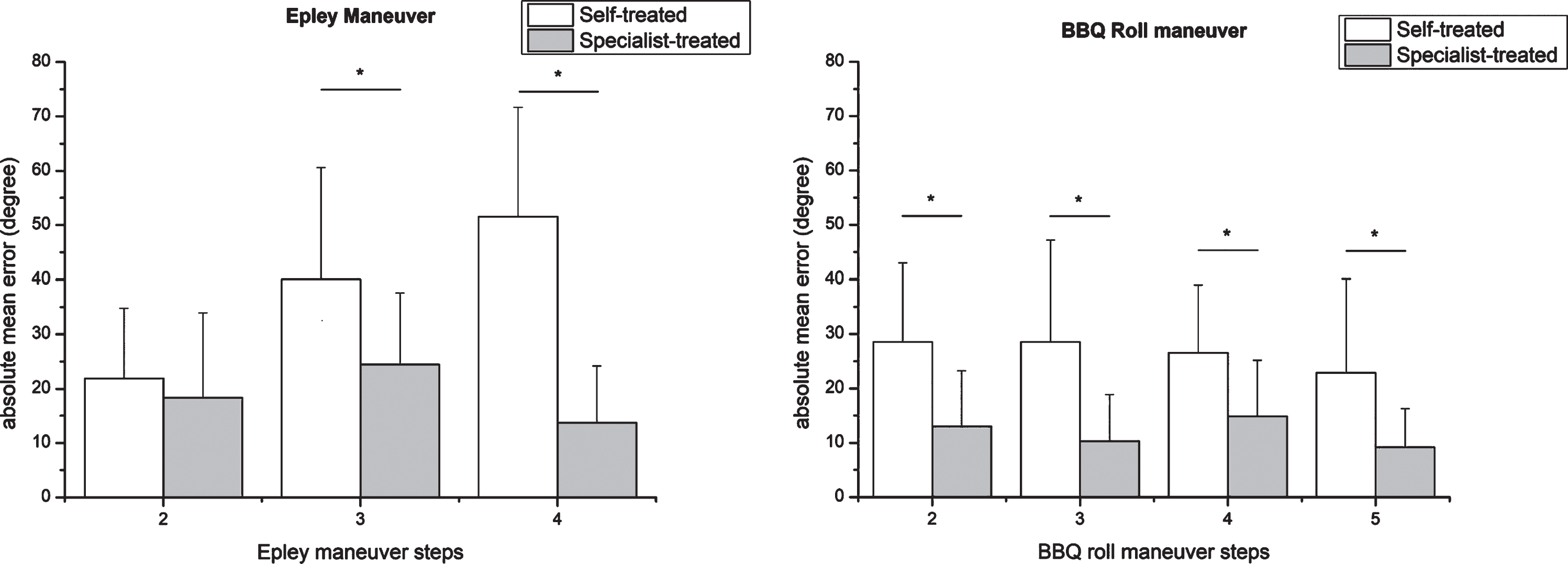
Absolute Errors in Self- and Specialist-treated Maneuvers (Mean and Standard Deviation).
For the BBQ roll maneuver, significant differences were found in steps 2, 3, 4, and 5 (95% CI 10.6% to 20.5%; 95% CI 12.5% to 24.0%; 95% CI 7.1% to 16.2%; and 95% CI 8.5% to 18.9%; all P < 0.001) between the self- and specialist-treated maneuvers. The absolute mean errors [SD] of the self-treated maneuver in steps 2, 3, 4, and 5 were 28.6 [14.4], 28.6 [18.6], 26.5 [12.5], and 22.9 [17.2] degrees, respectively. The absolute mean errors of the specialist-treated maneuver at steps 2, 3, 4, and 5 were 13.0 [10.2], 10.3 [8.6], 14.9 [10.3], and 9.2 [7.1] degrees, respectively. The range of absolute mean error differences was 11.6 to 18.3 degrees where self-treated maneuver always showed greater error compared to the specialist-treated maneuver in every step.
When comparing the self-treated younger group, self-treated older group, and the specialist-treated group; a one-way ANOVA revealed significant differences between the three groups in step 3 and 4 of the Epley maneuver (F(2, 97) = 11.2; F(2, 97) = 70.1, all P < 0.001). In the post hoc pairwise comparisons with Bonferroni’s correction, the specialist-treated group displayed a significantly lower absolute mean error [SD] of 24.4 [13.2] degrees than the self-treated younger group (44.1 [17.2] degrees) as well as the self-treated older group (37.3 [22.3] degrees) at step 3. In step 4, the specialist-treated group displayed a significantly lower absolute mean error [SD] of 13.7 [10.4] degrees than the self-treated younger group (48.9 [23.2] degrees) as well as the self-treated older group (53.3 [18.0] degrees). However, there was no significant difference between the self-treated younger and older groups in both steps.
For the BBQ roll maneuver, significant differences between the three groups were found in all steps (Table 1). The pairwise comparisons confirmed that absolute mean errors of the specialist-treated group were significantly lower than those of self-treated younger and older groups in all steps. When comparing the self-treated younger and older groups, there was significant difference in step 3 (95% CI –23.6% to –4.3%; P = 0.002). The absolute mean error of the self-treated older group was 14.0 degrees greater than that of the self-treated younger group.
Statistical comparison results of specialist-treated, self-treated younger, and self-treated older groups
Statistical comparison results of specialist-treated, self-treated younger, and self-treated older groups
When comparing first and second trials in the self-treated maneuvers, a significant difference was found only at step 4 of the Epley maneuver (95% CI 0.1% to 22.3%; P = 0.048). The absolute mean errors [SD] of the two self-treated trials were 57.1 [19.5] and 46.0 [19.5] degrees. There was no significant difference between first and second trials in the specialist-treated trials in any of the steps. The absolute mean errors of the two specialist-treated trials were 13.7 [10.6] and 13.8 [10.4] degrees for step 4. For the BBQ roll maneuver, significant differences were not found between first and second trials in both self-treated and specialist-treated maneuvers.
Discussion
When quantitatively measured with IMU sensors, the head rotation in the self-treated CRP was significantly inaccurate and variable than that in the specialist-treated CRP. In the comparison with the mean error, self-treated Epley Maneuver tended to rotate less than the specialist-treated Epley maneuver at step 3 and 4. Similarly, in BBQ maneuver, participants had a tendency rotating less than the specialist-treated at step 2 and 3. In the step 4 of BBQ maneuver, rotation angle of the self-treated case was larger than the specialist-treated case. In this step, participants easily followed the instruction to rotate their body to the left and look toward the floor, which caused the larger rotation angle due to the insufficient rotation of previous step in the self-treated.
In the comparison with absolute mean errors, the absolute mean error at step 3 of the self-treated Epley maneuver was 15.6 degrees worse compared to that of the specialist-treated Epley maneuver, and the absolute mean error at step 4 of the self-treated Epley maneuver was 37.8 degrees worse compared to that of the specialist-treated Epley maneuver. Since the absolute angles in the frame of reference was not used, it seems less likely that there was an accumulation of error from step to step. The absolute mean error of step 4 (Epley maneuver) was largest, because this position was challenging especially to elderly subjects, not because the absolute mean error accumulated. Thus, step 4 is the crevasse of self-treated Epley maneuver, which makes the treatment outcome inferior to that of specialist-treated Epley maneuver. Participants were confused about how to turn the body 90 degrees while maintaining the head position of the previous step (step 3). They tended to move the head toward the front of the body. For self-treated BBQ roll maneuvers, the absolute mean errors of steps 2, 3, 4, and 5 were 11.6 to 18.3 degrees worse compared to that of the specialist-treated BBQ roll maneuver. Every step (2, 3, 4, and 5) of BBQ roll maneuver may be responsible for low treatment efficacy in self-treated CRP. Even though participants were likely to understand the procedure more easily than Epley maneuver, they had difficulty in rotating the head a full 90 degrees on a pillow in supine position. Although they thought that they turned their heads to the affected side as much as possible, the actual rotation angles were below 90 degrees, which cumulatively decreased the rotation angle to below 90 degrees at the second step. Some participants felt discomfort due to the tension around the neck and shoulder when rotating a full 90 degrees on the pillow in specialist-treated maneuvers.
For the same reason, participants had difficulty rotating the head 90 degrees in supine position at the third step, especially those in the older group. Inaccurate head movement during self-treated CRP was especially problematic in elderly subjects who had limited range of motion in the head and neck. Currently, there are two different guidelines for the first and third steps of the BBQ roll maneuver. The type we chose involved rotating the head 90 degrees to the right or left in supine position [8, 11]. The other involves rolling the body 90 degrees to the right or left while keeping the head straight ahead [14, 24]. For the BBQ roll maneuver at home, the second type of guide would be preferred for better rotation accuracy, especially in the elderly.
The geometrically measured clinically acceptable ranges of head rotation for Epley maneuver were 18.3 [15.6] (step 2), 24.4 [13.2] (step 3), and 13.7 [10.4] (step 4) degrees, based on the specialist-treated Epley maneuver. They were 12.1 [10.2] (step 2), 10.3 [8.6] (step 3), 14.9 [10.3] (step 4), and 9.2 [7.1] (step 5) for the BBQ roll maneuver. We found that absolute mean errors of the specialist-treated CRP were usually larger for Epley maneuver (approximately 20 degrees) compared to that of BBQ roll maneuver (approximately 10 degrees). Several previous studies have reported successful assistive tools for treating BPPV. Tabnafar et al. developed and validated a smartphone-based virtual reality system guiding the Epley maneuver [15]. Organ et al. reported the efficacy of a smartphone application to help family physicians perform the Epley maneuver [17]. These tools are significantly beneficial; however, the correctness of head movements was evaluated using subjective scores rated by expert observers. Our study can provide the quantitative criterion of each step based on the rotation angles of the CRP performed by two specialists. To our knowledge, there is no study evaluating the step-by-step performances of self- and specialist-treated CRP by objective measures. The geometrically measured clinically acceptable range of head rotation during CRP, which is approximately 10–20 degrees depending on steps, can be used when building a device that can guide self-treated CRP.
Limitations
Our study has several limitations. First, because our study was conducted with participants without active BPPV, the effect of head rotations with low accuracies on BPPV treatment was not investigated. Future research is required to monitor changes in nystagmus and vertigo according to the performance evaluation of the maneuver. Next, the participants in this study were mostly females. A 39-year-old male participant showed greater accuracy especially at the fourth step of the Epley maneuver and the second step of the BBQ roll maneuver. However, it is difficult to determine the effect of gender due to lack of male participants with broad age ranges in the current study. To our knowledge, there is no study investigating the effect of gender on the performance of maneuvers in BPPV treatment.
Conclusion
The lower success rate of the self-treated CRP is due to the significantly inaccurate and variable nature of simultaneous head and body rotations during step 4 of the Epley maneuver. In the self-treated BBQ roll maneuver, the lack of head rotation in supine position cumulatively decreases its overall accuracy. Thus, there is a need for assisted guiding of head movements in real-time to increase the success rate of self-treated CRP. Also, the margins of head rotation quantitatively measured during specialist-treated CRP may serve to set a range of flexibility when building assist devices.
Footnotes
Acknowledgments
No competing interests exist.
This research was supported by the Korea Health Industry Development Institute (KHDI) of the Ko-rean Ministry of Health and Welfare (HI18C0626).