
Abstract
BACKGROUND:
The efforts to achieve better functional results in vestibular rehabilitation have been continued by using different visual and somatosensory stimuli for a long time. Whole-body vibration (WBV) is a mechanical vertical stimulation that provides high frequency vibration stimulus to the proprioceptive receptors. Biofeedback provides continuous information to the subject regarding postural changes. These techniques may aid to improve vestibular rehabilitation.
OBJECTIVE:
We aimed to investigate the effect of adding WBV or biofeedback postural training (BPT) to standard rehabilitation exercises in patients with chronic unilateral vestibular weakness.
METHODS:
Ninety patients were randomized into three groups. Group 1 had WBV and Group 2 BPT in addition to the standard rehabilitation exercises. Group 3 only carried out the home-based exercises and served as the control. Outcome measures such as static posturography, Berg Balance Scale, Timed Up-and-Go test, Visual Analog Scale, and Dizziness Handicap Inventory (DHI) were used for comparison.
RESULTS:
Statistically significant gains were achieved in all groups with all parameters at the end of treatment when compared to baseline (p < 0.05). The patients in Group 1 (WBV), however, were significantly better than those in Groups 2 and 3 at the static posturographic stability score, Berg Balance Scale, and DHI (p < 0.05).
CONCLUSION:
Adding WBV to a rehabilitation program may be an effective strategy to improve postural stability and achieve better physical, functional and emotional outcomes.
Introduction
The vestibular rehabilitation program is an essential part of vertigo treatment. Patients with either ac-ute or chronic vestibular failure require special care to return to their daily routine. There is strong evidence that vestibular rehabilitation is effective, particularly in unilateral peripheral vestibular dysfunction [28]. In 2015, Hillier et al. suggested that there is insufficient evidence to answer the question “what kind of rehabilitation was more effective?” [28].
Several factors, including age, physical and psychological conditions, comorbid disease, and the type of dysfunction affect the outcome. Therefore, not all patients achieve the expected benefits [23]. Different rehabilitation techniques have been proposed to overcome this issue. These range from simple booklets to high-end technological virtual reality solutions [45]. Most depend on different visual and somatosensory stimulation methods. Moving targets, lights, and videos are used for eye stability, and soft surface or moving platforms are used for postural stability. Following the introduction of moving platforms, there have been no new developments in stimulating the proprioceptive system; exercises have been the preferred tool [44]. Whichever technique is used for rehabilitation, the expected result is the compensation of the functional deficit by the unaffected parallel systems in the CNS. The primary factor in this context is input. Lack of input to the vestibular system causes a delay in compensation. In contrast, better functional results will be achieved in a shorter period of time as the variety, frequency and quality of the inputs are increased [24].
In our clinic, we have shown that even simple exercises are effective for balance control [40], but occasionally it is difficult to convince patients to comply with home-based exercises. We observed that the physical condition of the patient is important in co-mpliance to exercises as the majority of balance exe-rcises require active participation from the patients. The second factor that we observed to affect compliance was the psychogenic profile of the patient;∼45%had an abnormal score on the Symptom Checklist Inventory [7]. Therefore, continuous support and fun are important during the exercises. To overcome these issues, we are continuously looking for new hospital-based programs to support vestibular exercises. In this study, we investigated two additional techniques: whole-body vibration (WBV) and biofeedback postural training (BPT).
We hypothesized that if we increased input to the proprioceptive system and forced the antigravity muscles, we may achieve improved functional outcome in patients with unilateral vestibular weakness. WBV is a mechanical vertical stimulation that provides high frequency vibration stimulus to the proprioceptive receptors [31]. It is a technique used to improve bone density and muscle strength in postmenopausal females [26], and has been reported to improve neuromuscular performance [2]. Vibration is oscillating mechanical energy transferred from a generator to the body via a platform [33]. The human body acts like a spring and stores mechanical energy; when the body is going upward with the stimulus, energy is stored, and when the body is going down with gravity, energy is released. During these movements, muscles, tendons, and joints work together to manage the energy flow through the body. The CNS also receives proprioceptive input during the movement. It is using the natural proprioceptive pathways and not only changing the weight of proprioceptive inputs on the vestibular system but also increasing strength, flexibility, and control of the muscles and joints [15]. Some researchers have used vibration stimulus via a belt system to improve balance [10, 22]. This device detects the oscillations of the body and provides vibrotactile feedback to the patient. Providing an external additional stimulus, such as postural feedback, is a different rehabilitation strategy.
Biofeedback is an important technique used in neuromuscular rehabilitation. Regardless of the mode applied, when used in balance rehabilitation, the pat-ient is continuously informed of postural changes. It has been found to improve balance training in stroke patients, compared with conventional exercises, and patient compliance was also better with biofeedback training [25]. Similar results have also been reported in parkinsonism [14]. Previously, visual, auditory, and vibrotactile feedback stimuli were used, but bio-feedback may be the effective solution for patients with concentration and emotional difficulties.
The aim of this research was to evaluate the eff-ectiveness of WBV and BPT as add-ons to vestibular exercises in patients with chronic unilateral vestibular weakness (CUVW). We proposed that additional peripheral inputs from proprioceptive receptors wo-uld improve the musculoskeletal system, in particular antigravity muscles, and also alter the preferred vestibular system input, resulting in improved ves-tibular rehabilitation outcomes compared with the conventional rehabilitation programs.
Materials and methods
Patients with CUVW and persistent dizziness for more than 3 months were divided into three interventional groups. The groups all had home exercises as a baseline standard vestibular rehabilitation. Group 1 had WBV and Group 2 did BPT sessions in the hospital as additional interventions. Group 3 had no additional intervention (Control) (Fig. 1).
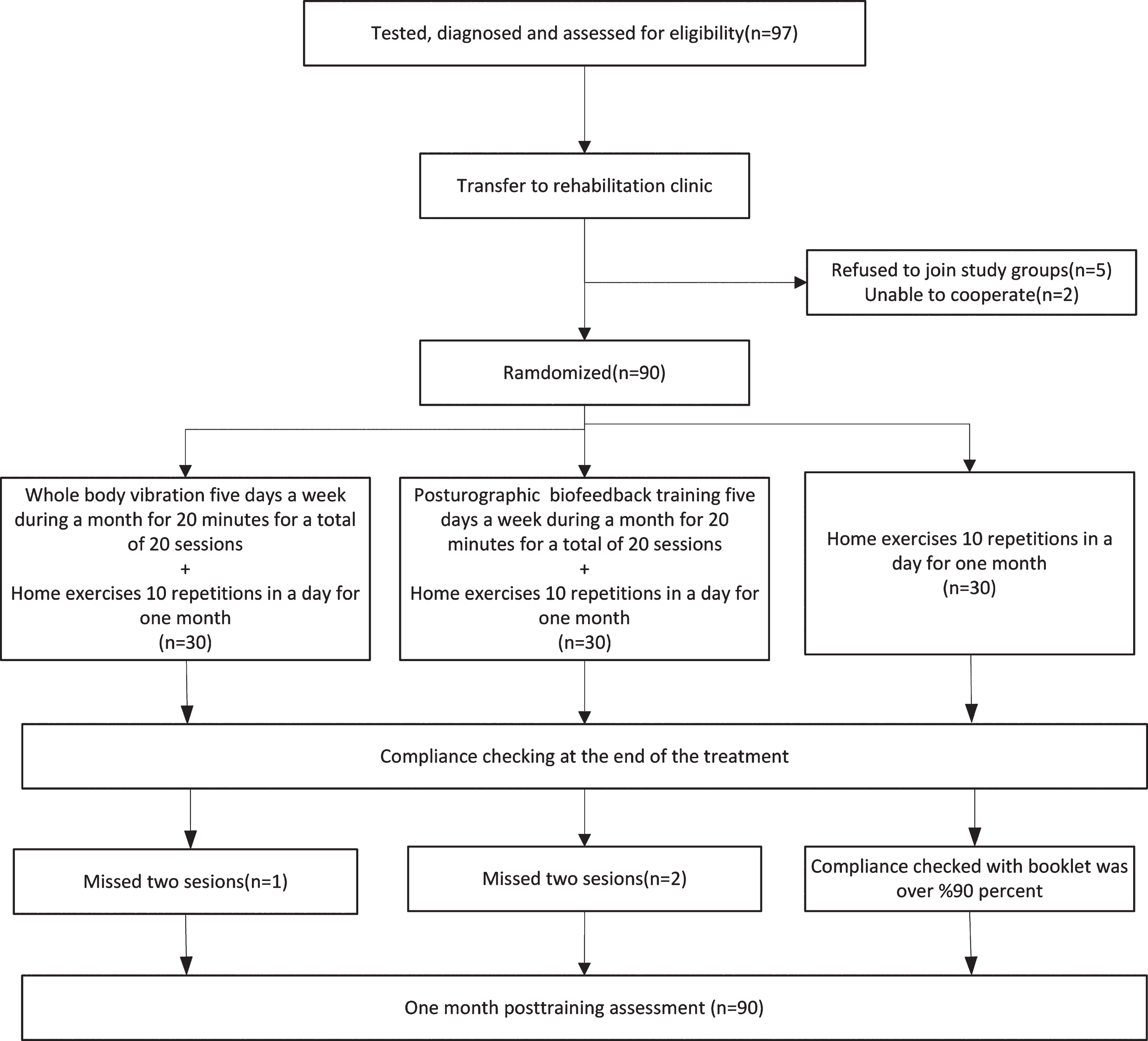
Randomization of groups and interventions.
Ninety-seven consecutive adult patients with CUVW and persistent dizziness for more than 3 months were screened for eligibility and 90 were included in this prospective, randomized controlled study over a 2-year period. The patients were randomly divided into three groups using random number tables. Each group consisted of 30 patients.
All patients were first seen in the otolaryngology clinic, where demographic information and detailed medical histories were collected, and physical examinations carried out. All patients received a comprehensive assessment including pure tone aud-iometry, videonystagmography, static posturography, and MRI. Patients with bithermal caloric test results showing weakness of the horizontal canal > 30%were categorized as unilateral vestibular weakness (Chartr VNG, ICS Medical, and USA). Those with neurological or psychiatric disease, bilateral vestibular weakness, recurrent vestibulopathy, benign parox-ysmal positional vertigo, or orthopedic problems in the lower extremities were excluded from the study. Patients with severe visual and hearing impairment were also not suitable for the study. Following the differential diagnosis, patients who fulfilled the inclusion criteria were transferred to the rehabilitation clinic. All participants were informed regarding the procedure and provided written informed consent. Permission was obtained from the University Ethics Committee (60116787-020/20944).
Intervention
A home-based vestibular rehabilitation program, including vestibular adaptation exercises, oculomotor exercises, static and dynamic balance exercises was given to each group in the form of a booklet [40]. The exercises were demonstrated and performed for the first time at the hospital, under supervision. The booklet provided descriptions and images of each exercise to enable the patients to perform the exercises at home. Ten daily repetitions of the exercises were to be performed and the patients were asked to record their performance on a chart. The diary was used to monitor adherence to the program for a period of 1 month.
BPT, as an adjunct to the home-based exercises, was carried out 5 days a week for a month, using a Tetrax® (Sunlight Medical Ltd) static posture analysis device. Each session lasted 20 min and there were a total of 20 sessions. The BPT included “catch, speedball, sky ball, gotcha” exercises, which require the patient to follow a visual target during weight transfer movements, capturing fast-moving objects by changing the center of gravity, or quickly escaping from incoming objects [3, 14]. There was a 30-s pause between each exercise.
WBV training was also carried out 5 days a week for a month. Twenty sessions, each lasting 20 min, were performed over the month using a Power Plate Pro 5 (MDD CE 0086, Performance Health Systems, Northbrook, IL, United States), which is a vertical vibration device. The patient moved between bilateral lunge (single leg position), partial squat, and deep squat positions, whilst a 35 Hz frequency, 2 mm vibration amplitude was applied over five sets, with a 30-s rest period between each set [9, 39]. Positions that were effective on the calves, quadriceps, hamstrings, abdominals, lower back, and buttocks were selected. In the first lunge position, patients placed the right leg with a 70° flexion in the hip and 90° flexion in the knee on the platform, and the left leg on the ground. In the second lunge position, patients placed the left leg with a 70° flexion in the hip and 90° flexion in the knee on the platform, and the right leg remained on the ground. In the third position, both legs were on the platform, and the patient performed a mini squat (120° angle at the knee). In the fourth position, the patient performed a 70° squat on the platform. In all positions, the patient held onto the safety handles. Each vibration position was held for 30 s, with a 30-s rest between each position. The WBV training program consisted of five sets of four vibration positions with 30-s exercises and 30-s rest between each vibration position. A total of five sets was carried out in one session.
Outcome measures
At the start and end of the study (1 month), all par-ameters were observed by a doctor who was blinded to the study groups.
Static posturography was used to assess postural function (Tetrax Interactive Balance System, Sunlight Medical, Tel-Aviv, Israel). Patients were evaluated in eight different positions and measu-rements were made on soft/hard surfaces, with eyes open/closed, head turned right/left, head tilted up/ down (Fig. 2). Changes in stability, weight distribution, and sway were measured. All measurements were used to calculate a total stability score (It is named as “fall index” by the company), between 0 and 100; 100 represents extreme risk of falling. The calculation method and standing positions have been described previously [4, 14]. The calculated stability score indicates the functional postural stability of the patient. Its test-retest reliability was shown in young adults [1] and was found to correlate well with clinical balance tests in the elderly [5].
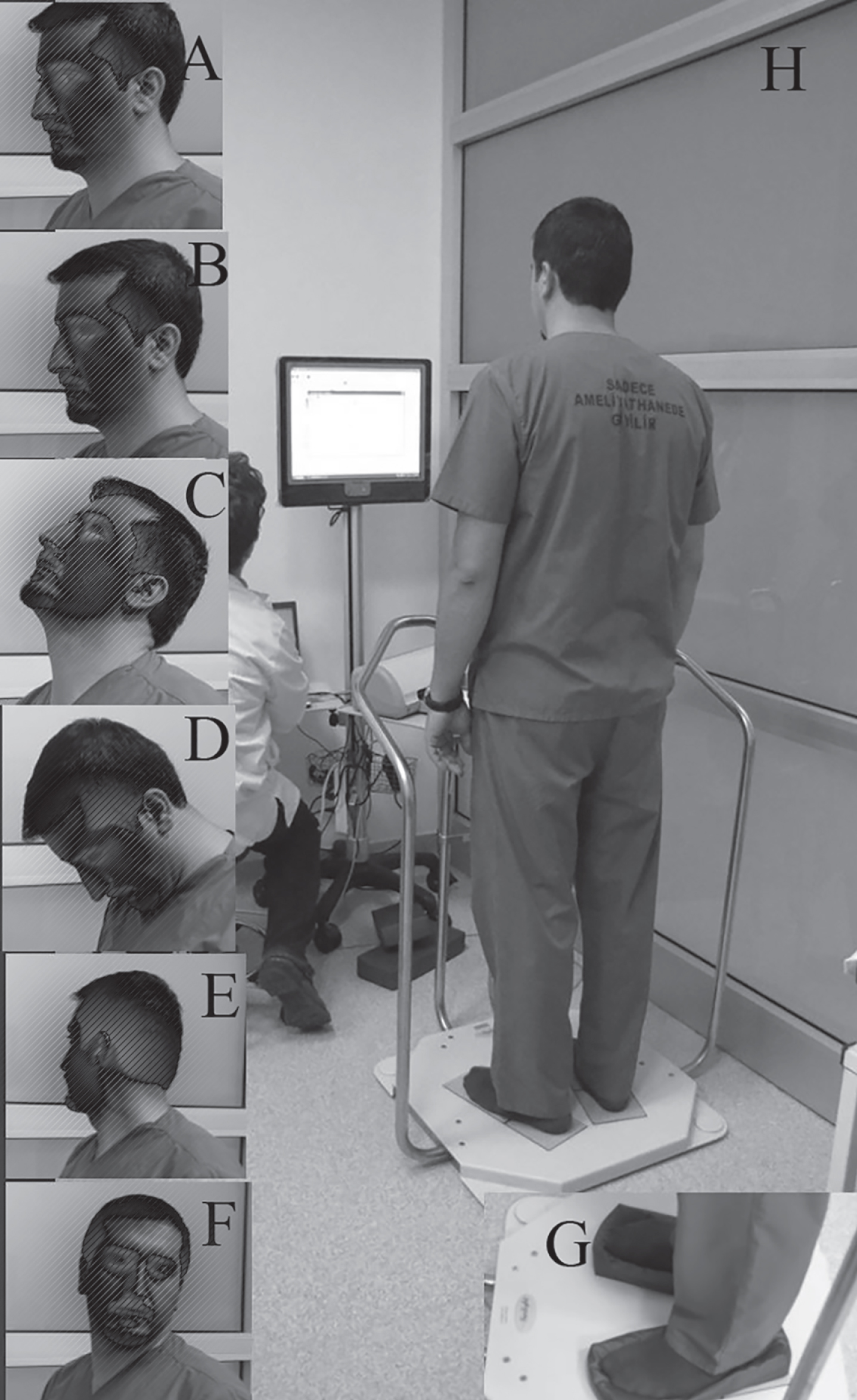
Calculation of total stability score(fall index) in Tetrax. The standard examination consists of eight positions. Same instrument was also used for biofeedback training A. Two positions,eyes open, head straight on soft and hard surface. B. Two positions, eyes closed, head straight on soft and hard surface C. Eyes closed, head tilted up on hard surface.D. Eyes closed, head tilted down on hard surface. E. Eyes closed, head turned right on hard surface. F. Eyes closed, head turned left on hard sürfece G. Example of soft surface. H. Testing equipment and position of the patient.
The Berg Balance Scale (BBS) consists of 14 tasks, each of which is scored on a scale from 0–4. The possible highest score is 56, and indicates no balance difficulty. The Turkish version of the BBS has been shown to be reliable and valid [36].
The Standard Timed Up and Go test (TUG) is a widely used balance and gait index based on the time taken to complete a specific task. Standard and expanded versions are described in detail in the literature [42]. First the procedure was described to the patient, then patient did a test trial. After that we recorded the time for one trial.
A 10-point scale was used for the Visual Analog Scale (VAS), where 0 points corresponds with “no vertigo”, and 10 points with “the worst vertigo”. Patients marked a point on the 10-cm vertical line according to the severity of their vertigo.
The Dizziness Handicap Inventory (DHI) was developed to assess the level of handicap associated with vertigo [20]. It consists of 25 items, sub-grouped into three domains: functional, emotional, and physical. There are three closed-form answers where patients can answer: “yes”, “sometimes” or “no” with the corresponding scores of 4, 2, and 0. The Turkish version of the DHI has been adapted and validated previously [13]. We used only total score because because different factor analyses reveal different clusters each time [8].
When the effect size of VAS scores in 15th and 45th days(dz = 1.87; dz = 2.21) in the reference study was considered, the sample size was calculated as 78 patients(at least 26 patients each group) to determine an acceptable the VAS score difference(dz = 0.6) between groups with a power 90%at 95%confidence level [40].
SPSS version 22.0 (Statistical Package for the So-cial Sciences Inc., Chicago, IL, USA) was used for statistical analysis. The Kolmogorov-Smirnov test was used to analyze normal distribution, and as the distributions were not normal, nonparametric tests were used for statistical evaluation. The significance of pretreatment and post-treatment improvements were assessed using the Wilcoxon signed-rank test. Demographic characteristics are shown as mean, with standard deviation, and rates. For continuous variables, the significance of the differences was analyzed using the Kruskal-Wallis variance analysis while categorical variables were analyzed with the chi-square test at baseline. The Kruskal-Wallis variance analysis and post hoc Bonferroni correction (Mann-Whitney U-test) were used for intergroup comparisons. In the post hoc Bonferroni correction analyses p-values <0.0167 were considered statistically significant while in all other analyses, p-values <0.05 were considered statistically significant.
Results
A total of 97 patients fulfilled the inclusion criteria. Seven were excluded from the study prior to randomization; two were unable to co-operate due to confusion, and five refused to participate. Therefore, 90 patients, who had been diagnosed with CUVW, were included in this randomized controlled study and all completed the study. Patients in the groups with interventions showed good compliance. The attendance rate at the home-based rehabilitation exercises averaged > 90%for all groups. Compliance during the rehabilitation program was excellent as only one patient from Group 1 (WBV) and two from Group 2 (BPT) missed two sessions each. The median age was 51.3 years. There was no statistically significant difference between the groups according to demographic characteristics, as shown in Table 1.
Demographic and clinical characteristics of patients with unilateral vestibular weakness. There were no significant differences between groups at baseline parameters (Kruskal-Wallis variance analysis)
Demographic and clinical characteristics of patients with unilateral vestibular weakness. There were no significant differences between groups at baseline parameters (Kruskal-Wallis variance analysis)
Pre- and post-treatment data for each group are provided in Table 2. Stability score, BBS, and all DHI subscores were significantly different in the WBV group (Group 1) compared to the other groups (Table 2). Post-treatment vertigo VAS scores also differed significantly between the WBV group and the home-based vestibular rehabilitation group (Group 1 versus Group 3) (p < 0.001). On the other hand, the TUG scores were not significantly different (p =0.261). Furthermore, there was no statistically significant difference in vertigo severity, stability score, and DHI total score at the end of the treatment between Groups 2 and 3 (Table 2).
Comparison of the post-treatment clinical characteristics of the groups and intergroup treatment efficacy in patients with unilateral vestibular weakness
pa: Wilcoxon, pb: Kruskall Wallis, pc: Mann-Whitney U test with Bonferroni Correction PreT: Pretreatment, PostT: Posttreatment BBS: Berg Balance Scale, TUG: Timed Up-and-Go, VAS: Visual Analogue Scale DHI: Dizziness Handicap Inventory.
In this prospective randomized controlled study, we compared the efficacy of different types of training in patients with CUVW. BPT or WBV were prescribed to patients in addition to home-based exercises. A third group carried out only traditional home-based vestibular exercises, and served as the control. During BPT, patients attempted to adjust visual inputs by postural movements so that they calibrated postural and visual inputs together. In WBV, the strong vibrations were effective on all of the muscles and joints, especially those responsible for the antigravity reaction. The results of the current study showed that WBV was more effective than BPT at reducing the static posturographic stability score and improving balance in patients with CUVW. This study has also confirmed the results of our previous study which showed that simple home-based exercises alone were also effective for vestibular rehabilitation [40]. We had expected to also see additional benefits with the addition of BPT, and although there were improved values for stability score, BBS, VAS, and DHI, there was no significant difference between BPT+exercises and exercises alone.
Despina et al. worked with elite gymnasts, and using 30 Hz (2 mm) vibrations, found that WBV in-creased flexibility, strength, and improved some balance tests in the acute period [15]. They concluded that the addition of vibration to an exercise program provided superior results compared to the equivalent exercises without vibration. This hypothesis was also tested for improvement in balance of subjects with Parkinson’s disease [16], multiple sclerosis [17], and geriatric age [11]. Uhm et al. worked with acute stroke patients and showed that the addition of WBV to biofeedback training elicited superior results compared to biofeedback alone [41]. They used a similar 30 Hz, 2 mm amplitude protocol. In et al. worked on patients with incomplete cervical spinal cord injury and found that 30 Hz, 2–4 mm WBV stimuli were effective on ankle spasticity, balance, and walking [19]. In a review of the effects of WBV on bone mass in older adults, it was concluded that the addition of WBV to strength exercises may shorten the time to reach desired bone density because of the stimulating effect on osteogenesis [18]. However, bone density is a long-term goal compared with gaining better muscle strength and balance control. All studies in the review had protocols of 6–12 months in order to achieve this goal. The evidence gathered from these studies, including increased muscle strength, bone density and improved balance tests, support our findings.
Multiple sclerosis is often investigated in WBV studies, but the results are contradictory. Schuhfried et al. found significantly improved results in multiple sclerosis patients with low frequency WBV (2.0–4.4 Hz oscillations at 3-mm amplitude) compared to the control group [38]. Mason et al. carried out an 8-week protocol with increasing vibration frequency, up to 26 Hz, and found positive effects on balance and walking time [27]. On the contrary, Freitas et al. could not find any acute or chronic positive effect of 30 Hz WBV in multiple sclerosis patients [17]. The fluctuating nature of multiple sclerosis may lead to these conflicting results. Wegener et al. reported similar ineffectiveness on balance control in patients with back pain [43], using 20 Hz as the highest intensity. In a recent meta-analysis, it was concluded that there is some evidence regarding the effectiveness of WBV on selected balance measures in the elderly, but that it would be too early to reach a conclusion as there are many different protocols and missing parameters make comparisons unreliable [29]. We achieved a clear result for the benefit of WBV on balance parameters, but the mean age of our patients was ∼50, therefore, this was a more active patient group than the elderly population.
An important concern regarding WBV is acute effects on the balance of patients as it is a tiring exercise. However, the studies revealed no negative effect on the balance of different age groups [13, 25], and compliance of our patients to WBV was good. One of the major widespread health problems of today is inactivity. It worsens all health conditions, including vestibular diseases. Inactive individuals have a weaker musculoskeletal system and reduced proprioceptive input due to their sedentary lifestyle. Active participation of these patients in postural exercises is, therefore, difficult. WBV might be a solution for this problem, also
The underlying mechanism of WBV is not only mechanical. Sa-Caputa et al. reviewed the literature and systematically summarized the effects of WBV as stimulation of the hormonal and non-hormonal pathways [35]. They highlighted fluctuations in testosterone, growth hormone, insulin-like growth factor1, epinephrine, norepinephrine, cortisol, and many others. They also found studies that showed alterations in glucose, free fatty acids, adiponectin, etc.[35]. Bosco et al. worked with healthy males and investigated mechanical forces and blood samples before and after WBV therapy. Using EMG measurements, they found an increase in mechanical power output and an improvement in neuromuscular efficiency. They also reported increased testosterone and growth hormone levels and decreased blood cortisol levels in the acute period [12]. We did not focus on these parameters in our study, but all of these hormonal pathways have possible effects on balance control and compensation.
Vibrations could stimulate the otolithic system, and a change in the vestibulo-ocular reflex resulting from low frequency stimulation (up to 1Hz)has previously been reported [37]. In general, the caloric test (a low frequency stimulus) can provide information on a limited frequency range band and a limited part of the peripheral vestibular system (superior vestibular nerve). We could not claim complete denervation of the vestibular system with the caloric test only. Therefore, we can speculate that the possible effects of vibration on the otolith organs and semicircular canals increase the inputs from both ears and participates in the compensation mechanisms in the CNS. There was also a case report where WBV induced benign positional paroxysmal vertigo (BPPV) [6] but we did not observe this.
Whatever the mechanisms, the results were found to increase muscle strength, gait flexibility, and bone mineral density, resulting in a better quality of life with less pain and decreased fall risk, better balance control, and cognitive function [30, 32]. Prisby et al., however, highlighted the lack of standardized protocols [30].
Biofeedback is a common modality in rehabilitation, and the literature includes several studies using methods such as vibrotactile, auditory or visual stimuli [3, 34]. Alkan et al. studied the effect of biofeedback training+exercises on the balance of a group of osteoporotic females and reported that the addition of biofeedback improved the stability score, compared to the control group (exercise only) [3]. We could not find any differences between the same groups in CUWV. Kingma et al. applied vibrotactile feedback stimulus via a belt to patients with bilateral vestibular weakness and found that the belt was an effective prosthesis for improving their quality of life [22]. Bao et al. confirmed these results and concluded that vibrotactile biofeedback may provide additional benefit, lasting up to 6 months [10]. Rosiak et al. compared the visual biofeedback with a virtual reality system and found that there were no differences between groups in posturographic parameters but that virtual reality improved subjective parameters [34]. This subjective difference may be due to the fun effect of virtual reality. Lupo et al. emphasized that patients with stroke not only benefit from biofeedback training but their compliance was also better than that of the control group [25]. Chang et al. used the same biofeedback system and stability score as in our study, and found that biofeedback showed better results in parkinsonism than conventional balance training [14]. We found improved values for stability score, BBS, VAS, and DHI, although we did not find a significant difference between BPT+exercises and exercises alone.
Lacour et al. suggested that vestibular rehabilitation programs that start early, with the active par-ticipation of the patient, targeting different aspects of sensory systems, will improve the results [24]. Using only one type of stimulus cannot fulfill the goals of vestibular rehabilitation, but by adding different proprioceptive and visual inputs to the program, we can improve results. Jáuregui-Renaud et al. reported that patients with peripheral vestibular disease had improved postural control when proprioceptive exercises were carried out in addition to Cawthorne and Cooksey exercises [21]. There are several alternatives for visual, vestibular, and proprioceptive inputs and the type of exercise, duration, and outcome measures must be planned using a team approach. Tailored programs according to age, physical and cognitive condition, and pathology of the patients will be more beneficial [45].
We hypothesized that WBV would increase the proprioceptive impulses to the CNS and provide a trusted stimulus to maintain balance control. The vibrations would also have a positive effect on the strength of the muscles and ligaments and both mechanisms would be beneficial in maintaining balance control. The results of the study proved our hypothesis.
A potential limitation of the present study was the evaluation of assessment parameters only at the end of the study and not carrying out a follow-up evaluation. A second limitation was the predomina-nce of females, who are more likely to seek help and volunteer for studies. We could not find any study comparing WBV between male and female subjects. For future research, it is worth investigating the idea that WBV could be more effective in males due to their higher muscles/fat ratio. Another limitation of the study, which we did not consider, was the previous physical condition of the patients as a differential factor, e.g. body mass index, muscle strength. These parameters were also related to gender. Also, we cou-ld not omit the effect of WBV on the vestibular system via semicircular canals and otolith organs as vestibular sensory organs are also sensitive to this kind of stimulus. Vibration threshold of the proprioceptive system may have an impact on WBV technique and a further limitation was that we did not know the intersubject difference in vibration thresholds.
Further longitudinal, prospective studies are warranted to evaluate the long-term results of the WBV in patients with unilateral vestibular weakness. Also, it would be worth considering parameters such as sex, body mass index, muscle strength, and vibration threshold to evaluate individual differences. It is important to establish standardized WBV parameters for different age and sex groups, but creating homogenous patient groups in this subject is difficult, therefore, the collaboration of multiple clinics is needed.
In conclusion, all three experimental groups showed improvement in postural tests and subjective questionnaires. Adding WBV to home-based exercises resulted in improved rehabilitation outcomes compared with the exercises alone. This study also demonstrated that WBV was a more effective vestibular rehabilitation add-on for improving balance than BPT.
Footnotes
Acknowledgments
*All authors (Fazıl Necdet Ardıç, Hakan Alkan, Funda Tümkaya, Füsun Ardıç) work together for designing the study, acquisition, and analysis of data, and writing the manuscript. We thank to Statistician Hande Şenol, Ph.D. for statistics.
*This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
*The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.