
Abstract
BACKGROUND:
Cochlear implantation may be complicated by concurrent injury to the vestibular apparatus, potentially resulting in disabling vertigo and balance problems. Information on vestibular function before implantation as measured by the video head impulse test (VHIT) and cervical vestibular evoked myogenic potentials (cVEMPs) is scarce and literature on long-term effects is non-existing.
OBJECTIVE:
We aimed to evaluate how vestibular function was affected by cochlear implantation (CI), as measured by VHIT and cVEMPs in the late phase after implantation.
METHODS:
Retrospective repeated measurement study. Patients: Among the 436 patients elected for CI surgery during 2013 to 2018, 45 patients met the inclusion criteria (CI recipients with a vestibular assessment prior to the first CI and a repeated vestibular assessment after the CI operation). Intervention: VHIT and cVEMPs before and after cochlear implantation. Main outcome measures were vestibular function as evaluated by VHIT gain, saccades and cVEMPs.
RESULTS:
The mean time between first and second vestibular screening was 19 months. The mean VHIT gain on implanted ears was 0.79 before the operation and showed no change at follow-up (p = 0.65). Likewise, the number of abnormal VHIT gain values was equal before and after the operation (p = 0.31). Preoperatively, saccades were present on 12 ears (14%) compared with 25 ears (29%) postoperatively (p = 0.013) and were associated with significantly lower VHIT gain values. Preoperatively, positive cVEMPs were found in 20 CI ears (49%) and 24 contralateral ears (62%). 10 CI ears lost cVEMP postoperatively compared with 2 ears on the contralateral side (p = 0.0047).
CONCLUSIONS:
Even though VHIT gain has been reported to be affected in the immediate post-implantation period, the findings in this study show that VHIT gain is normalized in the long-term. However, cochlear implantation is associated with the occurrence of VHIT saccades in the long-term and these are associated with lower VHIT gain values. In addition, cVEMP responses are significantly reduced long-term on implanted ears, which agrees with other studies with shorter follow-up.
Introduction
Vertigo is the most common post-operative complaint following cochlear implantation (CI), affecting approximately 25% (10). The vertigo can evidently be explained by iatrogenic affection of the vestibular apparatus, as histopathologic vestibular changes after cochlear implantation are not uncommon (20). Causes for vestibular changes may include e.g. traumatic, inflammatory, hemorrhagic and vascular compromise triggered by opening of the cochlea and electrode insertion. Increasing focus on vestibular affection has led to vestibular assessment as a standard part of the workup prior to implantation, in order to screen for vestibulopathy preoperative (2, 17, 21). The assessment can assist decision-making in the selection of the ear most suited for implantation.
In addition, due to the frequency of vertigo after surgery, objective assessment of the vestibular status post-operative has become of interest in many CI centers. In a recent meta-analysis, Hänsel et al (11) systematically reviewed subjective vertigo complaints and vestibular dysfunction after cochlear implantation, although not considering the widely used video head impulse test (VHIT) (8). VHIT testing has indeed been performed in the immediate post-operative period, e.g. two days post-CI (4, 12, 13). However, although long-term affection is expected since histopathologic changes can be found in temporal bones with CI, the existing literature does not answer the question if the early VHIT findings can be found in a later stage.
We aimed to examine vestibular function long-term after CI, by the assessment of VHIT gain, saccades and cVEMPs.
Methods
Study design and setting
We performed a retrospective comparative study of all cochlear implantations performed at our tertiary referral center between 2013 and 2018. During this period, 436 CI recipients were identified. The recipients represented 360 cochlear implantations of which 69 was bilateral (single procedure), in addition to 114 contralateral (“sequential bilateral”). Furthermore, 18 re-implantations were performed (e.g. due to device issues). In total, 561 cochlear implantations were performed in the period. In our institution, if indicated, contralateral procedure is offered according to the national public standard of care. Vestibular screening both before first CI and before any sequential contralateral CI is mandatory in the work-up for all CI candidates who can cooperate to undergo vestibular testing. The standard surgical CI procedure applied in our institution is the round window approach.
Patients
Inclusion criteria consisted of 1) CI recipients, with 2) a vestibular assessment prior to the first CI and 3) a repeated vestibular assessment after the CI operation. Thus, we included consecutive patients who received sequential bilateral cochlear implantation. As a result, two sequential vestibular tests were performed; one before the first CI (“preoperative”) and one before the second CI (“postoperative”), allowing assessment of the impact of the first CI on vestibular function (Fig. 1). One patient received primary bilateral implantation but had a postoperative vestibular assessment performed. The study was authorized by approvals from the Data Protection Agency (record number 2012– 58– 0004) and the Patient Safety Authority (record number 3– 3013– 2344/1).
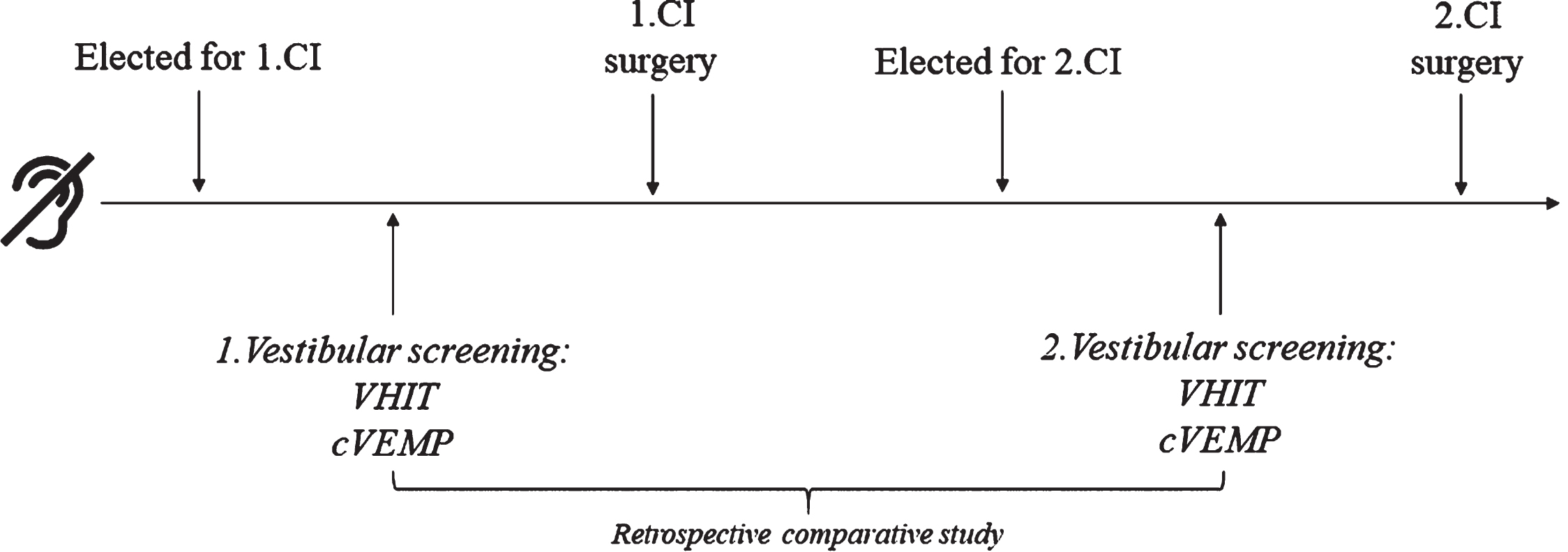
Timeline for included patients. Timeline for the included patients (n = 45). Patients underwent vestibular testing with VHIT and cVEMP tests as a part of both first and second pre-CI work-up. The mean interval between the two vestibular evaluations was 19 months and the mean interval between 1.CI surgery and second vestibular evaluation was 14 months. CI = cochlear implantation; cVEMP = cervical vestibular evoked myogenic potential; VHIT = Video head impulse test.
Vestibular screening before cochlear implantation included the video head impulse test (VHIT) in the horizontal plane and the cervical vestibular evoked myogenic potential (cVEMP) test, which respectively evaluate the vestibulo-ocular (VOR) and the vestibulo-collic reflex. The vestibular tests were with very few exceptions performed by the same examiner. The VHIT (EyeSeeCam, Interacoustics, Middelfart, Denmark or ICS impulse, Otometrics, Taastrup, Denmark) is performed with the patient fitted with videonystagmography googles, fixating on a wall spot at a distance of approximately 1 meter as the examiner applies horizontal head thrusts in a random pattern. The outcome measures of VHIT used were VOR gain (defined to be abnormal when gain <0.7, as previously suggested by Halmagyi et al. (8)) and catch-up saccades (abnormal in presence of consistent covert or overt saccades) (15). Head impulses were rejected if below 150 degrees/second (EyeSeeCam) or 120 degrees/second (ICS Impulse). The cVEMP test (Eclipse, Interacoustics, Middelfart, Denmark) is performed at each side individually by stimulating the saccule through air-conducted loud tone bursts (standard 100 dBnHL at 500 Hz) with an electrode detecting the elicited myogenic activity in the ipsilateral contracted sternocleidomastoid muscle (19). The cVEMP outcome was defined to be abnormal when absent.
Statistics
The GraphPad Prism software (7) version 8.0 (GraphPad Software, La Jolla California USA) for Windows was used for data handling and graphic illustrations. The Mann-Whitney (U) and the Wilcoxon paired tests (W) were used for nonparametric continuous data, and Chi square (χ2) test was used for nominal data. Significance level was defined to be a two-tailed p-value < 0.05.
Results
Baseline information
Forty-five patients with two available vestibular assessments were included. There were 26 females (58%) and 19 males (42%). Mean age was 51 years [range 8– 79] at first implantation. Three recipients were children. All patients had bilateral profound hearing loss. Etiologies of hearing loss were uncertain DLA (acoustic labyrinth degeneration) (n = 10), non-congenital inherited DLA (n = 10), congenital non-specified DLA (n = 8), Pendred syndrome (n = 4), meningitis (n = 3), auditory neuropathy (n = 2), congenital inherited DLA (n = 2), connexin 26 defect (n = 2), otosclerosis (n = 1), posttraumatic (n = 1), sudden deafness (n = 1), and branchio-oto-renal syndrome (n = 1). Otoscopy findings were normal (n = 38), with tympanosclerosis (n = 2), retracted ear drum (n = 2), tympanosclerosis and retraction (n = 1), ear drum transplant (n = 1), ear drum perforation (n = 1).
The mean time from first to second vestibular screening (pre-1.CI and post-1.CI) was 19 months (range 8– 47; SD 10 months). The mean time from first cochlear implantation to second vestibular screening was 14 months (range 2– 42; SD 10 months).
VHIT gain and saccades
Mean gain values (both ears) were 0.82 (range 0.17– 1.35; SD 0.21) before first CI and 0.81 (range 0.12– 1.33; SD 0.22) after first CI (p = 0.503; W). Post-implantation, the mean gain on operated ears was 0.79 compared with 0.82 on contralateral ears (p = 0.69; W).
Considering the operated side, mean gain values on implanted ears were 0.79 (range 0.38– 1.35; SD 0.22) before first CI and 0.79 (range 0.28– 1.21; SD 0.22) after first CI (p = 0.65; W) (Fig. 2). On implanted ears, 13 patients had abnormal gain (<0.70) before the operation and 10 patients had abnormal gain after the operation (p = 0.31; χ2).

VHIT gain before and after first CI. There was no significant difference between mean preoperative gain (0.79) and mean postoperative gain (0.79) on implanted ears. SD (whiskers) is also unchanged. Re-testing was performed at a mean of 14 months postoperative. SD = standard deviation; VHIT = video head impulse test.

cVEMPs before and after first CI. On implanted ears, significantly more patients (53%) lost their cVEMP as compared to the contralateral, non-implanted ears (9%) (p = 0.0047; FE). CI = Cochlear implant; FE = Fisher’s exact test; cVEMP = Cervical vestibular evoked myogenic potential.
Regarding all ears, before the first operation 12 ears (14%) demonstrated saccades. After the operation this number had increased to 25 ears (29%) (p = 0.013; χ2). Comparing sides after the first implantation, there were 17 CI-ears with saccades and 26 ears without saccades. On the contralateral side, 8 ears demonstrated saccades and 35 ears had no saccades. The difference between CI ears and contralateral, non-implanted ears was significant (p = 0.03; χ2). However, when considering ears with new incidents of saccades post-operative, relative to preoperative, there were 10 CI ears with new saccades and 6 contralateral ears with new saccades, respectively. This difference was non-significant (p = 0.27; χ2).
Postoperatively, the mean gain value for ears with saccades was 0.62 and 0.88 for ears without saccades (p < 0.001; U). When considering only new incidents of saccades, ears with post-implantation saccades had a mean gain value of 0.63 versus all other ears with a mean gain of 0.85 (p = 0.0014; U).
Preoperatively, CI ears had positive cVEMPs in 20 cases (49%) and absent cVEMPs in 21 cases (51%). On contralateral ears, 24 cases (62%) had positive cVEMPs and 15 (38%) had absent cVEMPs. CVEMP data was unavailable for 5 patients (11%) preoperative and 6 patients (13%) postoperative. Postoperatively, CI ears had positive cVEMPs in 13 cases (33%) and absent cVEMPs in 26 cases (67%), and on the contralateral side 26 ears (67%) had positive cVEMPs and 13 (33%) absent cVEMPs (p = 0.0062; FE). If only cases with preoperative positive cVEMPs were considered, 10 CI ears (53%) lost cVEMP postoperatively and 9 ears (47%) had preserved cVEMP. In contrast, on the contralateral side two ears (9%) lost cVEMP postoperatively, and 20 ears (91%) had preserved cVEMP (p = 0.0047; FE) (Fig.3).
Discussion
Summary of results and literature perspectivation
The present study investigates vestibular function retrospectively in patients at long-term (>1 month; mean 14 months) after cochlear implantation. We find that VHIT gain (lateral VOR) function, that may be reduced at short-term (3, 12), is not significantly affected long-term after CI surgery. However, an increased number of patients present with saccades after the implantation. In addition, the occurrence of post-implantation saccades is associated with a significantly lower gain value than for ears without saccades. Considering cVEMPs, a significant number of patients lose the ipsilateral potential after implantation.
Comparing the implanted ears with non-implanted ears, there were more ears with saccades on the CI side both before and after the operation. It would be expected that ears elected for CI would have more saccades, since this is one of the indications for choice of CI ear. However, the absolute number of ears with saccades increased significantly after CI. Thus, on both the implanted and the non-implanted side, the number of ears with saccades doubled.
In 2015, Batuecas-Caletrio et al (3) studied 30 CI recipients for short-term postoperative vestibular changes (re-tested 2 days after the operation). The authors found that 30% of patients demonstrated vestibular changes as measured with the VHIT. Noteworthy, the authors defined gain normality with a higher threshold (0.8) than present study and it should be expected that these differences in interpretation of data would account for some differences in results. However, it appears that immediate VHIT affection is not uncommon after CI. Considering the (long-term) results in the present study, it is plausible that a normalization of gain values takes place during the postoperative period, in accordance with the findings in a previous case report (13). Hence, the length of follow-up is essential to the issue. In the future, patients should be studied at multiple time points after the operation to assess individual vestibular reaction and restitution patterns. Using the scleral search-coil technique, another two studies (n = 28 ears and n = 11 ears) from the same institution performed quantitative head impulse testing (qHIT) on patients 4– 8 weeks after CI (17, 18). Only one subject in each study (3.6% and 9%, respectively) demonstrated a noteworthy decrease in qHIT. Neither study accounted for saccades.
In a clinical setting, both a gain reduction and pathological re-fixation saccades would be considered of importance (1). However, re-fixation saccades may demonstrate a more reliable measure of VOR function long-term than VHIT gain, which is subject to normalization by central compensatory mechanisms. In 2004, Buchman et al (5) reported 1-year and 2-year (n = 28 and n = 14, respectively) post-implantation data on VOR function, as measured by the bithermal caloric test. The authors found that 29% of patients had substantial reduction of their VOR. Interestingly, the dizziness handicap did not reflect these objective changes, and an improvement in postural stability was observed (5).
Limitations of the study and future research
The present study constitutes the largest patient cohort investigating VHIT outcomes after CI, and the first to consider the long-term effect. A limitation to the study is the slightly selected patient cohort, as is the nature of the retrospective setup. Although consecutively assessed and included, the patient cohort omits patients that do not meet criteria for a second CI or those not interested in bilateral CI. It is not implausible, that a patient with severe CI-induced vestibulopathy and subjective complaints, would be discouraged to initialize another CI work-up, thus carrying a selection bias to the study. We know from previous studies that some patients are advised against a second CI due to poor unilateral vestibular performance in the previously implanted ear (21). In addition, the vestibular testing setup is incomplete since not all the vestibular end-organs are studied with lateral VHIT and cVEMP. Some studies have shown discrepancy between vestibular tests (3, 12, 16), leaving the possibility for false negative results when only performing two tests. A complete and more accurate vestibular investigation would require more comprehensive vestibular assessment (e.g. include the caloric test and the testing of all semi-circular canals (RALP and LARP) in the VHIT). Future studies should also include evaluation of patient-perceived disequilibrium (e.g. dizziness handicap) to study the subjective impact associated with vestibular dysfunction after CI.
True vestibular loss, artefact or vestibular performance variability
As demonstrated in previous literature, cVEMPs are more vulnerable to CI surgery than other tests. Being anatomically close to the inserted electrode, the saccule is at high risk for trauma, inflammation or vascular change that may compromise function and cause chronic late vestibular complaints (9,20). However, elicitation of a cVEMP is dependent on an intact and freely vibrating ossicular chain and tympanic membrane, and one may speculate that the presence of the CI electrode in the round window (and scala tympani) and scar tissue from the packing potentially involving the adjacent ossicular chain can cause a pseudo-conductive energy loss (shunting) that will hamper energy transduction to the saccule, thus leading to a false negative, absent VEMP. Intuitively, the patients would report more vestibular complaints if the loss of the cVEMP was attributed to a real loss of saccular function, which again advocate for a strong correlation between objective and subjective findings, which has only been partially demonstrated in previous studies (3, 5, 20). Conversely, in case of enlarged vestibular aqueduct, that may be found in Pendred syndrome, cVEMP elicitations may be abnormally hypersensitive (22). Among the 4 individuals with Pendred syndrome in present study, 3 had preimplantation bilateral cVEMP responses, but only one of these was preserved on the implanted ear after surgery. Implications of CI on both subjective and objective vestibular function in individuals with large vestibular aqueduct should be a focus for future research.
Interestingly, some patients performed better at the second vestibular assessment, as compared with the first. It appears that in this population, there is some degree of fluctuation in the vestibular function and/or intra-individual variability. Vestibular testing of individuals with profound SNHL is often more challenging than in the normal hearing population (21). The difference in performance could represent inaccurate recordings (8) or intra- or inter-examiner variability (1). The fact that assessment was made with two types of vestibular devices (Interacoustics and GN) may play a role in this regard. The two VHIT systems have previously been found to demonstrate good inter- and intraexaminer reliability, however to avoid bias in any inaccuracies in calculating VHIT gains between the two systems, future protocolized studies should apply only one system and one examiner (1). Moreover, a potential methodological limitation of the study is the camera position of the VHIT device as the VOR gain may be larger in the adducting eye (20). Data on camera position were not available for the EyeSeeCam device, however the camera on the ICS impulse device is positioned to capture the right eye movements resulting in higher right-sided gains. Camera position should be taken into account in future VOR analyses. In addition, details on cVEMP amplitudes sizes were unavailable. Future studies investigating cVEMP amplitudes may disclose other subtle saccular changes. As information on imbalance and dizziness handicap was not available in present study, the vestibular loss found can currently not be concluded to have functional or subjective impact on quality of life and daily life activities. Noteworthy, previous studies have found weak association between objective and subjective vestibular findings (3, 14). The disagreement may be explained by contralateral normal vestibular function and compensatory mechanisms. Nonetheless, a unilateral vestibular loss may be clinically important if a contralateral vestibular function is jeopardized by comorbidity or later bilateral implantation. Thus, in case that a unilateral vestibular dysfunction is found during a CI workup the ear with normal vestibular function is relatively contraindicated to elect for implantation. Conversely, from a vestibular perspective the ear with preoperative vestibulopathy should be favored for implantation (21).
Conclusion
Even though VHIT gain has been reported to be affected in the immediate post-implantation period, the findings in this study show that VHIT gain is normalized in the long-term. However, cochlear implantation is associated with the occurrence of VHIT saccades in the long-term and these are associated with lower VHIT gain values. In addition, cVEMP responses are significantly reduced long-term on implanted ears, which agrees with other studies with shorter follow-up.
Disclosure And Funding
Nothing to disclose. The contents of this paper have not been published or presented previously.
Footnotes
Acknowledgments
The authors would like to acknowledge vestibular assistant Gerd Hansen for her important work.