
Abstract
BACKGROUND:
Surgical treatment of vestibular schwannoma (VS) leads to acute ipsilateral vestibular loss if there is residual vestibular function before surgery. To overcome the sequelae of acute ipsilateral vestibular loss and to decrease postoperative recovery time, the concept of preemptive vestibular ablation with gentamicin and vestibular prehabilitation before surgery has been developed (“vestibular prehab”).
OBJECTIVE:
Studying postural stability during walking and handicap of dizziness over a 1-year follow-up period in VS patients undergoing vestibular prehab before surgical treatment of VS.
METHODS:
A retrospective review of consecutive patients with a diagnosis of a VS undergoing surgical therapy from June 2012 to March 2018 was performed. All patients were included with documentation of the length of hospital duration and the Dizziness Handicap Inventory (DHI) and the Functional Gait Assessment (FGA) assessed preoperatively as well as 6 weeks and 1 year postoperatively.
RESULTS:
A total 68 VS patients were included, of which 29 patients received preoperative vestibular ablation by intratympanic injection of gentamicin. Mean VS diameter was 20.2 mm (SD 9.4 mm) and mean age at surgery was 49.6 years (SD 11.5 years). Vestibular prehab had no effect on DHI and FGA at any time point studied.
CONCLUSIONS:
We found no effect of vestibular prehab on postural stability during walking and on the handicap of dizziness. These findings add to the body of knowledge consisting of conflicting results of vestibular prehab. Therefore, vestibular prehab should be applied only in selected cases in an experimental setting.
Keywords
Introduction
Schwannomas of the cochleovestibular nerve (“vestibular schwannoma” [VS]) are the most common tumors of the internal auditory canal and the cerebellopontine angle [3, 20]. VS have an incidence of at least 1 per 100,000 and there is evidence that there is an increasing incidence due to advanced imaging techniques and imaging availability [14]. Management of VS includes watchful waiting, radiation therapy, and surgery [6, 32]. Surgical removal of VS is associated with an extremely low rate of recurrence and is a well-established definitive treatment option, if the patient is no longer suited for watchful waiting [23]. Three different approaches are commonly used to assess the tumor: Translabyrinthine, retrosigmoidal, and transtemporal. Vestibular function is usually abolished during surgery since around 90 %of cochleovestibular schwannomas originate from the vestibular nerve [20], which in these cases is transected. Further, vestibular function is abolished in the translabyrinthine approach. Although VS may cause vestibular areflexia itself, there is a majority of patients with a (partially) preserved vestibular function preoperatively, more often but not exclusively in smaller tumors or tumors being located more medially [2, 29]. After surgery, this group of patients suffers from an acute loss of the vestibular function leading to vertigo, dizziness, and impaired postural control. Importantly, postoperative vertigo has been shown to be strongly associated with an increased length of hospital stay and worse postoperative quality of life [21, 30].
To overcome the sequelae of acute vestibular loss by preoperative slow adaption to the vestibular loss, Mangusson et al. have developed the concept of preemptive vestibular ablation with gentamicin and vestibular prehabilitation (physical training) before surgery (“vestibular prehab”) [17]. The procedure should allow the patient to recover from his vestibular loss in the preoperative phase, where active physical training is possible in contrast to the immediate postoperative phase, where mobilization is challenging. This should ultimately decrease postoperative recovery time. This procedure should allow the patient to recover from his vestibular loss preoperatively and to enter the surgery in a fully compensated state. Treatment protocols with improvement of the limits of stability and the correction of sensory input selection problems with rehabilitation are known to reduce disability and handicap [18]. This is hypothesized to eventually decrease postoperative recovery time. Several favorable outcomes after vestibular prehab have been reported, such as absence of dizziness and vertigo as well as a benefit in the postural control system in terms of a better short- (adaptation) and long-term (habituation) recovery [17, 25–27]. However, these positive results have all been reported by the same research group and have been challenged by two recent studies showing that vestibular prehab does neither improve objective outcomes, e.g., the subjective visual vertical or posturographic results, nor subjective outcomes such as quality of life from the view of postural control or the Activities-Specific Balance Confidence Scale [4, 10].
In the light of these conflicting results, we aimed to report our experience with vestibular prehab in VS patients with a focus on postural stability during walking tasks and the self-perceived handicap of dizziness on daily life with a follow-up period of one year.
Methods
Ethical considerations
This retrospective explorative study was approved by the local Ethics Committee (application KEK-ZH-Nr. 2018-00862, Kantonale Ethikkommission, Zurich, Switzerland) in accordance with the Helsinki declaration and its amendments. Written informed general consent was obtained from all the participants.
Patients
A retrospective review of all consecutive patients (n = 142) with a diagnosis of a unilateral VS, who underwent surgical treatment at the Department of Otolaryngology, Head and Neck surgery at the University Hospital Zurich (tertiary referral center) from June 2012 to March 2018 was performed (Fig. 1). Patients received vestibular prehab unless fulfilling any of the following three exclusion criteria: (i) Patients with a remaining ipsilateral hearing function and a hearing preserving surgical approach, (ii) patients who already had no residual function of the ipsilateral vestibular organ, (iii) missing consent to vestibular prehab, or central signs/vertigo (clinically and radiologically). (Fig. 2).
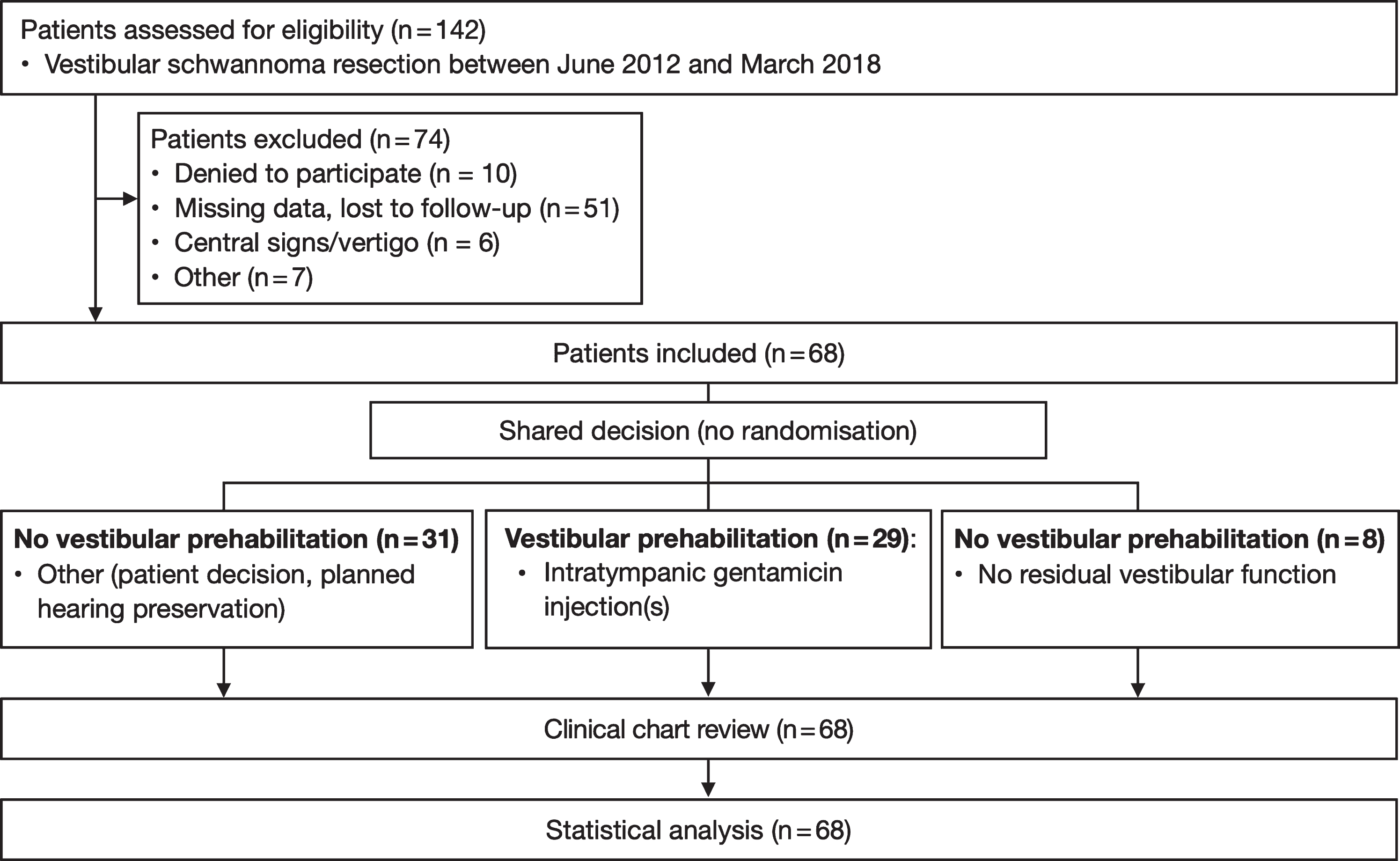
Study flow chart.

(A) Length of hospital stay (day of surgery to day of discharge). (B–C) Dizziness Handicap Inventory scores (B) and Functional Gait Assessment scores (C) over time in vestibular schwannoma patients receiving no vestibular prehab (white), vestibular prehab (dark grey) and patients receiving no vestibular prehab due to no remaining preoperative vestibular function (light gray). P-values refer to treatment effect. Whiskers indicate 10th-90th percentile, bold horizontal line represents median.
The Dizziness Handicap Inventory (DHI) is a 25-item questionnaire assessing the impact of dizziness on everyday life [12]. The DHI minimum score is 0 and the DHI maximum score is 100. A higher DHI total score corresponds to a greater subjective handicap due to dizziness. The minimal clinically important difference (MCID) is estimated at 18 points [12]. The DHI was completed preoperatively within 6 weeks prior to surgery, as well as 6 weeks and 1 year after surgery. If vestibular prehab was performed, DHI was assessed again directly before VS surgery.
Functional gait assessment
The Functional Gait Assessment (FGA) consists of a 10-item score chart and assesses postural stability during walking tasks [33]. The FGA was developed as a modification of the Dynamic Gait Index (DGI) [22, 33]. At our department, the FGA is performed and scored by specially trained physiotherapists. The FGA total score ranges from 0 to 30 as every item is scored on a 4-level (0–3) scale. The MCID is estimated at 4 points [1]. The lower the FGA score is, the greater the clinical gait impairment. The FGA was performed preoperatively within 6 weeks prior to surgery, as well as 6 weeks and 1 year after surgery. If vestibular prehab was performed, FGA was performed directly before VS surgery.
Intratympanic gentamicin injection protocol
Although gentamicin is a preferentially vestibulotoxic aminoglycoside agent, intratympanic injection of gentamicin carries a substantial risk for sensorineural hearing loss [17, 18]. Therefore, vestibular prehab is used with caution, in cases exhibiting (near) normal preoperative hearing where hearing preservation is aimed at. We offered an intratympanic injection of gentamicin to patients with a residual vestibular function as assessed on the side affected by the VS. Before treatment, vestibular function was assessed by video head impulse testing of all semicircular canals. A total of 0.3 ml gentamicin at a concentration of 40 mg/ml was administered as intratympanic injection. Injections were performed in a supine position and via the anterosuperior quadrant of the tympanic membrane under local anesthesia. After completion of the injection, subjects were instructed stay in this position for 30 minutes, during which patients were told not to speak and swallow as little as possible. Vestibular testing using three-dimensional video head impulse test was carried out two weeks after the first injection and at a minimum of six weeks before surgery. If relevant residual function was detected (video head impulse test gain > 0.8 in horizontal semicircular canal and/or gain > 0.7 in any other semicircular canal), additional injections were administered approximately two weeks after the prior injection until vestibular hypofunction including corrective eye-saccades could be detected.
Preoperative physical therapy
Patients, who underwent gentamicin ablation, were instructed about the probable increase of dizziness due to the anticipated loss of vestibular function in the days following the injection. They were enrolled in regular sessions of vestibular physical training in an outpatient setting, carried out by specialized physical therapists. In this group, DHI was completed and FGA was performed again upon entering the hospital for surgery, after completion of vestibular prehab. All patients received postoperative physical therapy after surgery.
Surgical procedures
Depending on tumor size, tumor location and hearing function, an interdisciplinary tumor board made a patient-based decision regarding the surgical approach using a retrosigmoidal, translabyrinthine or transtemporal approach under general anesthesia [6].
Statistical analysis
Null hypotheses and statistical tests were selected before data analysis. The significance level was set to p < 0.05. To determine significant differences between expected and the observed frequencies for binary variables, a chi-squared test was performed if all frequencies were greater than five. Otherwise, Fisher’s exact test was used. Depending on distribution, interval type variables were analyzed using a one-was analysis of variance (ANOVA) for normally distributed data or a Kruskal-Wallis test for data not fulfilling criteria for normal distribution. Differences in DHI and FGA scores among the three groups over time were assessed using two-way repeated measures ANOVA. Statistical analyses were performed using IBM SPSS Statistics, version 24 (IBM Corp., Armonk, NY, USA) and Prism (version 7, GraphPad Software, La Jolla, CA, USA).
Results
Patient characteristics
Out of 142 patients who were assessed for eligibility in the time period of June 2012 to March 2018, 10 patients declined to participate in the study. From the remaining 132 patients, 51 patients were excluded due to loss to follow-up or missing data. A total 6 patients were excluded due to central signs or central vertigo due to brainstem compression (clinically and radiologically). Another 7 patients were excluded due to a complication during the operation or the postoperative rehabilitation: Five patients developed a postoperative cerebrospinal fluid (CSF) leak, of which 3 patients were treated with a lumbar drain and two by revision surgery. One patient developed a hospital-acquired pneumonia and in one patient, the schwannoma was adherent at the abducens nerve, which led to an abducens nerve paralysis. These 7 patients were excluded from this study.
The final analysis included 68 patients (mean age 49.6 years, 41 males, 27 females; Table 1). In this cohort, 29 patients received vestibular prehab. In the remaining 39 patients, reasons for not performing vestibular prehab were no residual vestibular function (n = 8) and planned hearing preservation during surgery or patient decision (n = 31). Regarding the surgical access, patients receiving vestibular prehab tended to be more often operated via a translabyrinthine (17/29, 59%) approach compared to patients receiving no vestibular prehab (5/31, 16%; p = 0.02). Vestibular prehab did not reduce the length of the hospital stay (day of surgery to day of discharge, vestibular prehab: 8.1 [SD 1.7] days; no vestibular prehab: 7.9 [SD 2.1] days; p = 0.16; Fig. 2A).
Demographics and clinical characteristics of vestibular schwannoma patients
Demographics and clinical characteristics of vestibular schwannoma patients
Before surgical intervention and, if applied, before vestibular prehab, median DHI score in the entire cohort was 10 (0–25 [25th–75th percentiles]). In patients undergoing vestibular prehab, no statistically different DHI score before and after vestibular prehab was found preoperatively (2 [0–25] vs. 14 [7–30], p = 0.14). In the entire cohort, there was a statistically significant increase in the perceived dizziness handicap six weeks after surgery to a median DHI score of 23 (5–29, p = 0.03). One year after surgery, the DHI score dropped to 12 (6–27) and the median DHI score was not significantly different from the baseline value (p > 0.99). No significant effect of any type of treatment on DHI scores was observed at any time point, F (2, 109) = 2.74, p = 0.07 (Fig. 2B). No significant differences between patients with and without residual vestibular function within the group receiving no vestibular prehab were observed (data not shown).
Functional gait assessment
Before surgical intervention and, if applied, before vestibular prehab, the median FGA score in the entire cohort was 27 (24–29). In patients undergoing vestibular prehab, no statistically different FGA score before and after vestibular prehab was found preoperatively (27 [23–28] vs. 26 [24–28], p = 0.99). Assessing the entire cohort, FGA scores remained stable at a high level with a median FGA score of 26 (25–27) six weeks after surgery and 27 (25–28) one year after surgery. No significant effect of any type of treatment on FGA scores was observed at any time point, F (2, 163) = 0.51, p = 0.60 (Fig. 2C). No significant differences between patients with and without residual vestibular function within the group receiving no vestibular prehab were observed (data not shown).
Discussion
Here, we report our experience with vestibular prehab in VS patients with a focus on postural stability during walking tasks and the self-perceived handicap of dizziness on daily life. Our VS cohort is the largest cohort undergoing vestibular prehab reported in the literature. In the present study, vestibular prehab before surgical treatment of VS had no effect neither on postural stability during walking tasks nor on the self-perceived handicap of dizziness on daily life compared to standard care without vestibular prehab. Before surgery as well as six weeks and one year after surgery, patients having received vestibular prehab did not significantly differ from patients receiving standard care in DHI and FGA scores. Further, the length of hospital stay (day of surgery to day of discharge) was not decreased by vestibular prehab.
Several studies, all published by the same research group, have reported favorable effects of vestibular prehab before surgical treatment of VS in the past. Firstly, in a sample of twelve patients with preoperatively preserved vestibular function, none suffered of dizziness or vertigo after surgery [17]. Secondly, in a small sample of six patients undergoing surgery for VS by a translabyrinthine access, vestibular prehab led to a significant reduction in postural sway one to six weeks after surgery as well as six months postoperatively [25]. It was concluded that vestibular prehab may lead to better adaption to the unilateral vestibular loss leading not only to a short- but also long-term symptom reduction. Lastly, it was demonstrated that vestibular prehab leads to a benefit in the postural control system in terms of a better short- (adaptation) and long-term (habituation) recovery [27]. It was hypothesized that the improved recovery may be the consequence of a different “sensory weighting”. However, these findings may be expected to be also reflected by in the FGA, which demonstrated no advantage of vestibular prehab on postural stability during walking tasks. This is in line with two recent studies demonstrating no effect of vestibular prehab on several objective and subjective outcome parameters: In a controlled study from 2016, it was shown that vestibular prehab does not significantly improve quality of life [4]. The same study also applied the DHI, the Glasgow Benefit Inventory and the Glasgow Health Status Inventory, all of which showed no differences between patients that had received vestibular prehab and the control group. Furthermore, a study from another group investigating the potential of vestibular prehab to accelerate the vestibular compensation process in the early postoperative course demonstrated no benefit in any of the studied outcome parameters including the subjective visual vertical, posturography and the Activities-Specific Balance Confidence Scale [10]. These latter results are well in line with our findings. In accordance to Čada et al., who studied a time period up to three months postoperatively, we did not find an impact of vestibular prehab on DHI scores reflecting the self-perceived handicap of dizziness on daily life [4]. As a side note, the overall long-term DHI scores in our cohort tended to be lower than reported in the literature [11, 16].
The question remains why vestibular prehab may fail to effectively decrease postoperative adaptation and habituation to the unilateral vestibular loss. Firstly, the outcomes assessed should be critically reappraised. The reported objective measure showing a positive outcome of vestibular prehab is the postural sway as measured as energy expenditure while standing on a force platform during vibratory stimulation of the calf muscles. Yet, it is unclear whether this objectifiable difference also translates to a relevant acceleration of the recovery period and improvement of an objective functional outcome, such as the FGA. Further, it remains elusive whether this difference is a subjectively perceivable difference, which would be reflected in patient-reported outcome measures such as the DHI. On the other hand, generic outcomes such as the FGA and DHI may not be highly sensitive to small changes and therefore not capture small differences and changes in vestibular function. In particular, although the FGA contains vestibular components and objectifies postural stability during gait tasks to predict falls, it may fail in sensitivity when it comes to a VS population. Secondly, gentamicin targets the lateral canal and the otolith organs as determined by caloric stimulation, video head impulse test, cervical vestibular evoked myogenic potentials and the subjective visual vertical [9, 31]. However, it is well known that even with systemic application, gentamicin may spare entire vestibular organs or single frequency ranges that are not covered by current vestibular testing [5, 24]. Therefore, a partial preoperative vestibular function that is not detected in vestibular testing may still undergo a sudden loss due to surgery, resulting in postoperative dizziness and vertigo. This may have led to the similar length of hospital stay. Lastly, the effects of vestibular prehab may also be masked by an intense vestibular rehabilitation in both groups [8, 10]. We may add that vestibular rehabilitation exercises are thought to be the most important factor in compensating a vestibular loss, regardless of the etiology of the loss [7].
Our study has the limitation that vestibular prehab leads to an inherent selection bias since only patients with remaining vestibular function and no planned hearing preservation are selected. These factors further influence the surgical approach, which is reflected in our cohort by a trend towards a higher number of patients with vestibular prehab that were operated via a translabyrinthine access. Moreover, the DHI and FGA are based on a subjective evaluation (DHI) and on the patient’s cooperation (FGA). Furthermore, the outcomes are postoperatively first assessed 6 weeks after surgery, when vestibular rehabilitation exercises may have compensated for any potential differences in dizziness or postural stability among the groups studied. A typical disadvantage of a retrospective study is the high rate of drop outs due to missing data or consent, which was also the case in this study and may result in a possible bias. It remains unclear whether the vestibular prehab treatment aroused patients’ expectations regarding their postoperative dizziness and mobility. To further study this question, a placebo-controlled randomized study with a higher number of patients would be necessary.
In conclusion, no effect of vestibular prehab neither on postural stability during walking tasks nor on the self-perceived handicap of dizziness on daily life was found in this study. These findings add to the body of knowledge consisting of conflicting results of vestibular prehab. Therefore, no clear recommendation can be made for or against vestibular prehab. We are confident that there is a role for prehabilitation in patients undergoing a VS surgery. However, as for now, vestibular prehab should be applied only in an experimental setting and used with caution, in particular with regard to its efficiency. Further studies may investigate larger patient cohorts in a placebo-controlled and randomized manner in order to identify a possible treatment effect, which may be limited to subgroups of VS patients.
Conflict of interest
The authors have declared that no conflict of interest exists.