
Abstract
BACKGROUND:
Benign paroxysmal positional vertigo (BPPV) has a reported recurrence ranging from 26.8 to 50%. Osteoporosis and Vitamin D deficiency seems to have an impact on recurrence of BPPV.
OBJECTIVE:
to evaluate the impact of osteoporosis and Vitamin D deficiency on recurrence of BPPV.
METHODS:
73 consecutive patients were divided in two groups according to the presence (group 1) or absence (group 0) of a recurrent episode. BMD, femoral and lumbar T-scores and Vitamin D levels were recorded. Statistical analysis was performed to investigate correlations.
RESULTS:
patients in group 1 had statistically significant lower values of both femoral (–1,62±1,06 vs. –0,53±1,51; p = 0,001), lumbar T-score (–2,10±1,19 vs –0, 53±1.51, p = 0.001) and Vitamin D (19.53±15.33). The values of femoral T-score and Vitamin D could be combined in a model able to properly classify 65.8% of the cases (p = 0.002) as isolated or recurrent BPPV, with high accuracy (AUC 0.710 [0.590 –0.830]).
CONCLUSION:
present data show a probable correlation between osteoporosis and Vitamin D with recurrent BPPV.
Introduction
Benign paroxysmal positional vertigo (BPPV) represents a vestibular pathology with great prevalence and incidence, respectively 2.4% and 0.6% per year and up to 20–30% of ENT diagnoses [1]. It is the most common peripheral vestibular syndrome, triggered by head position changes on the three planes of the space and is characterized by a recurrent, sudden and paroxystic, vertiginous crisis, with rapid intensification up to a plateau kept from a few seconds to a few minutes, and a rapid decline until its disappearance. In the scientific literature it goes by the adjective of “benign”, although the nature of symptomatology does not always justify this term since it is often violent, sometimes with heavy vagal symptoms. However, this term is meant to differentiate the typical form of the nystagmus (ny) from atypical variants potentially related to central involvement [2]. BPPV crises are recurrent and generally grouped over a limited period of time (active phase) of about 15 days, with a tendency to relapse after silent intervals of unpredictable duration (inactive phase), with a recurrence rate ranging from 26.8 to 50% [1, 3–5]. The only certain cause found in literature is traumatic and about 50% of BPPV is still classified as idiopathic [6]. In the remaining cases, it has been associated with other pathological events involving the labyrinth, such as viral neurolabyrinthitis, sudden loss of unilateral vestibular function for vascular causes, or otologic surgery, all conditions that may somehow cause either a direct detachment of otoconia from utricle macula, their degeneration, or alter the endolymphatic metabolism. It is now widely accepted that the event underlying BPPV is the detachment of small clusters of otoconial debris from utricle macula or the formation of floating aggregates of higher density material than the endolymph. These agglomerates are subjected to both linear and angular accelerations, generated by gravity and rotation of the head, and move within the vestibule, or burden with their mass on adjacent structures stimulating hair cells [7].
Several studies over the past decade have investigated the potential association between BPPV, osteoporosis, and Vitamin D deficiency, suggesting that an alteration in calcium metabolism could cause the detachment of otoconia. Otoconia are particularly important for the inner ear: they are involved in both the sensitivity to gravity and other linear accelerations and the ionic homeostasis as a reserve of calcium ions. They are conglomerates of thousands of calcium carbonate crystals (unlike bones and teeth that are made of calcium phosphate) of about 2-3 mm in length that lie on the surface of a gelatinous membrane [8].
Osteoporosis is a systemic bone disease that causes a reduction in its density and microarchitecture, making it susceptible to fractures. Osteoporosis can be generalized and involve the entire skeleton or can be localized and affect only some bone segments. Calcium plays a key role in physiological situations such as bone formation, muscle contraction, cellular cell membrane potential stabilization, and blood clotting. The bone is constantly subjected to turnover through bone remodeling. The calcium (Ca) and phosphorus (P) ions in and out of the bone mineral phase are under the control of three main hormones: estrogens, parathormon, and Vitamin D metabolites. Vitamin D plays an important role in the homeostasis of calcium and phosphate, it is essential for bone growth and integrity [9]. Given the anatomical structure of the otoconia, which represents a calcium reservoir at the inner ear level, and given their continuous turnover, it has been hypothesized that variations in systemic calcium homeostasis could affect the structure of otoconia and otoliths through the same mechanisms and mediators involved in the process of osteoporosis.
To evaluate the impact of osteoporosis and Vitamin D deficiency in BPPV and their role in recurrent forms we decided to analyze a consecutive series of patients at our Institution.
Material and methods
The objective of this prospective cohort study was to seek if a correlation exists between osteoporosis (diagnosed with femoral and lumbar T-scores as defined by the WHO), Vitamin D deficiency, and relapsing BPPV. Ethical approval and informed consent were obtained from our Institution and enrolled patients respectively. To test our hypotheses all the consecutive BPPV patients fitting the inclusion and exclusion criteria were recruited from January to June 2016 at the audio-vestibular unit of the otolaryngology department, A.O.U. Sassari (Italy). Associated comorbidities were recorded. Exclusion criteria were a history of cranial trauma, ear surgery, previous vestibular deficiencies, or calcium and/or Vitamin D supplementation at the time of the first evaluation. Inclusion criteria were a clinical diagnosis of BPPV through a bedside examination performed with infrared video-oculoscopy analysis. BPPV of the posterior (PSC) and the lateral semicircular canal (LSC) was diagnosed after observation of the pathognomonic ny elicited respectively by Dix-Hallpike and Pagnini Mc-Clure maneuvers. All patients were treated with Semont or Epley’s rehabilitation maneuver for PSC cases and Baloh’s barbecue maneuver for the LSC cases. All patients were then evaluated after one week. The resolution of the episode was defined as the absence of evoked nystagmus or dizziness at the time of the follow-up. Recurrence was defined as a new episode of BPPV at least 15 days after the complete resolution of the previous one. Patients with recurrent BPPV were included in group 1, patients with isolated BPPV in group 0.
To evaluate bone metabolism status, all patients underwent a densitometric examination with Dual-energy X-ray absorptiometry (DXA), a radiological examination that studies the bone mineral density at the femoral and lumbar levels. Specifically, we evaluated the bone mineral density (BMD) and the T-score, a comparison of a patient’s BMD to that of a healthy 30-year-old. According to WHO criteria, normality is defined as a T-score (femoral and lumbar) between +1 and –1 is normal, osteopenia is between –1 and –2.5 and osteoporosis includes values below –2.5 [10]. Patients underwent a serologic test to assess the following parameters involved in phospho-calcium metabolism: 1.25 (OH) D3 (Vitamin D), calcium, phosphoremia, alkaline phosphatase. Normal Vitamin D values were defined as greater than 30 ng/mL, insufficient levels as between 20 and 29 ng/mL, and deficiency as below 20 ng/mL [11]. Calcium values are normally between 8.8 and 10 mg/dL, those of phosphoremia between 2.3 and 4.7 mg/dL, and those of alkaline phosphatase between 40 and 150 U/L.
Statistical analysis
Statistical analyzes were conducted with SPSS 22 software and JASP. The baseline characteristics of patients were reported as mean±standard deviation (SD) for continuous variables and as a percentage for categorical variables. Continuous variables were compared with Student’s t-test for independent samples and dichotomous variables with Fisher Chi-square test and ANOVA. The univariate binomial logistic regression analysis was performed considering the recurrent BPPV as a dependent variable and the independent variables corresponding to all parameters of the study. Predictors that were significant from univariate analysis were tested in a multivariate binomial logistic regression model. A simple linear regression analysis was performed between the femoral T-score and the lumbar T-score. A multivariate binomial logistic regression analysis was performed on the likelihood of being affected by recurrent BPPV starting from a univariate binomial logistic regression analysis. The K-neighbor neighbors (KNN) algorithm was applied to the parameters found to investigate a possible pool of samples. KNN is a non-parametric technique based on determining distances between an unknown object and each object in the training set. K objects closest to the unknown sample are selected and a majority rule is applied: the unknown is classified in the group in which the majority of k objects belong. The classification method was performed after applying the SELECT algorithm as a function selection technique. A ROC curve was built for the likelihood of belonging to the recurrent BPPV group. For all statistical analyzes, a statistically significant difference was assumed for p < 0.05.
Results
73 consecutive patients with a diagnosis of BPPV were recruited from January to June 2016 at the audio-vestibular unit of the otolaryngology department, A.O.U. Sassari (Italy). Group 1 included 43 patients, group 0 included 30 patients. Patients characteristics, scores, and Vitamin D values for each group are shown in Table 1.
Data comparison between patients with relapsing and isolated BPPV
Data comparison between patients with relapsing and isolated BPPV
Patients with recurrent BPPV (group 1) had statistically significant lower values of both femoral T-score (–1.62±1.06 vs. –0.53±1.51; p = 0.001) and lumbar T-score (–2.10±1.19 vs –0. 53±1.51, p = 0.001). Similarly, dividing the sample into three groups (osteoporosis, osteopenia and patients with normal bone density) and analyzing categorical data, a significantly higher number of patients with osteoporosis was included in the recurrent BPPV group, according to the femoral (26% vs. 3%, p = 0.001) and lumbar T-score (51% vs. 23%, p = 0.001). Patients in group 1 had lower values of Vitamin D (19.53±15.33 vs 25.85±14.10). By analysing categorical data (Normal > 30 ng/mL, insufficient between 20 and 29 ng/mL, and deficiency < 20 ng/mL) a correlation between deficient vitamin D levels and BPPV recurrence (p = 0.029) can be evidenced (Fig. 1). The univariate binomial logistic regression analysis confirmed that the significant predictors of recurrent BPPV were the low femoral T-score (OR 0.513 [0.338 –0.780], p = 0.002), lumbar T-score (OR 0.566 [0.339 –0.801], p = 0.001), and Vitamin D deficiency (OR 1.840 [1.072 –3.160], p = 0.027). Linear regression showed a statistically significant linear association (r = 830, R2 = 689; p = 0.001) between lumbar and femoral T-score. Given their shared high significance at the univariate binomial logistic regression analysis, femoral T-score rather than lumbar T-score, along with vitamin D, was chosen arbitrarily as an independent predictor for inclusion in the multivariate binomial logistic regression. The multivariate binomial logistic regression model confirmed that the low T-score femoral values were associated with recurrent BPPV (OR 0.535 [0.349 –0.882], p = 0.004). The subsequent discriminant analysis showed that the values of femoral T-score and Vitamin D could be combined in a statistically significant model (p = 0.002) able to properly classify 66% of the cases as isolated or recurrent BPPV. As expected the femoral T-score and Vitamin D also are linearly correlated (p = 0.0183). As shown by the graphical representation of the model, high Vitamin D values, and femoral T-scores were associated with isolated BPPV and low values to BPPV recurrences (Fig. 2). Starting from the probabilities calculated with the discriminant analysis to belong to group 1 rather than group 0, a ROC curve was built on the likelihood of belonging to each BPPV group, and good accuracy values were obtained for the model (AUC 0.710 [0.590 –0.830]) (Fig. 3).
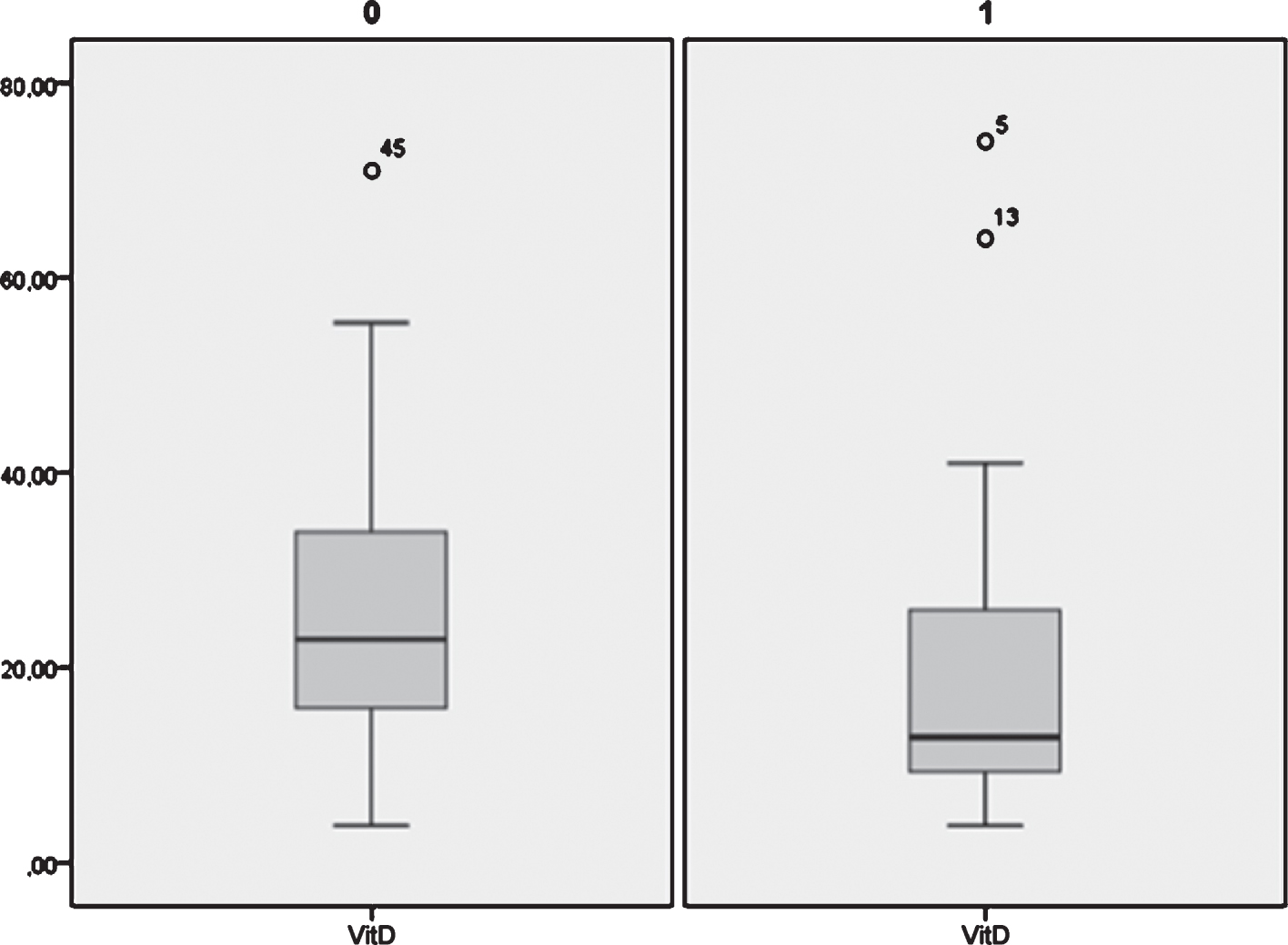
Vitamin D values were lower in group 1 (right side) (19.53±15.33) rather than in group 0 (left side) (25.85±14.10). By analysing categorical data (Normal > 30 ng/mL, insufficient between 20 and 29 ng/mL, and deficiency < 20 ng/mL) emerged a correlation between deficient vitamin D levels and BPPV recurrence (p = 0.029).
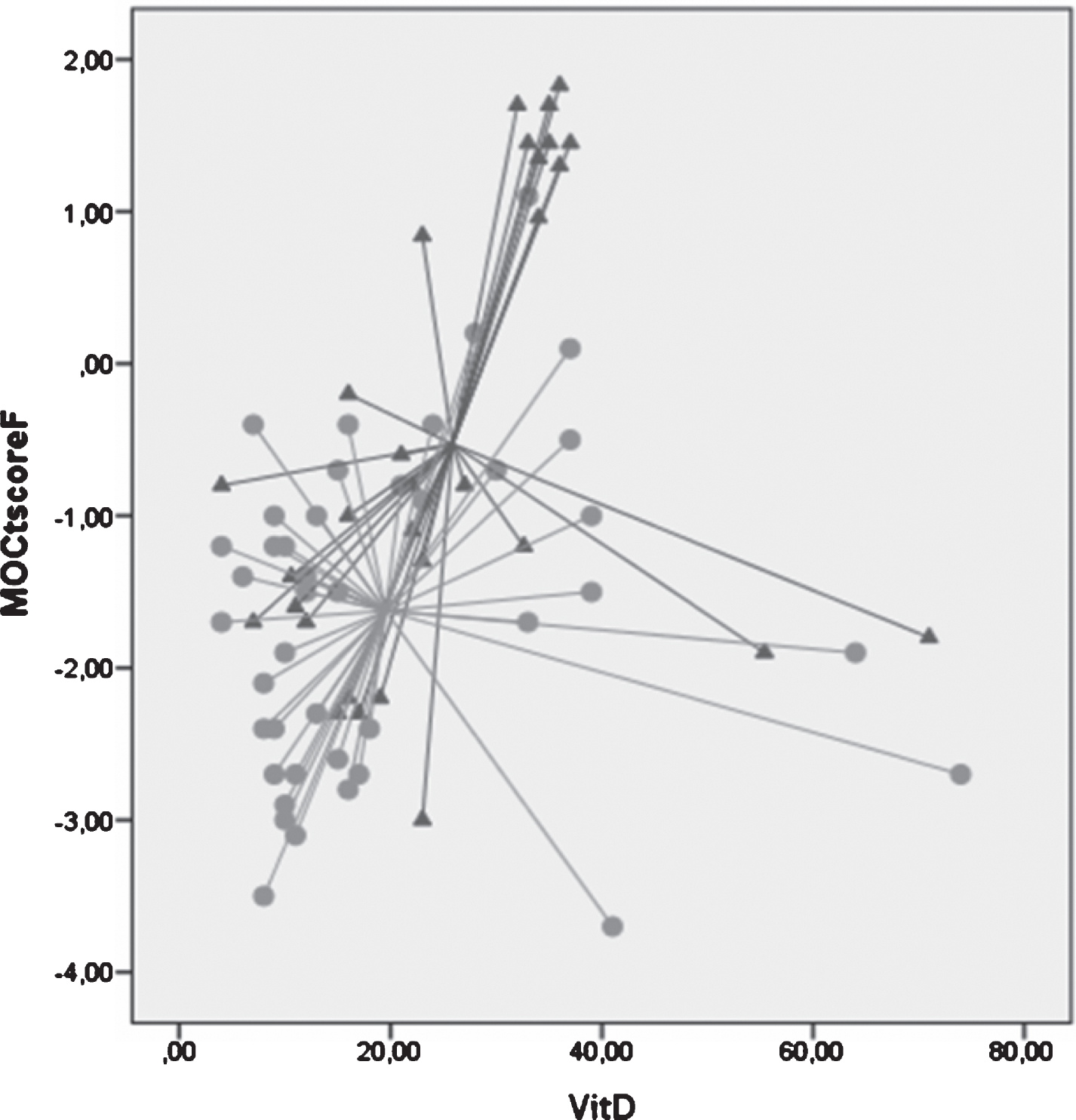
The discriminant analysis showed that the values of femoral T-score and Vitamin D could be combined in a statistically significant model (p = 0.002) able to properly classify 66% of the cases as belonging to the relapsing (circles) or isolated (triangles) BPPV group.
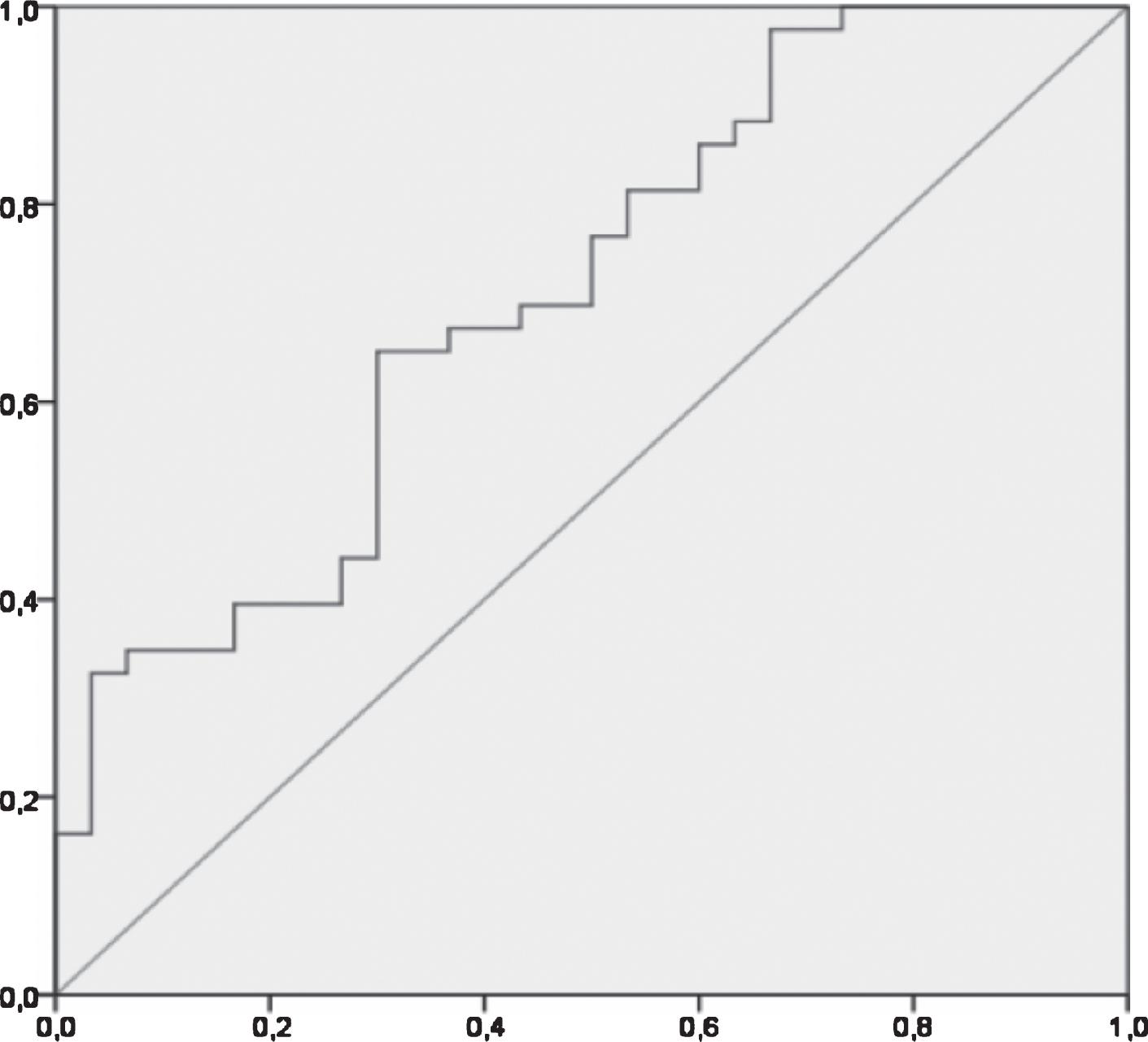
Starting from the probabilities calculated with the discriminant analysis to belong to group 1 rather than group 0, a ROC curve was built on the likelihood of belonging to each BPPV group, and good accuracy values were obtained for the model (AUC 0.710 [0.590 –0.830]). (X axis = specificity; Y axis = sensitivity).
Benign paroxysmal positional vertigo is known to be the most frequent otoneurological disease, accounting for up to 20–30% of ENT diagnoses [1]. It may occur at any age, but is considered exceptional in adolescents, being more frequent in the adult and in the elderly [9]. The 73 patients of the present series displayed a a mean age (63.81±12.49), consistent with the literature [6]. In our analysis age, sex, Ca2+, phosphoremia, semicircular canal (posterior vs. lateral), and involved side did not show significant correlation with recurrence. However, the PSC was the most commonly involved canal in both groups (respectively in 79% of group 1 and 66% in group 0) and the right side was the most involved. Also these data are consistent with the literature [6] as other Authors found that the most common form of BPPV involves the posterior semicircular canal (PSC) with a prevalence of the right side [12], while the lateral semicircular canal (LSC) is involved in a percentage of only 5 to 22%. In most of the recurrent patients in our series (n = 30), the same side of the first presentation was affected. This suggests the presence of an “organ damage” involving a particular semicircular canal, as suggested by Oas [13].
Otoliths are made up of Calcium Carbonate and are produced through a biomineralization process [8, 13]. A negative feedback mechanism modulates formation, slowing it down when the otoliths have reached their proper mass and shape. Recently, hypothesizing that such calcium recycling process may be altered by age or concomitant systemic pathological processes such as osteoporosis, attention has been paid to the possible role of calcium dysmetabolism in the increased tendency of otoconia to detach from the macula. Such connection, and also the possible association with Vitamin D deficiency has been further suggested by the known and synchronous seasonality of both BPPV and Vitamin D levels, as highlighted by some papers [14–17].
By conducting a research on scientific databases with specific keywords (osteoporosis, BPPV, Vitamin D, calcium metabolism), we were able to find, starting from 2009, 20 studies that have tried to establish an association between osteoporosis, markers of calcium metabolism, and primary and recurrent BPPV. Many of them, focusing on BMD, T-scores and/or Vitamin D have succeeded in establishing an association [18–33]. Among the first to suggest an association between BPPV and osteopenia/osteoporosis were Vibert and colleagues, that found 75% of the enrolled women having such condition and a lower T-score irrespective of the age category [29]. A few years later an interesting paper from Jang and Kang confirmed this observation on higher numbers of patients and expanded the concept by finding that a lower BMD was associated with a higher number of canalith repositioning maneuvers [31]. In 2009 Jeong and colleagues published the first paper demonstrating an association between lower BMD and BPPV in both men and women [33]. An association with a higher number of recurrences was instead proposed by Yamanaka et al. [18]. On the other side of the coin, in 2010 Mikulec and colleagues found a potential protective effect of treated osteoporosis on BPPV [30]. Jeong and colleagues in 2013 published a study that builds on the previous evidence of an association between BPPV and osteoporosis showing an association between lower levels of vitamin D and BPPV [32], a finding further confirmed by Talaat and colleagues [19]. Some following works questioned these results, with different arguments, such as that being both osteoporosis and BPPV rather frequent disorders, a casual rather than causal association was more probable [34], that the prevalence of BPPV in patients affected by osteoporosis is low [35], and that even if the correlation between T-score and a marker of BPPV (Otolin-1) is strong, such correlation is not seen between Otolin-1 and markers of osteoporosis such as P1NP or NTX [36]. Analyzing the literature on the subject as a whole, it is clear anyway that there is inhomogeneity in study designs, sample sizes, objectives, population studied as a reference (i.e. populations of BPPV patients or patients affected by osteoporosis). Moreover, most of the studies carried out to date did not examine all of the calcium metabolism parameters analyzed in our study at the same time, and many only focused on a particular subset of patients such as postmenopausal women, men or women in general [18, 37]. At any rate, a recent literature review and meta-analysis of the literature by Yang and colleagues has recently concluded that the available evidence suggests that BPPV is associated with decreased levels of serum Vitamin D, and Vitamin D deficiency is an independent risk factor for BPPV [38].
Only a small subset of the available studies compared the differences in the prevalence of osteoporosis (as defined by BMD and T-score values) in patients affected by isolated and recurrent BPPV, mainly concluding that lower values of BMD and higher T-scores are associated with recurrence, a result which is further supported by our results that highlighted an association between lower T-score values and an increased likelihood of BPPV recurrence [18–20, 31]. Such association is interesting also because the significant difference between isolated and recurrent cases is another hint at a causal association between calcium metabolism and BPPV. Still, some controversy exists as at least one paper from Kim and colleagues found that occurrence but no recurrence of BPPV was associated with BMD [20]. It should be noted that among our study and others the definition of recurrence has not always been the same, thus bringing another layer of possible bias while comparing data.
Almost all studies have analyzed only BMD and T-score values without taking Vitamin D values into consideration, in particular there is little literature on the comparison of values between patients with isolated and recurrent BPPV. We know that Vitamin D serum levels undergo significant seasonal fluctuations since 1,25-dihydroxyvitamin D is a photochemical mediator produced by a precursor, namely 7-dehydrocholesterol [39]. Our patients were sampled between the winter period and the beginning of the spring season, so the values of Vitamin D reported are fairly homogeneous, and differences between isolated and recurrent BPPV can be evaluated without much bias due to seasonal fluctuations. Few studies have shown that Vitamin D concentrations are significantly reduced in patients with recurrent BPPV compared to those in the first episode [19, 40–44]. In our study patients with vitamin D deficiency have a higher probability of having recurrent rather than isolated BPPV. Taking into consideration the whole population in our study, a condition of Vitamin D deficiency rather than an insufficiency was present. Nonetheless, a recent work by Maslovara and colleagues showed that the serum level of Vitamin D is not significantly different in patients with recurrent and non-recurrent BPPV [40], and a paper from Yang and colleagues did not find a correlation at a multivariate analysis between low Vitamin D levels and recurrence [24]. However, again, a recent review and meta-analysis by Yang B found that Vitamin D levels are not only significantly lower in BPPV patients but specifically lower in recurrent than non-recurrent BPPV [38], a evidence further confirmed by AlGarni and colleagues [45]. Such evidence has led some to attempt Vitamin D supplementation in order to reduce the recurrence of BPPV. Two studies in 2016, on 81 and 93 patients respectively [46, 47], showed that supplementation of Vitamin D in patients with recurrent BPPV significantly reduced the recurrence rate [46, 47].
Another interesting, even if expected, finding is the linear correlation between T-score and Vitamin D values and that together are sufficient to properly classify patients as belonging to the recurrent or isolated BPPV group in almost 66% of cases, a notion further confirmed by the ROC curves that highlight a good accuracy. This criteria, if proven valid in a prospective study, could be used to counsel the patient, and to discriminate between patients more prone to recurrence, thus more fit to be treated with Vitamin D supplementation. At the same time this data suggest that BPPV is correlated to calcium metabolism as a whole, and not to a single parameter, and thus studying many different parameters, even intercorrelated, as we did in the present study, may help giving a more comprehensive view on the issue
The epidemiological approach to the patients with relapsing paroxysmal positional vertigo remains quite complex, but it is of paramount importance to keep searching for a causal therapy, in order to interrupt the onset and recurrence of BPPV. Our study, among others, shows a correlation between relapsing BPPV and calcium metabolism alterations, suggesting that the calcium homeostasis in the inner ear can be altered by systemic mechanisms similar to those involved in other clinical conditions, such as osteoporosis. Further studies are therefore desirable both to define precisely the relationships between calcium metabolism and BPPV and to evaluate the efficacy of potential therapies targeting these pathways (as vitamin D or estrogen supplementation [48]) in preventing BPPV recurrence. Vitamin D supplementation in particular seems to be promising with a recent randomized trial and a recent meta-analysis both proving a protective effect of vitamin D supplementation on the recurrence rate on BPPV [49, 50].
Conflict of interest
The authors declare that they have no conflict of interest.