
Abstract
BACKGROUND:
Several studies on seasonal variation in benign paroxysmal positional vertigo (BPPV) have been reported. However, the association between season and BPPV remains controversial; thus, further study is required.
OBJECTIVE:
We analyzed patients with BPPV to evaluate monthly and seasonal variations.
METHODS:
Patients with BPPV seen between 2013 and 2017 were retrospectively enrolled in this study. Differences among the months and seasons of BPPV visits were analyzed. Patients were divided into two groups according to age (65 years or older and younger than 65 years) and sex, respectively, and the differences were analyzed in each group.
RESULTS:
There was no significant difference in the monthly or seasonal distribution of BPPV in the 1,216 patients. There was also no significant difference in the monthly or seasonal distribution in the older and younger groups or in male and female patients.
CONCLUSIONS:
There was no significant difference in the monthly or seasonal distribution of patients with BPPV. Additional studies on seasonal variation in BPPV are required in terms of not only vitamin D levels but also other associated factors.
Introduction
Benign paroxysmal positional vertigo (BPPV) is the most common type of vertigo [4, 24]. The reported incidence of BPPV was 0.6% per year and the lifetime prevalence of BPPV was 2.4% in a population-based study in Germany [4, 23]. BPPV is characterized by recurrent vertigo induced by positional changes of the head [2, 23]. In BPPV, detached otoconial debris from the utricular macula, which is composed of protein and calcium carbonate, moves around in the semicircular canal or attaches to the ampullary cupula [2, 24].
BPPV may be secondary to head trauma, Ménière’s disease, or vestibular neuritis (VN). However, most commonly BPPV is idiopathic [5, 23]. Recently, vitamin D has been reported to be associated with BPPV [3, 21]. Vitamin D regulates calcium metabolism not only in bone, but also in the otoconia of the inner ear [7, 24]. Serum vitamin D levels have been reported to vary seasonally due to variations in seasonal insolation or skin exposure to sunlight [18, 22].
Considering the association between vitamin D and BPPV, it is important to evaluate seasonal variations in BPPV, and there have been several studies [12, 24]. Most found that specific seasons or periods were associated with BPPV, while one reported no correlation between seasons and BPPV.
The possible association between seasons and BPPV remains unclear; thus, further studies are required. Here, we analyzed a large number of patients with BPPV seen over several years to evaluate monthly and seasonal variations.
Materials and methods
Patients
Patients with BPPV who visited the Otorhinolaryngology Department of our secondary institution in Goyang, Korea (longitude: 37.6584; 37°39′30′′ N, latitude: 126.832; 126°49′55′′ E) between 2013 and 2017 were retrospectively enrolled in this study. The enrolled patients had experienced symptoms of spinning vertigo within the previous month and exhibited specific positional nystagmus at their first visit. They had no lesions suspicious of vertigo due to the central nervous system and the possibility of a central pathology was excluded. Positional nystagmus was verified based on the Dix-Hallpike test or the supine roll test. Patients who had etiologies other than BPPV, such as head trauma, VN, labyrinthitis, Ménière’s disease, ear surgery, or sudden sensorineural hearing loss were excluded. If the same patient visited due to BPPV several times during the enrollment period, only the first visit was included in the analysis because of the possibility of other etiologies in recurrent BPPV. The aim of this study was to elucidate monthly and seasonal variations in the onset of idiopathic BPPV.
Monthly and seasonal variations in BPPV
Age, sex, lesion side, the involved semicircular canal, and the month of first BPPV visit were evaluated. Differences among the months and seasons of BPPV visits were analyzed. Spring included March, April, and May; summer included June, July, and August; autumn included September, October, and November; and winter included December, January, and February. For the detailed analysis, patients were divided into two groups according to age (65 years or older and younger than 65 years) and sex, and differences among the months and seasons of BPPV visits were analyzed in each group.
Statistical analysis
Differences among the months and seasons of BPPV visits were analyzed based on the chi square goodness of fit test using IBM SPSS 23 (IBM, Armonk, NY, USA).
Ethical approval
This study was performed in accordance with the 1964 Declaration of Helsinki and its later amend-ments or comparable ethical standards. The institutional review board of the authors’ institution approved this study (NHIMC 2018-CR-039).
Results
In total, 1,216 patients with BPPV were enrolled over the five years; 369 (30.3%) patients were male and 847 (69.7%) were female. The medical records revealed that 692 (56.9%) cases involved the posterior semicircular canal, 315 (25.9%) involved the lateral semicircular canal canalolithiasis, 199 (16.4%) involved the lateral semicircular canal cupulolithiasis, and 10 (0.8%) involved the anterior semicircular canal; while 689 (56.7%) involved the right side and 527 (43.3%) involved the left side. As regards age at diagnosis, 394 (32.4%) were 65 years or older and 822 (67.6%) were younger than 65 years (mean age 57.3±14.4, range 12–92) (Table 1).
Demographic characteristics of patients with benign paroxysmal positional vertigo in this study
Demographic characteristics of patients with benign paroxysmal positional vertigo in this study
The numbers of visits for BPPV were analyzed among months and seasons. There was no significant difference in monthly (p = 0.823) or seasonal distribution (p = 0.670) (Fig. 1).
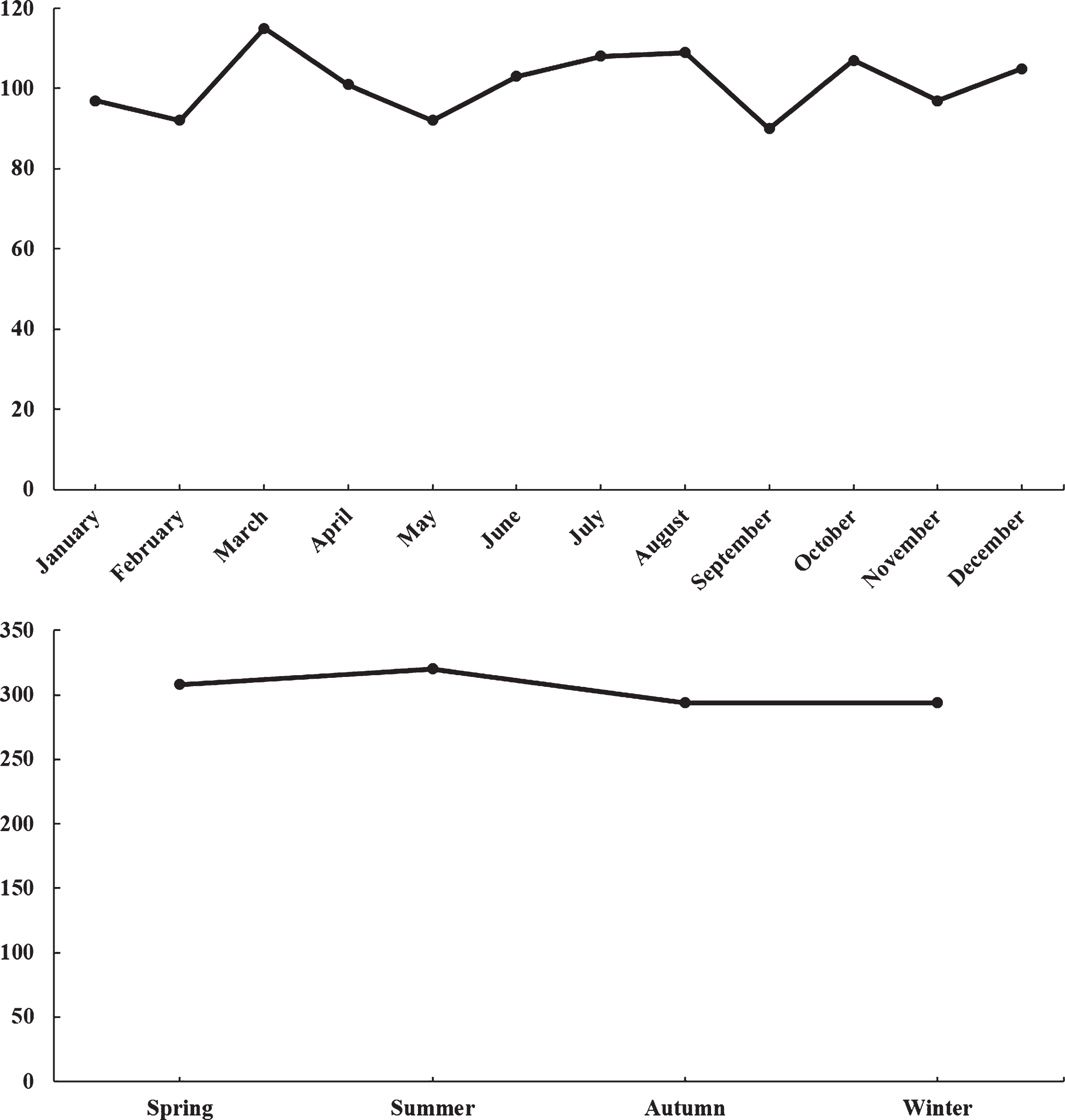
Monthly and seasonal distributions of patients with benign paroxysmal positional vertigo. There was no significant difference in the monthly or seasonal distribution.
The numbers of visits for BPPV were analyzed among months and seasons in the two age groups. There was no significant difference in monthly (p =0.759) or seasonal (p = 0.746) distribution in patients who were 65 years or older. There was also no significant difference in monthly (p = 0.899) or seasonal (p = 0.620) distribution in patients who were less than 65 years old (Fig. 2).

Monthly and seasonal distributions in older and younger patients with benign paroxysmal positional vertigo. There was no significant difference in the monthly or seasonal distribution, neither in patients who were 65 years or older nor in patients who were younger than 65 years. BPPV benign paroxysmal positional vertigo.
The numbers of visits for BPPV were analyzed among months and seasons in both male and female patients. There was no significant difference in monthly (p = 0.499) or seasonal (p = 0.056) distribution in male patients. There was also no significant difference in monthly (p = 0.844) or seasonal (p =0.920) distribution in female patients (Fig. 3).
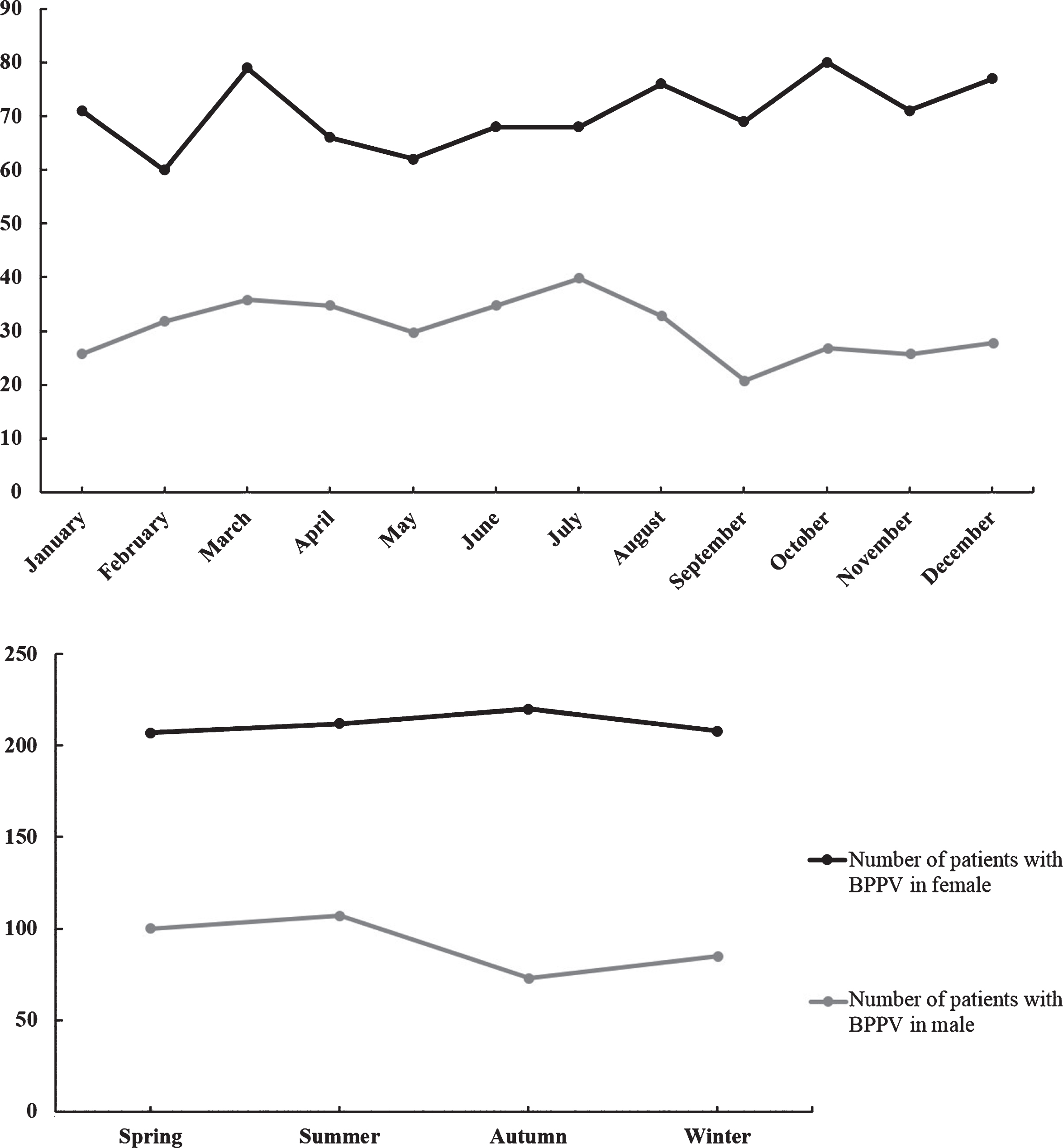
Monthly and seasonal distributions in male and female patients with benign paroxysmal positional vertigo. There was no significant difference in the monthly or seasonal distribution in male or female patients. BPPV benign paroxysmal positional vertigo.
Calcium is a component of otoconia in the utricular macula, and the metabolism of calcium is affected by vitamin D [7, 24]. Vitamin D is compounded mostly in the skin in the presence of sunlight via ultraviolet B radiation exposure. The synthesis of vitamin D in the skin is influenced by skin exposure to ultraviolet B radiation, season, time of day, latitude, altitude, cloud cover, air pollution, clothing, and sunscreen use [12, 24]. Thus, insolation, serum vitamin D levels, and BPPV may be related.
Several studies have reported seasonal variation in BPPV. Whitman and Baloh [20] analyzed 956 visits for BPPV in Boston, MA, USA, over 5 years and reported that the incidence of BPPV was significantly higher during the early spring months of March, April, and May. Saeed and Omari [15] analyzed 207 patients with BPPV in Duhok, Iraq, over 3 years and reported that the monthly distribution of BPPV differed significantly and that the seasonal variation in BPPV was statistically correlated with temperature. Meghji et al. [12] analyzed 339 patients with posterior canal BPPV in Norwich, UK, over 4 years and reported that the onset of BPPV was significantly higher during the low serum vitamin D months (January through June) than during the high serum vitamin D months (July through December). Zuma e Maia et al. [24] evaluated 214 patients with BPPV in Porto Alegre, Brazil, over 6 years and reported that the incidence of BPPV was associated with solar radiation, with more patients with BPPV during the autumn and winter, when there was low solar radiation. Shu et al. [17] evaluated 1,269 patients with BPPV in Shanghai, China, over 6 years and reported that more patients presented with BPPV during the winter than in the summer, and there was a moderate negative correlation between median BPPV patient numbers and serum 25-hydroxyvitamin D levels.
Considering that most BPPV is idiopathic and detachment of otoconia from the utricle is associated with the metabolism of calcium and vitamin D, it is thought that seasonal variation in vitamin D may affect the incidence of BPPV; thus, the incidence of BPPV may show seasonal variation.
Contrary to these studies, Seidel et al. [16] examined 11,153 patients with BPPV in Germany using a large nationwide database and reported no seasonal variation. Although this study was based on diagnostic codes and prescriptions, it included a larger number of patients with BPPV than other studies. Furthermore, the data included in this study represented routine demographic nationwide patients in one country; thus, the results can be used to determine true visits due to BPPV with reduced selection and recall biases. Although many studies demonstrated seasonality of BPPV, this should be re-evaluated in future studies.
Our study was performed in a temperate region with similar meteorological and geographical conditions to the regions in studies by Whiteman and Baloh, Meghji et al., Zuma e Maia et al., Shu et al., and Seidel et al. In our region, the monthly level of solar radiation is highest in May (spring) and lowest in December (winter), with resultant variation in people’s solar exposure. Thus, the variations in levels of solar radiation and solar exposure in our study population were not markedly different from those in previous studies. In our study, similar to previous reports, the number of patients with BPPV tended to increase in March (spring), but this trend was not significant. This conflicts with previous studies, in which the numbers of patients with BPPV in the summer were also high.
There are several explanations for the lack of seasonal variation in BPPV in this study. First, in the etiology of BPPV, viral infection and ischemia may be involved in the onset, although vitamin D may have a major effect. Lee et al. [11] examined population-based big data and reported that the risk of BPPV was higher in patients with sudden sensorineural hearing loss. They suggested that viral neurolabyrinthitis and ischemia could induce BPPV. Viruses and ischemia may also cause idiopathic BPPV, in addition to vitamin D.
Viral infection also causes VN [1, 9]. Several studies that evaluated the association between season and VN are also relevant to an investigation of seasonal variation in BPPV. Koors et al. [9] reported that there was no significant association between month or season and the incidence of VN. Adamec et al. [1] also reported that there was no significant seasonality in VN. Based on these reports, the viral etiology of VN may not be related to season. Considering that viral infection may also be a factor in BPPV, BPPV may not be associated with season. Further study is required to explore the relationship between seasons and BPPV from the perspective of viral infection and ischemia.
Second, during the spring, summer, and autumn, physical activity levels increase compared to the winter. Hanci and Altun [4] reported intensive motocross activity to be a cause of BPPV, without head trauma. Even if a physical activity is not strenuous (e.g., motocross), frequent head movement when using a vehicle and physical activities such as running and ball games could result in detachment of the otoconia from the utricular macula, without direct head trauma, increasing the possibility of BPPV. Some patients may experience unrecognized head trauma during physical activity. Regardless of definite head trauma, the extent of physical activity should also be considered as a factor in BPPV.
Hospital visits due to idiopathic BPPV are associated not only with vitamin D but also with other factors such as viral infection, ischemia, and physical activities. These factors should be considered when the seasonality of BPPV is analyzed.
There are several limitations to this study. First, we retrospectively included data from a single secondary institution. Second, this study included patients with BPPV who had visited our Otorhinolaryngology Department and did not include patients with BPPV who had visited other departments, such as the Neurology Department or the Emergency Department. However, at our institution, most patients who visited other departments were referred to the Otorhinolaryngology Department within 1 week if BPPV was suspected. There was no difference in the waiting period before visiting the Otorhinolaryngology Department according to month or season. Thus, the influence of the waiting period seems to have been negligible in this study.
Despite these limitations, we included a large number of patients with BPPV over a long period and showed that factors that could be associated with the incidence of BPPV (other than vitamin D) should also be considered when evaluating seasonal variation in BPPV. Additional studies on seasonal variation in BPPV are required based on prospective multi-center data or large-scale population-based data.
Conclusion
There was no significant difference in the monthly or seasonal distribution of patients with BPPV. Considering the controversial reports on the seasonality of BPPV, further study of seasonal variation in BPPV is required in terms of not only vitamin D levels but also other factors, such as viral infection, ischemia, and physical activity.
Conflict of interest
None
Funding
This study was funded by a National Health Insurance Service Ilsan Hospital Grant (NHIMC 2018-CR-039).
Ethical approval
This study was performed in accordance with the 1964 Declaration of Helsinki and its later amend-ments or comparable ethical standards. The institutional review board of the authors’ institution approved this study (NHIMC 2018-04-016). Written informed consent was exempted by the institutional review board of the authors’ institution.