
Abstract
BACKGROUND:
The cervical vestibular evoked myogenic potential (cVEMP) can be affected by the recording parameters used to quantify the response.
OBJECTIVE:
We investigated the effects of electrode placement and montage on the variability and symmetry of sternocleidomastoid (SCM) contraction strength and cVEMP amplitude.
METHODS:
We used inter-side asymmetries in electrode placement to mimic small clinical errors in twenty normal subjects. cVEMPs were recorded at three active electrode sites and referred to the distal SCM tendon (referential montages: upper, conventional and lower). Additional bipolar montages were constructed offline to measure SCM contraction strength using closely-spaced electrode pairs (bipolar montages: superior, lower and outer).
RESULTS:
The conventional montage generally produced the largest cVEMP amplitudes (P < 0.001). SCM contraction strength was larger for referential montages than bipolar ones (P < 0.001). Inter-side electrode position errors produced large variations in cVEMP and SCM contraction strength asymmetries in some subjects, producing erroneous abnormal test results.
CONCLUSION:
Recording locations affect cVEMP amplitude and SCM contraction strength. In most cases, small changes in electrode position had only minor effects but, in a minority of subjects, the different montages produced large changes in cVEMP and contraction amplitudes and asymmetry, potentially affecting test outcomes.
Introduction
The cervical vestibular evoked myogenic potential (cVEMP) is an otolithic test of vestibulo-collic reflex integrity and is recorded from the sternocleidomastoid (SCM) muscle using unrectified and rectified EMG averaging techniques [8]. Unrectified EMG averaging is best used to quantify the evoked response, which is a biphasic positive-negative (inhibitory) potential with peak latencies around 13 and 23 ms. Full-wave rectified (or root mean square) EMG is used to determine the underlying level of SCM muscle activity and is measured over the pre-stimulus recording interval.
Quantifying SCM activity is important as a sufficient level is required to record and interpret the cVEMP reflex. This is because the cVEMP represents a short period of inhibition of the underlying SCM motor units [9, 20], and little to no SCM activity would be insufficient to produce a reliable response above the physiological background noise. Changes in the level of SCM activity also alter the size of the evoked response and this relationship has been shown to be linear across moderate levels of SCM muscle activity [2, 16]. This also impacts cVEMP asymmetry, as differences in SCM activity between the sides or individual trials could potentially produce erroneously asymmetries which can lead to false positive (abnormal) results for a disease or condition. Furthermore, measurements of both reflex amplitude and SCM muscle activity will vary depending on electrode position [17, 22].
In this study, we were interested in the differences in cVEMP amplitude and symmetry recorded at three electrode sites over the SCM muscle to air-conducted (AC) sound and bone-conducted (BC) vibration vestibular stimuli. Routine cVEMP testing often results in small interside asymmetries in electrode placement, and we therefore sought to mimic these differences by comparing cVEMP amplitude asymmetries using differing electrode positions between the left and right sides. We were also interested in comparing different methods of measuring SCM muscle contraction strength and how the EMG measurement method affected cVEMP and contraction symmetry.
Materials and methods
Healthy subjects
Twenty normal volunteers with no history of vestibular dysfunction or neurological disease were tested (mean age: 43 years, range: 28 –70 years; 9 males, 11 females). The participants gave informed written consent according to the Declaration of Helsinki and the study was approved by the local ethics committee (X13-0270 & HREC/13/RPAH/354).
Stimulation and recording parameters
We recorded cVEMPs using one AC and one BC stimulus. The acoustic stimulus was an unshaped 2 ms, 500 Hz AC tone burst delivered using TDH-39 headphones (Telephonics Corp., Farmingdale, USA) and a custom amplifier. Stimulus intensity was 133 dB peak SPL (105 dB LAeq). BC stimuli consisted of 6 ms, 500 Hz tone bursts delivered to the forehead at AFz, and were delivered using a minishaker device and amplifier (model 4810; amplifier model 2706, Brüel & Kjaer P/L, Denmark). Both AC and BC stimuli were generated with Signal software and a laboratory interface (micro1401, both from Cambridge Electronic Design Ltd (CED), Cambridge, United Kingdom) and delivered at a rate of approximately 5 Hz for 100 repetitions per trial. For AC stimulation, the left and right ears were stimulated separately and recordings were made from the ipsilateral SCM. For BC stimuli, recordings were made bilaterally from the right and left SCM muscles.
To record cVEMPs, subjects reclined to approximately 20° above horizontal and lifted their head off the bed against gravity. cVEMPs were recorded in two head positions: head straight (BC 500 Hz stimuli) and head turned away from the stimulated ear (AC 500 Hz). SCM muscle activity was recorded bilaterally from three active (inverting) surface electrodes (Cleartrace, Conmed Corp., Utica New York, USA) placed over the SCM muscle belly (Fig. 1A). The main active electrode was placed at 60% of the medial clavicle-mastoid distance (i.e., slightly above the middle of the muscle belly, near the motor point [7]). Two additional electrodes were placed 2 cm above and below this electrode over the SCM muscle. All three recording electrodes were referred to a common medial clavicle electrode on each side, and an earth was placed on the sternum. EMG was sampled at 10 kHz from 20 ms before to 80 ms after stimulus onset, amplified and bandpass filtered (5 Hz to 2 kHz), using 1902 amplifiers (CED) and the same micro1401 data acquisition interface and Signal software as described above. Negative potentials at the active electrodes were displayed as upward deflections.
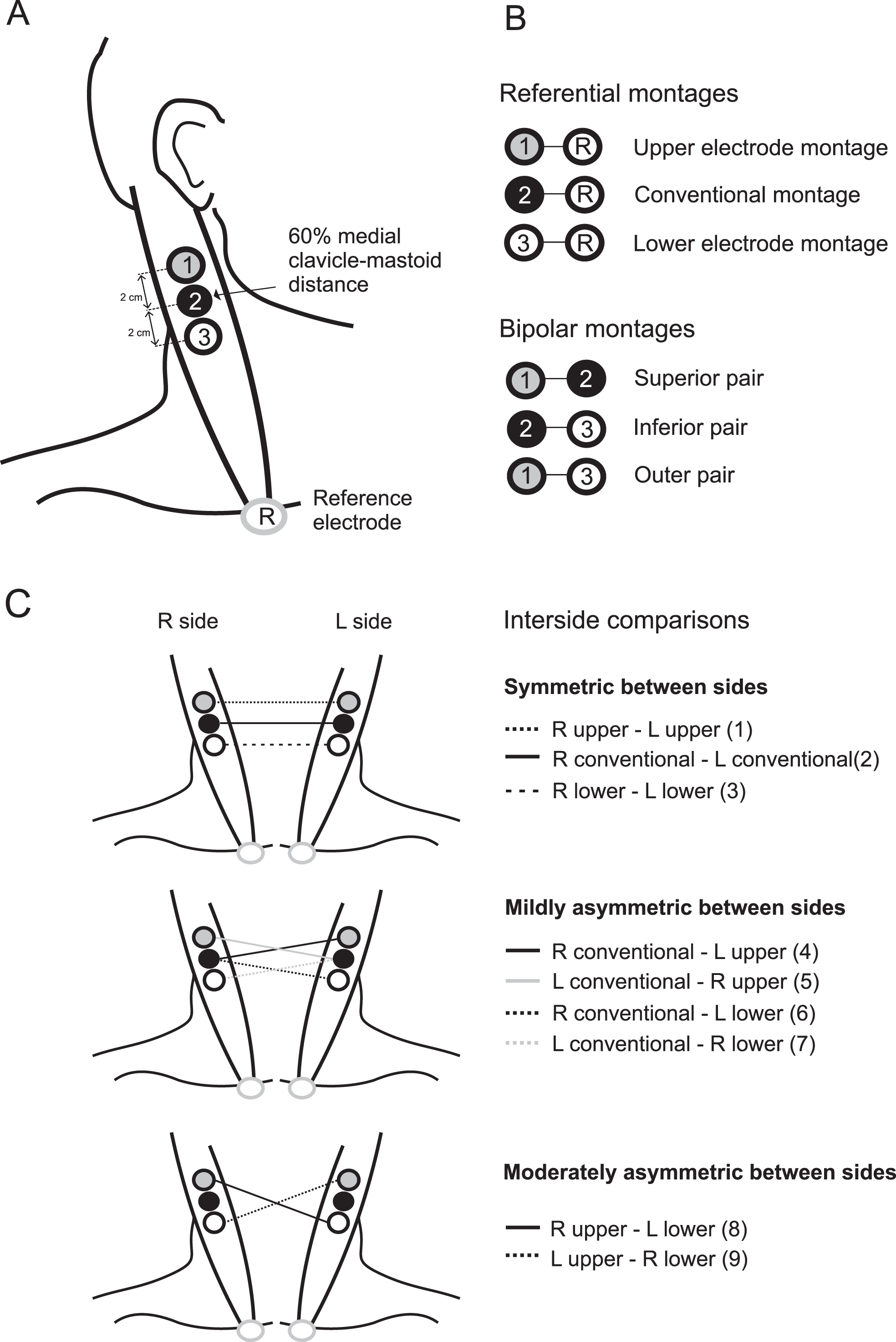
(A) Electrode configurations used for recording SCM contraction strength and cVEMPs. Recording electrodes (1, 2 and 3) were positioned over the sternocleidomastoid muscle. Electrode 2 was placed at 60 % the distance between the insertion points at the mastoid and medial clavicle, and electrodes 1 and 3 were placed 2 cm above and below this position as measured from the midpoint between electrodes. All three recording electrodes were referenced to the reference electrode (R) at the medial clavicle. (B) This produced the three referential montages (1-R: upper montage, 2-R: conventional montage and 3-R: lower montage). Additional bipolar electrode montages for measuring background muscle contraction were also reconstructed offline using electrode pairs positioned over the SCM muscle belly (1-2: superior pair, 2-3: inferior pair and 1–3: outer pair). (C) The nine electrode comparisons used to compare cVEMP asymmetry between the right and left sides. Each of the three referential montages were compared between the sides and classified as being either symmetric, mildly asymmetric or moderately asymmetric.
cVEMPs were recorded from the SCM and compared across the three electrode positions (upper, middle (conventional) and lower) and two sides of stimulation. To measure the cVEMP, amplitudes were measured at the initial biphasic response peaks. Amplitudes were expressed as raw peak-to-peak values and as a ratio of the background activity (amplitude ratio). To assess the effect of interside electrode placement on cVEMP amplitude, we compared cVEMP asymmetries between the left and right sides using symmetric and asymmetric electrode comparisons (Fig. 1C). The electrode comparisons consisted of three types: symmetric (i.e. active electrodes at the same level on both sides, R-L upper (1), R-L conventional (2), R-L lower (3)), mildly asymmetric (i.e. one level apart on each side, R conventional – L upper (4), L conventional – R upper (5), R conventional – L lower (6), L conventional – R lower (7)), and moderately asymmetric (i.e. two levels apart, R upper - L lower (8), L upper – R lower (9)). Two subjects had unilateral absent cVEMP responses to AC 500 Hz and one subject had absent responses to BC 500 Hz. These absent responses were not included in the analyses of cVEMP amplitudes and asymmetries for those stimuli.
To compare different methods of quantifying the SCM muscle contraction, EMG signals from all six referential montage channels were full-wave rectified offline and then averaged over all frames. The mean level of rectified EMG was measured over the 20 ms pre-stimulus period (“mean rectified EMG”). We also measured the strength of SCM contraction across pairs of recording electrodes by re-montaging the data offline to create bipolar montages. This created three new estimates of the contraction strength: the superior montage (difference between the upper and middle electrodes), inferior montage (difference between the middle and lower electrodes) and outer montage (difference between the upper and lower electrodes) (Fig. 1B). We investigated the variability and symmetry of the muscle contraction for each referential and bipolar measure of contraction in all twenty subjects.
Values are given as median [range] unless otherwise specified. Symmetry was calculated using the Jongkees formula for cVEMP and contraction levels: asymmetry ratio (AR)=100*((largest – smallest)/(largest+smallest)). Nonparametric statistics were used for data analyses as approximately 23 % of datasets were not normally distributed. Differences between conditions were tested using the Wilcoxon signed-rank test. Friedman’s ANOVA was used to assess cVEMP amplitude, asymmetry and EMG asymmetry. Chi-square was used to compare frequencies of responses across groups. The coefficient of variation (SD/Mean) was used to compare variability between conditions, electrode configurations and montages, and across electrode configurations within an individual. The significance level was set at α= 0.05, and a Bonferroni correction was used to control for familywise error. Graphs show boxplots (minimum, first quartile, median, third quartile and maximum of data sets) and individual data across the varying electrode configurations and montages.
Results
Effects of electrode placement on cVEMP amplitude using the referential montages
Across the three main referential montages, raw cVEMP amplitudes were generally larger for the conventional compared to the upper and lower montages but individual variations were observed (Fig. 2A and 2B). Median raw cVEMP amplitudes were 125.8μV (upper), 202.1μV (conventional) and 159.0μV (lower) for right ear stimulation, with 16 of 19 subjects (84 %) demonstrating largest amplitudes for the conventional montage (χ2 (2) = 20.2, P < 0.001). For left ear stimulation, median raw cVEMP amplitudes were 161.0μV (upper), 151.0μV (conventional) and 125.0μV (lower) (χ2 (2) = 14.0, P < 0.001), and the conventional bipolar montage produced the largest response in 12 of 19 subjects (63 %). For BC stimulation, median cVEMP amplitudes were 77.0μV (upper), 108.0μV (conventional) and 96.0μV (lower) and for the right SCM (χ2 (2) = 17.2, P < 0.001) and 81.3μV (upper), 102.0μV (conventional), and 70.0μV (lower) for the left SCM (χ2 (2) = 5.3, P = 0.07). Largest BC cVEMP amplitudes were recorded using the conventional montage in 11 of 19 subjects (58 %) for the right SCM and 10 of 19 subjects (53 %) for the left SCM. In one subject the cVEMP amplitude from the L SCM was 2.2 times larger when recorded from the lower compared to the conventional montage (250.0 vs 113.8μV; Fig. 2B, asterisk).
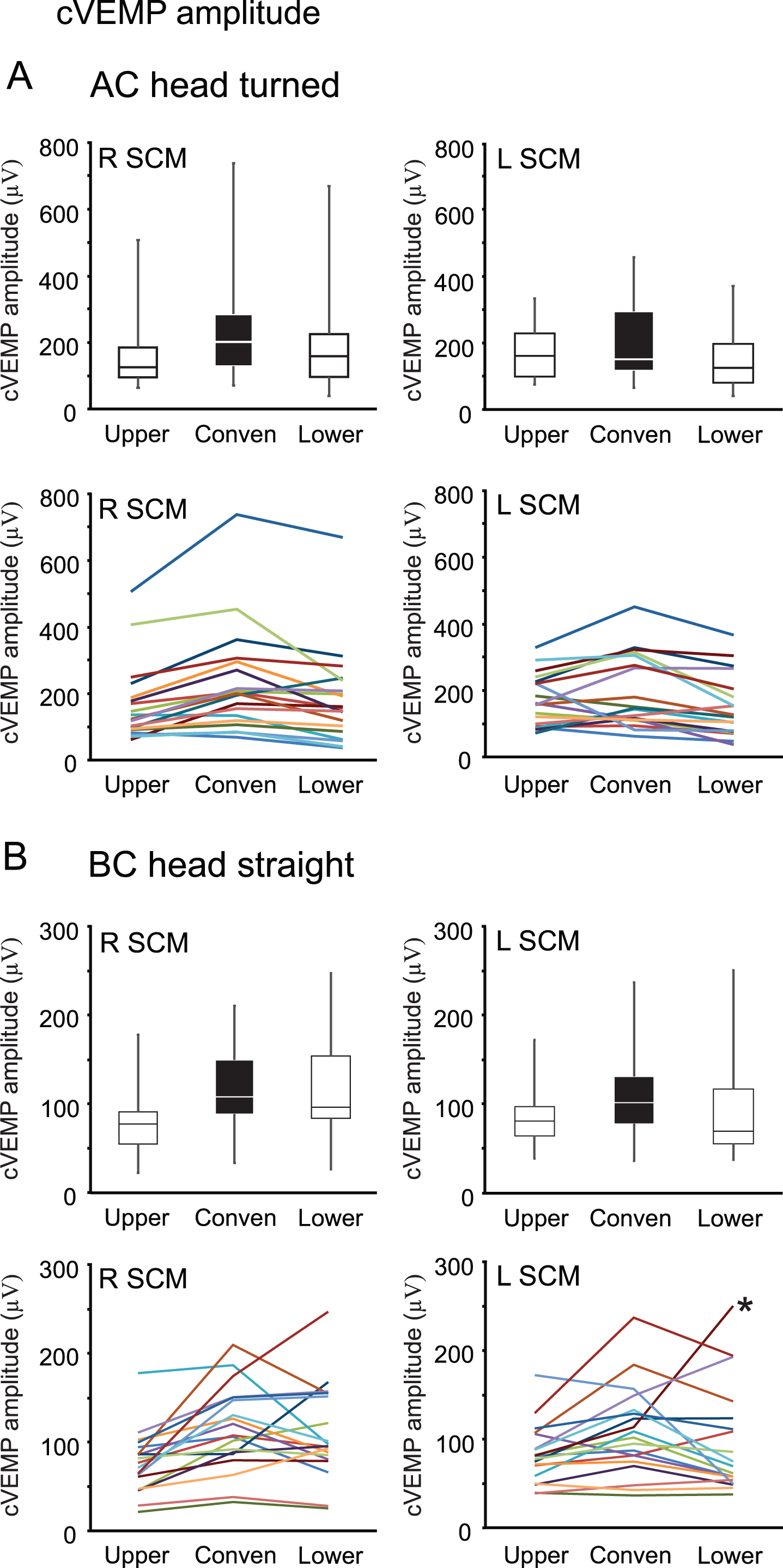
The effect of electrode placement on cVEMP raw amplitude for (A) AC head turned and (B) BC head straight. Results for the right and left SCM are shown in the left- and right-hand columns respectively with individual data in color shown below each boxplot (the same color is used for each individual across the figures). The three referential montages (upper, conventional and lower) were created by using different active electrode positions all referred to the same electrode over medial clavicle. Overall, larger amplitudes were recorded using the conventional (conven) montage. Filled black boxes (in all figures) indicate the conventional bipolar montage, which is used to record cVEMPs clinically. *An individual subject who had much larger BC cVEMP amplitudes with the lower compared to the conventional referential montage.
All subjects had asymmetry values within the normal range, except one, who had asymmetry of 42.1 % using the conventional electrode montage (Fig. 3). To mimic variations in electrode placement we compared cVEMP asymmetries using the three referential montages with varying degrees of asymmetry between the sides (i.e. no asymmetry, mild or moderate asymmetry). When calculated using the conventional montage on either side, for AC stimulation (Fig. 3A) the median cVEMP asymmetry was 12.2 % [0.9 – 56.2 %] for raw amplitudes and 13.0 % [1.7 – 42.1 %] for the amplitude ratio. Overall, cVEMP asymmetries were less variable when using the amplitude ratio compared to raw amplitudes, i.e. after correcting for differences in SCM contraction strength between the sides (coefficient of variation: 0.5 – 0.7 for the amplitude ratio & 0.5 – 0.9 for raw amplitudes). The median AC cVEMP asymmetry did not differ significantly over the nine asymmetry comparisons (Friedman’s test, χ2 (8) = 9.5 (raw amplitude) and 0.33 (amplitude ratio), P > 0.05). For BC stimulation, the results were similar, though the reflexes were more symmetric overall (Fig. 3B). The conventional montage produced median cVEMP asymmetry of 11.5 % [0.0 – 26.4 %] and 9.5 % [0.5 – 26.4 %] for raw amplitude and the amplitude ratio respectively. The BC cVEMP asymmetry differed significantly across the nine comparisons (Friedman’s test, χ2 (8) = 17.0 (raw amplitude) and 17.6 (amplitude ratio), P = 0.03 and 0.02), with the conventional montage on either side producing significantly lower BC cVEMP asymmetries than montage 6 (mildly asymmetric) and montage 8 (moderately asymmetric) for both raw amplitude and amplitude ratio measures (Wilcoxon signed-rank test, Z=–2.9 and –2.8, P = 0.003 and 0.005 for both comparisons, respectively).
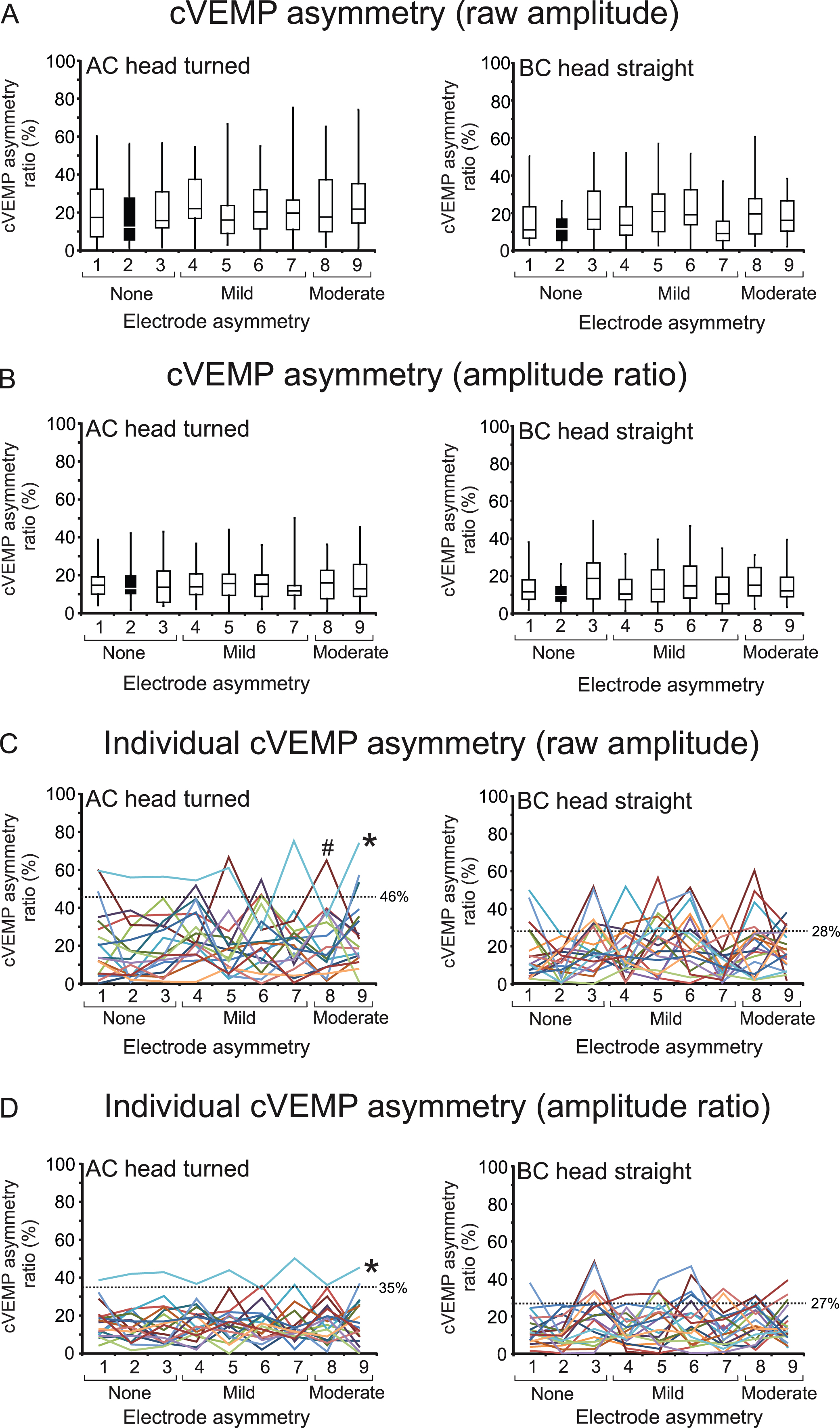
The effect of interside electrode asymmetry on cVEMP asymmetry using raw amplitude (A) and amplitude ratio (B). Individual data across all nine comparisons are also shown for raw amplitude (C) and amplitude ratio (D). The degree of electrode asymmetry is grouped according to three asymmetry levels; none (1–3), mildly (4–7) and moderately asymmetric (8 and 9). All recording electrodes were referred to the conventional reference electrode on the clavicle. Results for AC and BC stimulation are shown in the left- and right-hand columns respectively. Variability in cVEMP asymmetry was much greater across the electrode configurations when using raw cVEMP amplitude and not correcting for differences in SCM contraction strength between the sides. cVEMP asymmetries varied across all asymmetry comparisons, even within symmetric electrode comparisons (1–3). Dashed horizontal lines indicate the upper limit of normal (mean+2 SD) for each modality (AC and BC) and parameter (raw amplitude and amplitude ratio). *An individual subject (light blue line) who exceeded the upper limit of normal for cVEMP asymmetry across the majority of electrode comparisons for both raw amplitude and the amplitude ratio. # An individual subject (brown line) with an abnormal asymmetry ratio in three comparisons. This subject is illustrated in Fig. 4.

Traces from an individual subject showing the comparison of symmetric, mildly asymmetric and moderately asymmetric electrode pairs. The subject (shown by the hash [#] in Fig. 3) had a small cVEMP in the upper position on the right side, which had a significant impact on cVEMP asymmetry calculations. Each comparison with this electrode position produced an asymmetry ratio outside the normal range (upper limit 46% for raw amplitude). The numbers for each pair of traces match those for the different electrode pairs in Figs. 1 and 3.
cVEMP asymmetry did not increase systematically with greater electrode asymmetry. Instead, the pattern of cVEMP asymmetry varied within individuals across all nine comparisons. Even with no asymmetry in electrode position between the sides (i.e. the R-L upper, conventional and lower montages), cVEMP asymmetry varied considerably in individual subjects for both AC and BC 500 Hz stimuli, though it varied least for the conventional montage on each side (comparison 2).
We compared the individual asymmetry ratios in the current study to the upper limits of normal established by a larger sample of previously published normal subjects using a conventional electrode montage [19]. For AC stimulation, the upper limit of normal was 46 % for raw amplitude and 35 % for the amplitude ratio. In the current study, one subject had AC cVEMP asymmetry values exceeding 46 % in seven of the nine comparisons including the conventional montage comparison (1 – 5, 7 and 9; range: [56.2 – 75.4 %]), but would have been considered normal if comparisons six or eight were used (Fig. 3C, asterisk). The remaining subjects all had raw amplitude asymmetry under 46 % when comparing the conventional montage on both sides, but six subjects exceeded the normal limit using alternate asymmetry comparisons, with three of these subjects exceeding the upper limit for two or more asymmetry calculations (Fig. 3C and Fig. 4). In contrast, AC cVEMP asymmetries calculated with amplitude ratios (Fig. 3D) exceeded the 35 % upper limit less often, in only four subjects, and by smaller degrees (three subjects exceeded this value for only one comparison each and were close to the upper limit [comparisons 6, 7 and 9; 35.9, 36.3 and 37.1 % ] while the remaining subject (same as above) was abnormal using eight of the nine comparisons (1–5 and 7–9; range: [36.3 – 50.3 %], Fig. 3D, asterisk).
For BC stimulation, the upper limit of normal asymmetry for the conventional montage was calculated using data from the current study (mean+2SD), and was 28 % for raw amplitude and 27 % for amplitude ratio. For raw amplitude, there were many instances, of cVEMP asymmetries that exceeded the 28 % upper limit, across fifteen subjects. In nine of these subjects the cVEMP had elevated asymmetry for two or more non-conventional asymmetry comparisons (1, 3–9). For amplitude ratio, the variability was lower and eleven subjects had BC cVEMP asymmetries that exceeded the upper limit (across comparisons 1, 3–9). Six subjects exceed the 27 % value for two or more comparisons.
Background contraction levels were generally largest when recorded using the conventional referential montage, followed by the upper and lower referential montages, while the reconstructed bipolar montages (i.e. superior, inferior and outer) produced mostly smaller values (Fig. 5). Contraction levels were larger overall for AC recordings, as the head turning method was employed compared to straight ahead used during BC recordings.
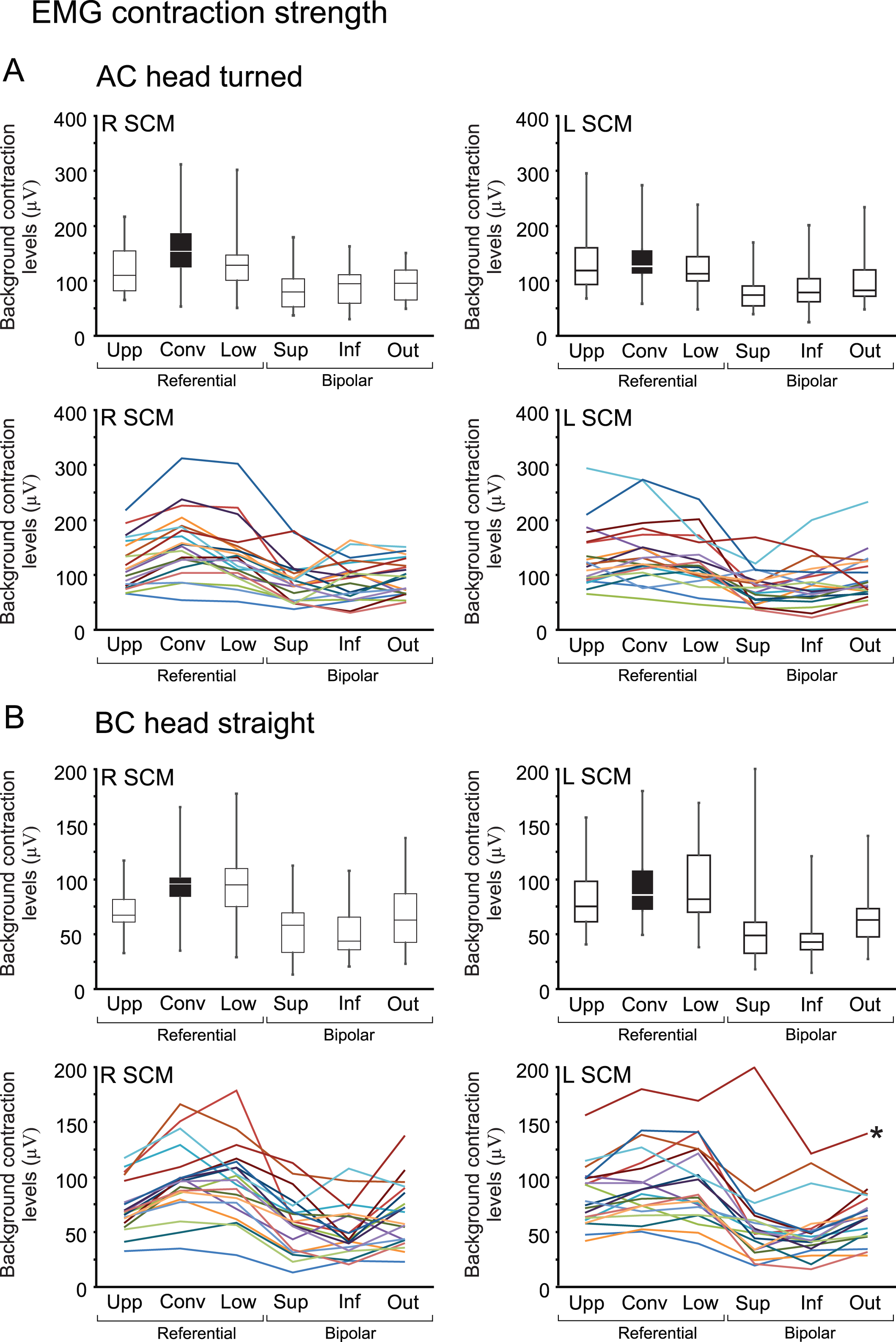
The effect of electrode placement on SCM contraction strength for (A) AC and (B) BC stimulation. Results for the right and left SCM are shown in the left- and right-hand columns, respectively, with individual data shown below each boxplot. The three referential montages included the upper (upp), conventional (conv) and lower (low) configuration, which were all referred to the same electrode over the medial clavicle but utilized differing active electrode positions. Additional electrode montages were constructed offline to produce the superior (sup), inferior (inf) and outer (out) bipolar montages. *A single subject (dark red line) in whom the largest EMG contraction level was recorded using the superior bipolar montage.
For AC stimulation (Fig. 5A), median contraction levels for the right and left SCMs were 110.1 & 117.2μV μV (upper), 153.8 & 124.9μV (conventional), 128.4 & 111.1μV μV (lower), 95.8 & 80.8μV μV (outer), 95.1 & 77.0μV μV (inferior) and 80.2 & 72.2μV (superior). Overall, 17 of 20 subjects (85 %) demonstrated largest contraction levels for the conventional montage for the R SCM (Friedman’s test, χ2 (5) = 56.6, P < 0.001) and 8 of 20 subjects (40%) for the L SCM (Friedman’s test, χ2 (5) = 44.7, P < 0.001). For both the right and left SCMs, the referential montages averaged together produced significantly larger contraction levels than the bipolar ones averaged together (Wilcoxon signed-rank test, Z=–3.9 and –3.8, P < 0.001 for both comparisons).
For BC stimulation (Fig. 5B), median contraction levels for the right and left SCMs were 67.5 & 75.6μV (upper), 96.0 & 86.1μV (conventional), 95.2 & 82.1μV (lower), 63.0 & 63.4μV (outer), 58.4 & 49.2μV (superior) and 43.8 & 43.2μV (inferior). Overall, the conventional montage produced the largest contractions in 10 of 20 subjects (50%) for the R SCM and in 6 of 20 subjects (30 %) for the L SCM (Friedman’s test, χ2 (5) = 63.1 & 74.0, P < 0.001). The referential montages produced significantly larger contraction levels than the bipolar montages (Wilcoxon signed-rank test, Z=–3.9 (R and L SCM), P < 0.001 for both comparisons). In one subject, background contraction levels from the L SCM were largest for the superior bipolar montage but varied considerably across the referential and bipolar montages (Fig. 5B, asterisk).
We also examined the effect of small changes of electrode position on asymmetry of the background contraction measure. Median EMG asymmetry was 14.0 [1.0–22.4] % for AC stimulation and 7.2 [1.1–24.5] % for BC stimulation when using the symmetric R-L conventional montage. Overall, EMG asymmetries did not differ significantly across the nine electrode comparisons for AC stimulation (Friedman’s test, χ2 (5) = 0.7, P = 0.985) and showed a weak effect for BC stimulation (Friedman’s test, χ2 (5) = 11.5, P = 0.042). Much like cVEMP asymmetry, SCM contraction asymmetry did not simply increase with greater electrode asymmetry (Fig. 6). For AC stimulation, two subjects had EMG asymmetries that exceeded the upper limit of normal (35 %) for the actual cVEMP amplitude ratio (recorded with comparisons 1, 5 and 7–9 [range: 38.3 – 43.7 % ]). Similarly, for BC stimulation, five subjects had EMG asymmetries that exceeded the upper limit of normal (27 %) for the BC cVEMP (recorded with comparisons 1, 3, 5 and 8 [range: 28.8 – 30.7 % ]).
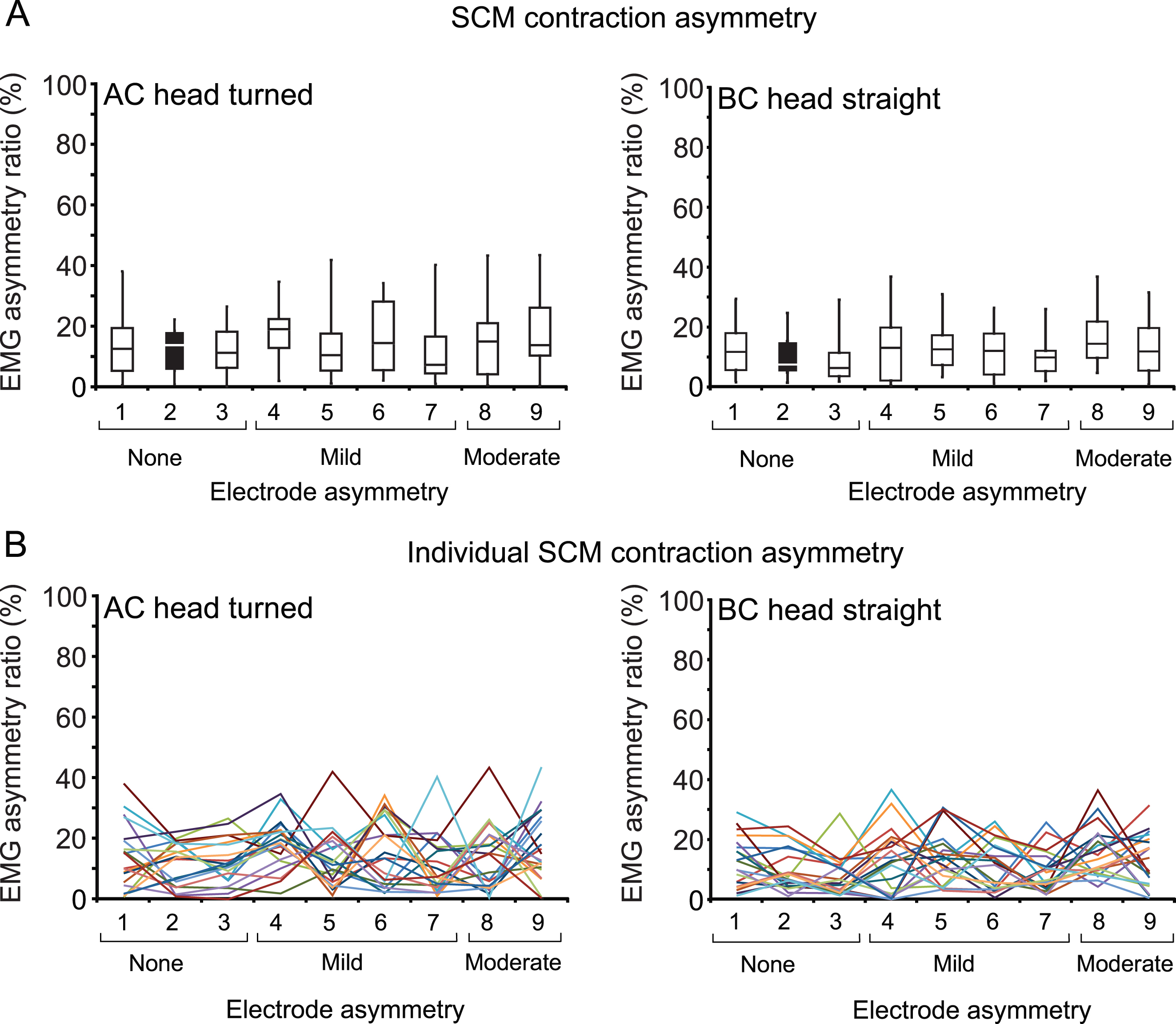
The effect of interside electrode asymmetry on SCM contraction asymmetry values. Individual data across all nine comparisons are also shown (B). The degree of electrode asymmetry is: none (1–3), mildly (4–7) or moderately asymmetric (8 and 9). Results for AC and BC stimulation are shown in the left- and right-hand columns respectively.
Amplitude ratios were calculated using raw cVEMP amplitudes recorded from the conventional montage and expressed against each of the six different contraction estimates for each side (Fig. 7). For AC stimulation, median amplitude ratios were 1.3 [0.5 – 3.2] and 1.3 [0.6 – 3.1] for the right and left SCMs respectively using the conventional montage for both cVEMP amplitude and SCM contraction measurement. There were significant differences in amplitude ratios across the differing measures of EMG activity for both the right and left SCMs (Friedman’s test, χ2 (5) = 52.9 & 43.8, P < 0.001). Overall, using the measure of EMG derived from the same electrode pair as the reflex produced the smallest amplitude ratios with the least variability (i.e. Fig. 7 “conv/conv”). Using an additional active electrode just above or below the conventional active electrode (but similarly referred to the clavicle) to estimate EMG produced slightly higher amplitude ratios, as the EMG recorded here was generally weaker (i.e. Fig. 7 “conv/upp” and “conv/low”). Finally, EMG measured using two electrodes across the belly of the muscle (bipolar montages) produced the largest amplitude ratios with greatest variability, as these montages produce much lower estimates of EMG activity (Fig. 7 “conv/sup”, “conv/inf” and “conv/out”). Likewise, for BC stimulation (Fig. 7B), there were significant differences in amplitude ratios across the differing measures of amplitude ratio for both sides (Friedman’s test, χ2 (5) = 62.4 & 68.9, P < 0.001), following a similar pattern to AC stimulation.

Using different measures of background SCM contraction to calculate the cVEMP amplitude ratio. Boxplots are shown for AC (A) and BC (B) stimulation, with responses from the right and left SCMs shown in the left and right columns respectively. Individual data are also shown below each boxplot. The cVEMP amplitude ratio was calculated by expressing the raw [cVEMP] response amplitude recorded from the conventional montage (conv) as a ratio of the [EMG] background contraction. EMG contraction levels used were measured using the conventional, upper (upp), lower (low), superior (sup), inferior (inf) and outer (out) montages.
Median cVEMP asymmetries were 13.0 % [1.7 – 42.1 %] for AC stimulation and 9.5 % [0.5 – 26.4 %] for BC stimulation using the conventional montage for both cVEMP amplitude and SCM contraction measurement (Fig. 8A). Overall, median cVEMP asymmetries were not significantly different across the six measures of cVEMP asymmetry (Friedman’s test, χ2 (5) = 6.0 & 6.6, P = 0.308 & 0.251, for AC and BC stimuli respectively), however, variability was greater for calculations using EMG measures from bipolar montages across the muscle belly and significant variations were observed amongst individuals (Fig. 8B). The coefficient of variation was 0.6 (conv/conv), 0.7 (conv/upp, conv/low, conv/inf, conv/out) and 0.8 (conv/sup) for AC stimuli and 0.7 (conv/upp, conv/conv, conv/low, conv/inf, conv/out) and 0.9 (conv/sup) for BC stimuli.
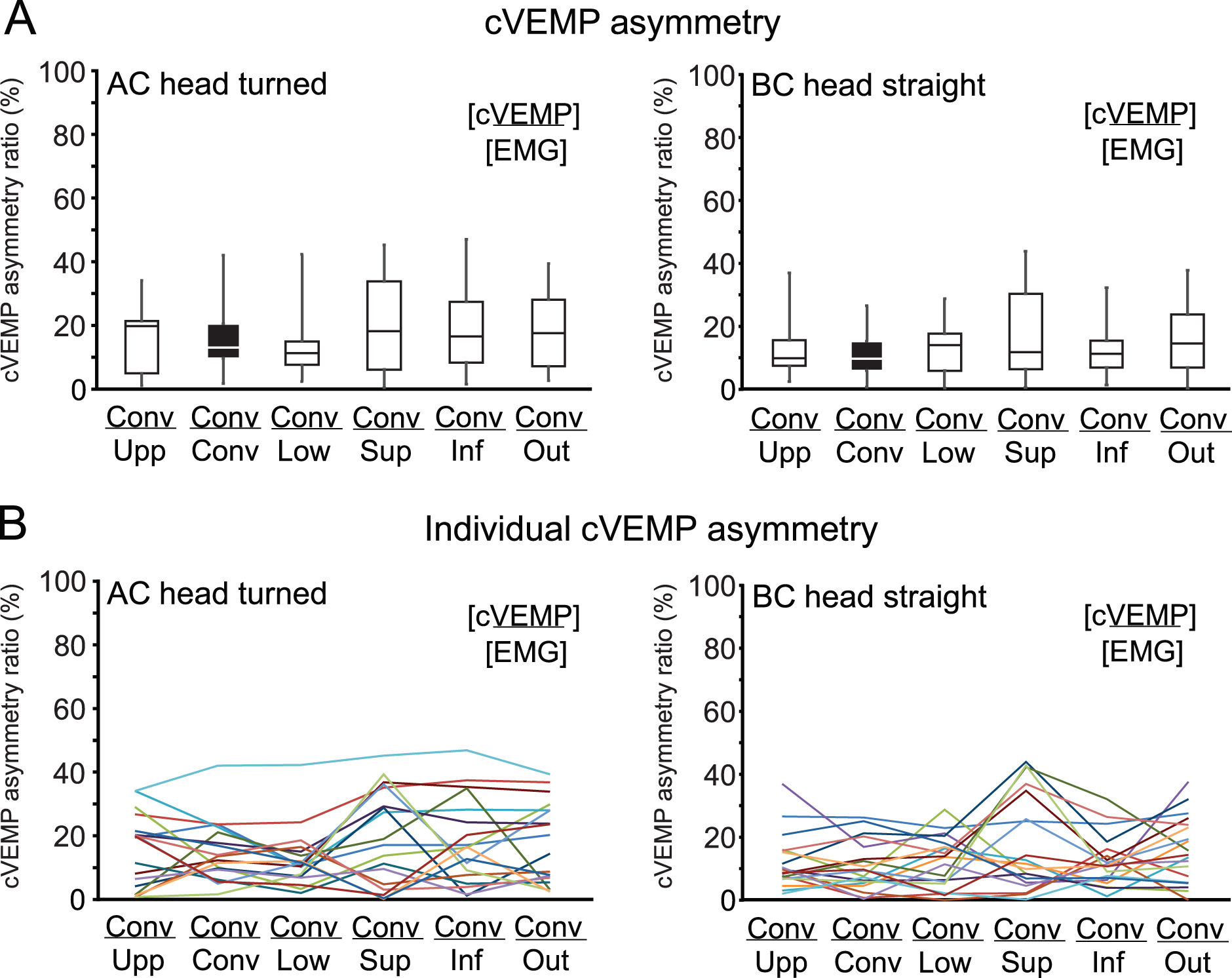
The effect of quantifying EMG contraction levels using different electrode configurations on cVEMP asymmetry ratio. Findings for AC and BC stimulation are shown in the left and right columns respectively. cVEMP asymmetries were calculated using SCM contraction levels determined from the conventional (conv), upper (upp), lower (low), superior (sup), inferior (inf) and outer (out) montages.
The cVEMP is an established otolith-dependent measure of vestibulo-collic reflex function [8, 21]. We have shown that the electrode montage affects measures of amplitude and symmetry for both the reflex and the estimate of muscle contraction. While in the majority of subjects cVEMP amplitudes and estimates of SCM contraction strength were similar across the different electrode comparisons, in some subjects there were large differences with small changes in electrode position. Similarly, while in most cases the reflex was quite symmetric, in some subjects the asymmetry of cVEMP amplitude and SCM contraction strength showed marked changes with different electrode comparisons.
Conventional montage vs nearby electrode positions
The conventional cVEMP electrode montage consists of a recording (active or inverting) electrode over the SCM muscle belly, close to the motor point, and a reference (indifferent or non-inverting) electrode over the distal SCM tendon [8]. Colebatch et al. [7] determined the average location of the SCM motor point to be approximately 60 % of the distance between the mastoid and sternoclavicular joint (9–12.5 cm above the sternoclavicular joint), and we have used this as the active electrode position for our conventional referential montage. Of the three referential electrode montages (conventional, upper and lower), the conventional montage produced the largest cVEMP amplitudes, in 53 –84 % of subjects across both sides and stimulus modalities. This is because the response is largest near the motor point and becomes smaller as the recording electrode is moved away from this point [17, 22]. The variability is likely due to differences in the location of the motor point across individuals [10, 25], which we did not measure.
Variability in cVEMP asymmetry was observed across electrode montages which mimicked small interside electrode asymmetries. This was employed to simulate the minor differences in electrode placement that would sometimes occur in clinical practice. The lowest cVEMP asymmetry values with the least variability were typically recorded using the conventional montage, demonstrating the importance of proper positioning of surface electrodes between the right and left SCM muscles. cVEMP asymmetries are used to quantify suspected otolithic dysfunction and abnormal asymmetries reflect values which exceed the upper normal limits defined by healthy controls. The upper limits of normal used in the present study were calculated using the conventional montage and are consistent with those previously reported [12, 24]. We have shown that small asymmetries in electrode position between the sides can produce cVEMP asymmetries that exceed the upper normal limits in some subjects. Likewise, with small changes in electrode position (Fig. 6), some subjects had muscle contraction asymmetries that approached or exceeded the upper normal limit for cVEMP amplitude ratio asymmetry. In these subjects, any underlying otolith asymmetry (the actual target of the test) would combine with this contraction asymmetry and potentially cause false positive (abnormal) test results (or mask actual positive test results).
For both modalities, more individuals had cVEMP asymmetries that exceeded the upper normal limit using raw amplitudes compared to the amplitude ratio. This demonstrates the greater potential for variability in cVEMP asymmetry when differences in SCM contractions between the sides are not controlled or corrected for, and shows that using raw values can lead to larger numbers of false positive test results. This is despite accounting for the wider normal limits set for cVEMP asymmetries when using raw amplitudes [12, 24].
Alternate measures of background contraction
SCM contraction strength affects cVEMP amplitude, latency and asymmetry [16], and direct measurements of the underlying SCM contraction strength provide a good way of ensuring that the muscle activity is adequate and reasonably symmetric. In the current study, measuring the background contraction levels from electrode pairs other than the conventional montage (i.e. electrodes near the motor point and medial clavicle) generally resulted in lower estimates of EMG. While the differences were subtle for the referential montages, more substantial differences were evident for the bipolar montages calculated offline (i.e. the superior, inferior and outer pairs). This is because closely spaced electrodes subtract out much of the underlying activity due to common mode rejection. Variability was also an issue for a minority of subjects using the bipolar montages, (Fig. 5B, lower panels), where there could be large differences between the superior and inferior pairs. These effects are likely to be due to placement of the electrode pairs on different sides of or across the motor point [15]. As a result of dividing by smaller numbers, the amplitude ratios calculated using our bipolar measures of contraction were larger and more variable, and cVEMP asymmetries were also more variable.
Our results are consistent with previous reports of SCM muscle activity measured during cVEMPs. While the cVEMP reference electrode is usually placed at or near the sternoclavicular joint, some previous studies have employed other distant reference locations to record cVEMPs or quantify SCM contraction strength. These have included the wrists [6, 23], hands [26], chin [14] and forehead [13]. As most of these sites are inactive they generally produce similar contraction estimates to the sternoclavicular joint [17]. Other studies have used a bipolar montage, similar to the ones used in the current study but with 1 cm between electrode bars [1–5]. These studies report SCM contractions in the range of approx. 30–90μV, which are associated with higher amplitude ratios. This close bipolar montage has the advantage of limiting the contribution of EMG activity from nearby non-target muscles, but produces smaller estimates of EMG that may be more sensitive to small changes in electrode position. Use of local normative values collected with the same montage will accommodate these different amplitudes and greater variability. But caution is warranted in directly comparing the cVEMP amplitudes and contraction strengths between studies, as the ranges may differ significantly depending on such montage differences.
Conclusion
Our results show that in most cases, small changes in electrode placement will have very little effect on cVEMP properties and test outcome. However, care should be taken in the correct and symmetric placement of recording electrodes for cVEMPs, as in a minority of patients asymmetric placement across the two sides may erroneously increase cVEMP asymmetry. For any systematic change in electrode montage, a different upper limit of normal will be required, particularly if a bipolar montage is used.
Footnotes
Acknowledgments
Dr Sally Rosengren was supported by the National Health and Medical Research Council of Australia (GNT1104772, GNT1058056).