
Abstract
BACKGROUND:
Evidence to support potential links between chronic otitis media (COM) and vestibular impairment/postural balance control issues is lacking.
OBJECTIVE:
To investigate whether COM associates with vestibular symptoms, balance problems, and abnormalities in vestibular function tests.
METHODS:
We selected 126 patients with COM and excluded patients with any identifiable underlying causes for vestibular dysfunction. Fifty-two healthy volunteers were included as controls. All subjects underwent anamnesis, physical examination, posturography, and video-head impulse tests.
RESULTS:
We found a high prevalence of vestibular symptoms (58.4%) among patients with COM, while only 2% of the controls had vestibular symptoms. There was a positive correlation between COM activity with the presence of tinnitus and vestibular symptoms (P < 0.05). Clinical vestibular tests were abnormal in 63% of patients with COM, and those positively associated with presence of vestibular symptoms. Posturography results shown worse postural balance control in patients with COM as compared with controls, especially in the limit of stability (LOS) (Mean LOS, COM = 157.56 cm2; controls = 228.98 cm2; p < 0.001) and worse results in the test with eyes closed while standing on a foam mattress (sway area, COM = 10.91 cm2; controls = 5.90 cm2; p < 0.001) in patients with COM as compared with controls. We did not observe differences in the average vestibuloocular reflex gains in the video-head impulse test between our COM and control groups.
CONCLUSIONS:
Our results show that COM associates with higher prevalence of vestibular symptoms and abnormalities in clinical vestibular function tests, and worse postural control as compared with controls. Among patients with COM, the activity of the middle-ear inflammation seemed to positively associate with the severity of hearing and balance problems.
Introduction
Chronic otitis media (COM) is a disease with high prevalence worldwide [33] – its incidence is estimated at 4.8 new episodes per 1000 people every year. Patients with COM are under risk of developing acute complications [30, 41] and long-term sequelae [1, 38], which include tinnitus and hearing loss.
The association between sensorineural hearing loss and COM has been demonstrated by several histopathologic and clinical studies in the past [14, 38]. More recently, it has been hypothesized that COM may associate with vestibular symptoms as well [20, 47]. However, a recent systematic review observed that most of the studies dedicated to evaluate links between vestibular symptoms and COM had several potential biases, which may have compromised their results [34]. Thus, the objective of this study is to investigate, based on a systematic research protocol, whether or not COM associates with vestibular symptoms, postural balance problems, and abnormalities in vestibular function tests.
Materials and methods
Design and ethical considerations
This study protocol was approved by the Institutional Review Board of our university (n.1.751.916). We conducted a cross-sectional, controlled study at a tertiary care referral center, from August 2016 to November 2018.
Patient selection
From our otology outpatient clinic, we selected consecutive patients with COM that complied with our inclusion and exclusion criteria. Patients with COM were identified by the presence of chronic infection/inflammation of the middle ear cleft and perforation of tympanic membrane [5, 6]. We excluded volunteers who (1) were less than 18 years; (2) had any identifiable cause for vestibular symptoms (past use of ototoxic medication, clinical otosclerosis, definite or probable Meniere’s disease, definite or probable vestibular migraine, perilymphatic fistula, untreated metabolic or cardiovascular diseases, diabetes or glucose intolerance, benign paroxysmal positional vertigo, head trauma or traumatic head blast injury, neurologic or neurodegenerative diseases, and syphilis); (3) had a history of otologic surgery (except ventilation tubes); (4) had cognitive deficits; (5) had genetic syndromes or otologic malformations; (6) had significant past noise exposure or acoustic trauma; (7) had cancer or underwent past chemotherapy or radiation therapy; and (8) had orthopedic or visual limitations.
Clinical evaluation
Patients with COM underwent a systematic clinical, laboratory, and imaging evaluation. We collected demographic (sex, age, ethnicity) and other relevant information, such as presence of tinnitus, vestibular symptoms (and its characteristics, triggers and worsening factors), and frequent episodes of otorrhea. Vestibular symptoms were classified as per the guideline proposed by the B
Subjects with COM were categorized in 3 groups: (1) chronic perforation of the tympanic membrane (CPTM) caused by otitis media, with infrequent suppuration; (2) chronic suppurative otitis media (CSOM), defined as frequent or intractable ear suppuration through a tympanic membrane perforation without cholesteatoma; and (3) COM with cholesteatoma. Patients with adhesive otitis media without cholesteatoma were not included in our study. We also defined as “active” COM when patients had signs of active middle ear inflammation, including presence of intense hyperemia and suppuration –by definition, CPTM cases were all “inactive”. Patients with bilateral COM groups were categorized using the following protocol: (1) at least one ear had cholesteatoma –cholesteatoma group; (2) at least one ear had CSOM, none had cholesteatoma –CSOM group; (3) both ears had CPTM –CPTM group.
With the same inclusion and exclusion criteria used for the COM groups, we also selected volunteers with no history of ear disease using a convenience sampling method, who were included in a control group. Subjects in the control group underwent the same routine of clinical, hearing, and vestibular testing used for the COM group.
Evaluation of vestibular function
To evaluate postural balance control and analyze vestibular function, we performed static posturography (Balance Rehabilitation Unit –BRU; Medicaa; Montevideo, Uruguay) and video-head impulse (video-HIT) (Otometrics A/S; Taastrup, Denmark) tests. Considering that our group of subjects ranged from healthy volunteers to patients with severe middle-ear abnormalities, we did not use caloric testing and vestibular evoked myogenic potentials (VEMPs). The posturography and video-HIT tests were selected because their results are not influenced by the presence of middle-ear disease.
The static posturography of the BRU allows an objective assessment of the postural control/vestibulospinal reflex [12]. A force platform measures displacement of the center of pressure, while patients are exposed to somatosensorial (eyes closed, standing on a medium density foam mattress with eyes closed), vestibular, and visual (saccadic, optokinetic) stimuli. The postural control is analyzed under 3 parameters: (1) limit of stability (LOS) = area in which the volunteers can intentionally dislocate their center of pressure (cm2); (2) sway area = area comprising 95% of the dislocations of the center of pressure in each specific test (cm2); and (3) sway velocity = total distance of dislocation divided by the duration of the test (cm/s).
The video-HIT is a bedside test used to evaluate function of the semicircular canals, providing objective measures of the gain of the vestibulo-ocular reflex (VOR) for each canal separately [28]. The number of movements toward each desired semicircular canal was set to 20. When artifacts were identified, the test was repeated one more time. Tests were performed by one of the authors, who has extensive experience in video-HITs. All individual impulses collected were stored and assessed for artifacts [29] by a blinded researcher, also with extensive training in video-HITs. Results were considered abnormal when VOR gain was less than 0.8 (horizontal canals) or 0.7 (vertical canals) and corrective saccades were present.
Statistical methods
All results obtained with the anamnesis, physical examination, and vestibular/postural testing in both COM and control groups were subjected to comparative analysis. Categoric variables were compared using Pearson’s x2 test and, when necessary, we performed the post-hoc cellwise residual analysis test [18]. The distribution of numerical data was assessed using Shapiro-Wilk test –normally distributed data was analyzed using independent t-tests or ANOVA with Tukey’s post-hoc test, and non-normal data was analyzed using Mann-Whitney U, Kruskal-Wallis test with Dunn-Bonferroni post-hoc pairwise comparisons, or Spearman’s rank coefficient test. All tests were carried using the IBM SPSS v. 23.0 Statistics software (Armonk, NY; IBM Corp). Results were considered statistically significant when the value of P was less than 0.05.
Results
Demography
Our final COM group comprised of 126 patients with COM –demographic information is listed in Table 1. Among the 39 patients with cholesteatoma, 28 (71.7%) had active signs of middle ear inflammation and 11 (28.3%) did not. We did not find significant age differences among our study and control groups (p = 0.34).
Demography information, frequency (%) of clinical complaints reported by volunteers of the COM and control groups and otoscopy findings
Demography information, frequency (%) of clinical complaints reported by volunteers of the COM and control groups and otoscopy findings
CPTM = Chronic perforation of the tympanic membrane; CSOM = Chronic suppurative otitis media; COM = Chronic otitis media; TM = tympanic membrane.
The most frequent symptoms among patients with COM were hearing loss and tinnitus (Table 1), and the prevalence of those symptoms in our COM patients was significantly higher as compared with the control group (P < 0.001). We did not find differences in prevalence of tinnitus among the COM subgroups (P = 0.102).
The overall prevalence of vestibular symptoms in the COM groups was 58.4%; in the control group, prevalence was 2.0% (P < 0.001) (Table 1). The characteristics and frequency of the vestibular symptoms among patients with COM are depicted in Fig. 1. Among the COM subgroups, vestibular symptoms were more frequent in patients with CSOM (77.7%) and cholesteatoma (64.1%) as compared with CPTM (46.6%) (P = 0.037). Triggers for the vestibular symptoms were reported by 65% of the patients with COM –the most frequent trigger was the onset or worsening of otorrhea (75%). Other triggers were positional (21%), unspecific headache (4%) and driving (2%). In our COM groups, the presence of tinnitus associated with a 2-fold increase in the risks of patients complaining of vestibular symptoms (Relative Risk [RR] = 2.63; 95% CI, 1.60–4.33; P < 0.001). We did not find a significant association between the presence of vestibular symptoms and laterality (unilateral or bilateral COM), sex, or race (P > 0.05).
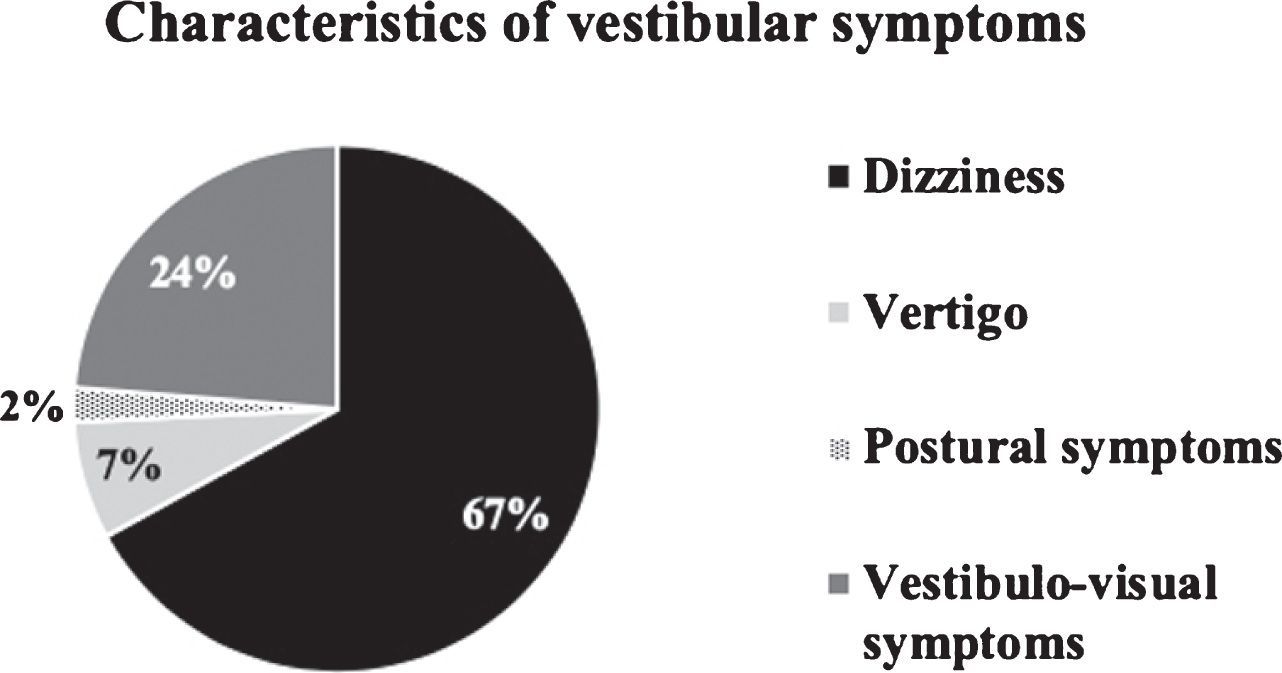
Characteristics of the vestibular symptoms among patients with COM (N = 74; 58.7%).
Results of audiometric evaluation are in Table 2. Patients with COM had worse pure-tone averages (PTA) and speech discrimination scores in all COM groups as compared with controls (P < 0.05). Among COM groups, patients with CSOM or cholesteatoma had significantly worse PTA (P = 0.006 and P = 0.009) scores than patients with CPTM. We did not find significant differences in speech recognition scores (P = 0.264) among the COM subgroups. Four of the volunteers from the control group (mean age = 58.75 years) had a mild sensorineural hearing loss affecting the frequencies above 4 kHz (mean speech recognition thresholds = 12.5 dB; mean speech discrimination scores = 98%), suggesting presbycusis.
Results of audiometric evaluation in the study and control groups, expressed as type of hearing loss, pure-tone average (PTA) and speech discrimination score
Legends: CPTM = chronic perforation of tympanic membrane; CSOM = Chronic suppurative otitis media; COM = Chronic otitis media. Light gray cells, *=significant difference (P < 0.05) as compared with controls. Dark gray cells, *=significant (P < 0.05) difference as compared with the CPTM and control groups.
We found no differences in the prevalence of conductive as compared with mixed hearing loss among our COM subgroups (P > 0.05). But the presence of mixed hearing loss significantly associated with worse PTA and speech discrimination scores (P < 0.001 and P = 0.019, respectively) as compared with conductive hearing loss. The type of hearing loss did not correlate significantly with presence or absence of tinnitus or vestibular symptoms (P > 0.30).
Among patients who had tinnitus, PTA was also significantly worse as compared with patients without tinnitus (45.5 dBNA and 38.1 dBNA, respectively; P = 0.024). We did not find differences in speech recognition scores between (1) patients with and without tinnitus (P > 0.05), and (2) patients with and without vestibular symptoms (P > 0.05).
Table 1 summarizes the otoscopy findings in the COM and control groups. Among patients with COM, only 4 volunteers did not have tympanic membrane perforation, all of which were from the cholesteatoma group. In those patients, otoscopy showed attic retraction pocket, local bony erosion, and presence of the characteristic pearly-white mass suggestive of cholesteatoma.
We found abnormalities in the clinical vestibular and cerebellar function tests in 63% of patients with COM. Those abnormalities correlated significantly with the presence of vestibular symptoms (P = 0.002; 95% CI = 0.108–0.458). The test which was most frequently abnormal was the Fukuda stepping test (62%), followed by instability in the Romberg test (12%), and presence of corrective saccades in the head impulse test (1.6%). The presence of abnormalities in the clinical vestibular tests did not associate significantly with type of hearing loss (conductive or mixed), laterality (unilateral or bilateral), or presence of tinnitus (P > 0.05).
The mean SVV results were above reference values (±2°) in all COM groups, and within normal among controls (Fig. 2); the difference between SVV results in patients with COM and controls was statistically significant (P < 0.001). But we found no significant differences in pairwise comparisons among our COM subgroups (P > 0.05). We did not find significant correlations between the SVV results and presence/absence of tinnitus, presence of vestibular symptoms, and abnormalities in clinical vestibular tests (P > 0.05).
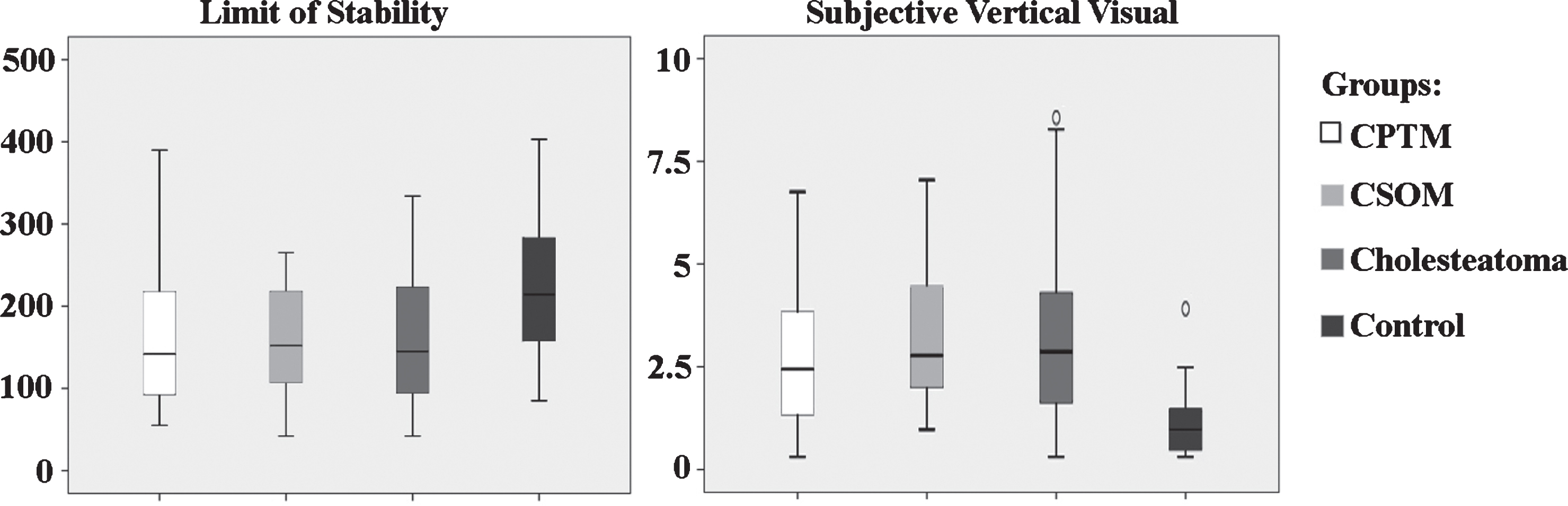
Left: boxplot graphic results obtained with the posturography test regarding the limit of stability (LOS) of the study and control groups. Right: boxplot graphic results showing results obtained with the subjective vertical visual using the “bucket test”. *=statistically significant difference (P < 0.05) as compared with the control roup.
The posturography test showed that all COM groups had worse LOS results as compared with controls (Fig. 2, Tables 3 and 4) (P < 0.05). We also observed that –in the CSOM and cholesteatoma with active middle ear infection groups –the sway areas and sway velocities were significantly increased in the majority of posturography test as compared with controls (P < 0.05) (Fig. 3, Table 3). On the other hand, the posturography results in the CPTM and cholesteatoma (with and without active infection) only yielded statistically significant differences as compared with controls under few specific stimuli (Table 3). We observed that the sway area and sway velocity were significantly worse in the CSOM group as compared with the CPTM group in several posturography tests (eyes closed, eyes closed while standing on a foam mattress, and optokinetic tests) (Table 4). The test with eyes closed while standing on a foam-mattress was the most challenging and yielded higher sway area/velocity in both COM and control groups (Fig. 3); 3 volunteers from the CSOM group needed support from the harness during this test.
Values of significance (P values) obtained from the comparisons of posturography test results in volunteers with COM and controls, as the result of Kruskal-Wallis analysis of variance and Dunn-Bonferroni post-hoc’s pairwise comparisons
Values of significance (P values) obtained from the comparisons of posturography test results in volunteers with COM and controls, as the result of Kruskal-Wallis analysis of variance and Dunn-Bonferroni post-hoc’s pairwise comparisons
LOS = Limit of stability; EC = eyes closed; EC, foam = Eyes closed, standing over foam mattress; SA = Sway area; SV = Sway Velocity; CPTM = chronic perforation of tympanic membrane; CSOM = Chronic suppurative otitis media; Infected Cholesteatoma = Volunteers who had active or chronic suppuration and cholesteatoma, excluding patients with cholesteatoma but no active infection. The cells marked in gray and marked with a * refer to significantly worse results in a specific COM group as compared with the control group (P < 0.05).
Values of significance (P values) obtained from the comparisons of posturography test results in volunteers with COM and controls, as the result of Dunn-Bonferroni post-hoc’s pairwise comparisons
LOS = Limit of stability; EC = eyes closed; EC, foam = Eyes closed, standing over foam mattress; SA = Sway area; SV = Sway Velocity; CPTM = chronic perforation of tympanic membrane; CSOM = Chronic suppurative otitis media; Cholesteatoma = presence of cholesteatoma, with or without active middle ear inflammation. The cells marked in gray and marked with a * refer to statistically significant difference in the results (P < 0.05).

Boxplot graphics showing comparative analysis of posturography results (sway area, cm2; sway velocity, cm/s) under different stimuli. Legend: Eyes closed, foam = Patient stands on a foam mattress with eyes closed; Saccadic = patient stands on a firm platform with saccadic stimuli; Optokinetic = patient stands on a firm platform while subjected to optokinetic stimuli; and Visual-vestibular = patient stands on a firm platform, while subjected to visual (optokinetic) and vestibular (head rotation) stimuli. *=statistically significant difference as compared with the control group.
Among COM groups, we found a significant negative moderate correlation between the SVV results and LOS (correlation coefficient [CC], –0.350; 95% CI, –0.150 ––0.541; P = 0.001), and a significant weak positive correlation between SVV and sway velocity in the tests using a foam mattress (CC, 0.210; 95% CI, 0.007–0.395; P = 0.049) and with the eyes closed (CC, 0.241; 95% CI, 0.027–0.447; P = 0.023). In patients who complained of vestibular symptoms, the sway velocity and sway area in most posturography tests (except the test using a foam-mattress) were significantly worse as compared with patients without vestibular symptoms (P < 0.05). We did not find significant correlations between posturography results and laterality (unilateral or bilateral COM), abnormalities in the clinical vestibular tests, or the presence of tinnitus (P > 0.05).
Comparative analysis between posturography results and type of hearing loss showed that patients with mixed hearing loss had significantly worse sway area (eyes open, eyes closed, saccadic, optokinetic and visual-vestibular integration) and sway velocity (eyes open, eyes closed, saccadic and visual-vestibular integration) in several tests as compared with patients with conductive hearing loss (P < 0.05). In addition, we found a significant weak-to-moderate negative correlation between PTA and LOS in patients with COM (CC, –0.225; 95% CI, –0.018 ––0.405; P = 0.027), and correlation was more powerful when including only CSOM and cholesteatoma groups (CC, –0.352; 95% CI, –0.103 ––0.568; P = 0.009). We did not find significant correlations between PTA and remaining posturography parameters (P > 0.05).
Results of the video-HIT test showed no significant differences in the VOR gain or symmetry between COM (total and subgroups) and control groups (P > 0.05). We found abnormal results in 9 of 98 (9.1%) tests in the COM groups (2, unilateral; 7, bilateral). The abnormalities were more frequent in the CSOM group (CPTM, 4.5%; CSOM, 23%; cholesteatoma, 7%; P > 0.05). The canals which yielded abnormal results were the posterior in 4 patients and the lateral in 5. The saccades observed in the lateral canals were classified as covert saccades in 4 and overt in 2 –both volunteers with overt saccades had those seen in the clinical HIT test. None of the volunteers from the control group had abnormal video-HIT results.
There has been some debate in the literature on whether or not COM leads to vestibular problems [13, 45]. Recently, studies in human temporal bones have demonstrated a significant decrease in the number of vestibular hair cells, especially in the saccule and utricle, in bones with COM [13, 35]. Clinically, sparse studies in this regard demonstrated a variety of abnormalities in several vestibular function tests; [20] however, a recent systematic review has identified several potential biases in those studies, especially concerning inclusion/exclusion criteria and lack of control for confounding variables [34]. Therefore, to the best of our knowledge, ours is the largest study dedicated, based on a systematic research protocol, to evaluate the prevalence of vestibular symptoms and postural control in patients with COM, potentially providing the best available evidence in this regard.
We found a high prevalence of vestibular symptoms among patients with COM (58.4%), which is consistent with previous reports –estimated prevalence ranged from 40–60% among studies [34]. In our COM subgroups, the presence of vestibular symptoms was significantly higher in the CSOM and cholesteatoma groups as compared with the CPTM groups. In addition, the most frequent trigger to those vestibular symptoms was the onset or worsening of ear suppuration. Therefore, those findings suggest that the frequency and severity of the middle ear inflammation/infection may associate with the development of vestibular symptoms. Histopathologic studies provide grounds to our hypothesis: it has been demonstrated that the degree of middle ear inflammation and tissue abnormalities associate positively with the severity of damage affecting the sensorial epithelium of the cochlea and vestibule [24, 35].
Among our patients with COM, the prevalence of hearing problems (92.8%) was higher than the prevalence of vestibular symptoms (58.7%). In this regard, it has been observed that the auditory sequela of COM seems to precede and be more severe than vestibular symptoms [9, 35]. It is also possible that a potential chronic, slow progression of vestibular or balance issues secondary to COM may allow adequate central compensation over time –in such case, vestibular symptoms would mostly occur in the events of challenging situations or acute or severe episodes of middle ear inflammation [9, 34].
The results of audiometry tests revealed that, among our patients with COM, 52.1% had mixed-type hearing loss, which, in turn, associated with worse PTA and speech discrimination scores as compared with conductive hearing loss (P < 0.05). Those results are consistent with extensive literature showing similar findings [11, 38]. In our study, some observations seemed to suggest a correlation between the presence of mixed-type hearing loss with postural balance problems and presence of vestibular symptoms: (1) among patients with mixed hearing loss, posturography results (LOS, sway velocity and sway area) were significantly worse as compared with patients with conductive hearing loss (P < 0.05); and (2) the presence of tinnitus, which has been associated with more intense degrees of cochlear hair cell loss and distal afferent dendrite degeneration [3, 48], was more frequent among patients with mixed hearing loss, and associated with a two-fold increase in the risk of patients suffering from vestibular symptoms (P < 0.05). To our knowledge, only one histopathologic study demonstrated such combined degeneration of the sensorial epithelium of the cochlea and vestibular structures secondary to COM [35].
Clinical vestibular function tests showed a significantly higher prevalence of abnormalities in patients with COM (63%) as compared with controls (2%), and those correlated positively with the presence of vestibular symptoms (P = 0.002). The abnormalities occurred mostly in tests directly or indirectly associated with the function of otolithic organs and vestibulospinal reflex (Fukuda, SVV, Romberg) [8, 39]. Although the role of the Fukuda and Romberg tests in the diagnosis of vestibular disfunction has been described in the past [16, 43], further studies analyzing their sensitivity and reliability have disputed those assumptions, especially in chronic, compensated vestibular disorders [7, 22]. The SVV test, on the other hand, is a validated and reliable way to assess otolithic function [51]. Although it may also suffer influences of higher vestibular structures and somatosensorial input, those do not seem to significantly influence their results [36]. Although several articles demonstrated that the SVV frequently yields abnormal results in diseases affecting the peripheral vestibular system in isolation [10], the role of the SVV in diagnosing chronic, compensated vestibular disorders has not been extensively studied yet. Assuming that the SVV somewhat reflects function of otolithic organs, our finding showing a significant negative correlation between the SVV and LOS may suggest that those balance problems may be at least partially attributable to otolithic dysfunction.
The results of posturography testing revealed worse limit of stability in all COM groups as compared with controls (P < 0.05). In groups with active disease (CSOM and COM with active middle ear inflammation), the sway area and sway velocity in the majority of the posturography tests using different stimuli were also significantly worse as compared with controls. Furthermore, we observed that –among patients with COM and vestibular symptoms –the LOS was significantly increased as compared with patients with COM who did not have vestibular symptoms. Although those findings point toward worse postural control and potential vestibular impairment, posturography results should be interpreted with caution, considering that it assesses “balance” rather than peripheral or central vestibular function [17]. Nonetheless, it has been demonstrated that some of its tests (particularly tests which deprive patient from visual and somatosensorial information) may grossly correlate with vestibular (mostly otolithic) function [27]. Considering those limitations, we observed that the most challenging test for patients with COM was the foam-mattress test with eyes closed (which deprives the patients from visual reference and proprioception), suggesting that some of those abnormalities could have occurred due to vestibular dysfunction [15, 27]. Although speculative, the observation of worse posturography results among groups with more severe middle ear inflammation (CSOM and cholesteatoma) may suggest that COM may play a role in the development of those symptoms [9, 46].
A noteworthy fact is that –although vestibular symptoms and worse balance control generally associated with the presence of more intense hearing problems –the progression of hearing problems seemed to occur regardless of the presence of vestibular/balance issues. Those findings may associate with previous observations that hearing sequela of COM is more frequent and more severe than vestibular sequela [9, 13]. In this regard, it has also been demonstrated that hearing loss in isolation may lead to worse postural control as compared with controls, which could have been a confounding factor in our study [23, 49]. Although our methodology and tests may not allow adequate control for such variable, some findings from our and other studies suggest that hearing loss may not be the only factor playing a role in the development of postural balance problems: (1) among patients with COM, the presence of sensorineural hearing loss which was more frequent in significantly associated with worse LOS as compared with patients with pure conductive hearing loss; and (2) histopathologic studies have demonstrated a significant positive correlation between the severity of loss of cochlear hair cells with loss of vestibular hair cells of temporal bones with COM, suggesting that the inner ear damage secondary to COM may affect the neuroepithelium of both the cochlea and vestibule [13, 35]. Thus, is possible that the presence of inner ear damage secondary to COM may also contribute with the development of postural instability in patients with COM.
We found no significant differences in the results of the video-HIT between the COM and control groups. We hypothesized 3 possible explanations for those findings: (1) the sensitivity of video-HIT may not allow accurate detection of chronic, compensated abnormalities affecting the semicircular canals, [31]; (2) because VHIT measures the VOR at high frequency, it is possible that abnormalities affecting the semicircular canal function in the lower, and more physiologic, frequencies could have been missed [42]; and (3) semicircular canals may be less affected by the inflammatory damages caused by COM than the otolithic organs [35]. The latter hypothesis is further supported by Chang et al. [9], who demonstrated that, in COM, vestibular deficits are more significant in the otolithic organs, while semicircular canal dysfunction occurs only in later stages.
Our findings bear important clinical implications. The clinical vestibular tests and posturography findings suggest that patients with COM (especially elderly) may be at an increased risk of disequilibrium and falls, which is a major cause of morbidity and mortality [35, 50]. Considering that COM is one of the leading causes of hearing impairment [25, 33], postural balance problems may constitute an additional burden to patients with COM.
Our study has some limitations. First, the strictness of our exclusion criteria (which is one of the main strengths of our study) has reduced drastically the number of potential volunteers. The use of some relevant tests for analyzing vestibular function (such as caloric tests and VEMPs) was not possible due to the negative influence of hearing loss and middle-ear conduction deficits in their results. In addition, although the selected vestibular function tests (video-HIT and posturography) are not influenced by those factors, they have other inherent limitations in evaluating vestibular function: posturography testing results do not directly correlate with vestibular function [17], and video-HIT test seems to have limitations to assess VOR abnormalities in chronic, compensated vestibular disorders [31]. It is possible that –in the future –other vestibular function tests (such as rotational chair testing, videooculography, dynamic posturography test, and dynamic SVV during centrifugation in the rotatory chair) may be used to further assess vestibular function among patients with COM.
Conclusion
Our study demonstrates that COM associates with significantly higher prevalence of vestibular symptoms, abnormalities in clinical vestibular function tests, and worse postural control in the static posturography as compared with controls. Patients in COM groups with signs of active middle ear inflammation (CSOM and cholesteatoma with active middle ear inflammation) seemed to be more symptomatic and have worse postural control than patients in the group with less frequent suppuration (CPTM).
Funding sources
Three authors (RCM, ALPK, TGAE) received a scholarship from the the “Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES)” (Finance Code 001).
Conflicts of interest
None to declare.
Footnotes
Acknowledgments
We thank Flavia Salvaterra Cusin for the great technical support; Grace Sinae Park for critically reviewing the manuscript; and the “Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES)” (Finance Code 001) for partially financing this study.