
Abstract
BACKGROUND:
Investigations measuring gait tests have rarely been studied in the benign paroxysmal positional vertigo (BPPV) population.
OBJECTIVE:
Examine instrumented mobility metrics in people with posterior semicircular canal BPPV. We examined the impact of a canalith repositioning procedure (CRP), prior to and after treatment on instrumented mobility measures, comparing the scores to those of healthy controls.
METHODS:
At baseline, the subject performed a series of instrumented gait and balance tests and then, the CRP was performed. At re-evaluation (1-week later), identical gait and balance tests were assessed. In addition, the Hallpike-Dix test identified patients who had improved or had not improved in their BPPV signs and symptoms.
RESULTS:
Thirty-two people with BPPV (25 women) and 15 healthy subjects participated in the study. At baseline (pre-CRP), people with BPPV demonstrated an increased vestibular ratio, and walked more slowly compared with the healthy controls. The CRP resolved the vertigo in 90.6% of the BPPV subjects. Compared with the pre-CRP scores, the BPPV subjects demonstrated a decreased vestibular ratio and faster walking at the post-CRP evaluation. Out of the five parameters that were significantly different from the healthy values pre-CRP, only one remained different post-CRP.
CONCLUSIONS:
Besides vertigo and balance difficulties, people with BPPV demonstrate walking modifications. Furthermore, the CRP has a high success rate in improving not only vertigo but also in restoring gait and balance in persons with BPPV.
Introduction
Benign paroxysmal positional vertigo (BPPV) is considered to be the most common peripheral vestibular disorder with an estimated incidence of 107/100,000 per year and a lifetime prevalence of 2.4% [16, 34]. BPPV most frequently affects the posterior semicircular canal accounting for 80–95% of cases; horizontal semicircular canal BPPV accounts for 5–30% of cases and the remainder comprise anterior and multiple semicircular canal BPPV [3].
BPPV is recognized as a disease of the elderly with females affected twice as often [26]. The 1-year prevalence of individuals with BPPV attacks rises steeply with age, from 0.5% in people aged 18 to 39 to 3.4% in those aged 60 and older, and the lifetime incidence of BPPV reaches almost 10% by the age of 80 [27, 34]. At present, the mechanisms of BPPV may be explained by canalolithiasis and cupulolithiasis. However, the underlying causes that lead to detachment of otoconia from the utricle are still poorly understood in the vast majority of patients [26]. A diagnosis of BPPV of the posterior semicircular canal is confirmed by the Dix-Hallpike test and is classified as objective when nystagmus is observed during the test or subjective when vertigo occurs without nystagmus [19]. The standard treatment for BPPV is the canalith repositioning procedure (CRP), which is designed to move the otoconia from the involved semicircular canal into the utricle, resulting in the resolution of symptoms. Other treatments for BPPV include Brandt-Daroff exercises [8], and medications, e.g, anti-vertiginous, anti-anxiety, and anti-emetic drugs [21].
Poor postural control is well established in people with BPPV [1, 23]. This symptom has been confirmed by studies demonstrating a significant increase in body sway in both the lateral and anteroposterior planes during static balance tests under eyes open and eyes closed test conditions [17]. Furthermore, increased postural sway while standing under conditions with altered proprioceptive feedback and/or reduced visual input was also found in people with BPPV [1]. Surprisingly, standard mobility and/or gait tests rarely have been studied in the BPPV population. Recently, Sim et al. (2019) published a systematic review and meta-analysis on evaluation measures following CRP maneuvers in adults with BPPV [33]. Remarkably, only three studies (out of 35) included a walking metric as an outcome measure [24, 31]. Two were examined only for a short walking distance (10m) while the other subject based a walking assessment on a single question. Celebisoy (2009) examined walking speed in adults with BPPV, however it was measured during a short tandem walking test, which is a test of dynamic balance [10].
According to our literature search, no study has of yet, examined gait over longer distances and/or collected spatiotemporal parameters of gait in people with BPPV. Furthermore, functional mobility tests such as the Timed-Up and Go (TUG) has never been tested in people with BPPV, which is regrettable. BPPV is a risk factor for falls [22], and the TUG test and spatiotemporal measures of gait, might be helpful as they may serve as predictors for an increased risk of falls, fractures and other fall-related injuries.
Therefore, the primary aim of the present study was to examine instrumented mobility metrics in people with posterior semicircular canal BPPV. Furthermore, we examined the impact of CRP on instrumented mobility measures and compared the scores of persons with BPPV to those of healthy controls.
Materials and methods
Study design and participants
This clinical prospective research study was performed at the Department of Physical Therapy, Maccabi Healthcare Services, Rishon LeZion, Israel, between June 2017 and December 2018. Thirty-two people with BPPV (25 women, 7 men), mean age 64.0 (S.D. = 6.4), volunteered to participate in the study. The participants learned of this study through e-mails and printed advertisements posted in the department. The study team’s contact details were provided, which enabled those interested to further enquire and participate in the study. Interested participants were provided with an information packet describing the study, supported by verbal information when requested. BPPV participants were screened for eligibility by the principal investigator, who obtained written informed consent from those who met the criteria. Only one patient who visited the service refused to participate in the study.
Inclusion criteria were: (1) a diagnosis of BPPV involving the posterior semicircular canal confirmed by the presence of positional vertigo and a typical torsional up-beating nystagmus provoked by the Dix-Hallpike test [13]; (2) the subject had undergone a clinical examination detailing their medical history and an oculomotor examination confirming the diagnosis; and (3) age range from 50–75 years, representing the common age of BPPV onset [4]. A decline in walking speed is evident after 70 years of age. Therefore, in order to increase the homogeneity of the group, the age range for eligibility was reduced compared to previous studies. Exclusion criteria were: (1) patients with BPPV involving the anterior and/or horizontal canal; (2) other vestibular disorders including Meniere’s disease, vestibular neuritis, labrinthitis and peripheral vestibular loss; and (3) proprioceptive impairment, cardiovascular disease or orthopedic disorders that could negatively affect mobility. Fifteen apparently healthy subjects (9 women and 6 men), mean age 63.5 (S.D. = 7.1), served as controls. Approval was obtained from the Maccabi Healthcare Medical Independent Ethics Committee prior to commencement of the study (ASMC-17-0007).
Experimental design
People with BPPV were assessed at two separate sessions. At baseline, following eligibility determined by YN and within two-weeks of onset of vertigo complaints, the subject performed a series of instrumented gait and balance tests. Immediately after these tests a CRP was performed on the patient by a physical therapist with ten years of experience in vestibular rehabilitation. The patient was subsequently sent home and rescheduled for a return visit one week later for re-evaluation. Gait and balance tests, identical to those performed at baseline, were performed at the second session by the same tester as the tester who performed the gait and balance tests at baseline. At the second session, the Dix-Hallpike test without visual fixation suppression was used to differentiate patients who had improved in their BPPV signs and symptoms from those who had not improved. These patients were referred to as having had a successful CRP outcome or an unsuccessful CRP outcome, respectively. Healthy controls performed all gait and balance tests at a single session.
Canalith repositioning procedure
The canalith repositioning procedure (CRP) is a specific treatment for patients with posterior semicircular canal benign paroxysmal positional vertigo based on the canalithiasis theory [15]. In our study, all subjects received the CRP as described by Epley not including vibrations of the mastoid process or use of valium in a single session [15]. Prior to treatment, it was explained to the subjects that the treatment might provoke vertigo and nausea.
The CRP was performed as follows: the patient was placed in an upright position with the head turned at a 45° angle toward the affected ear; the patient was then rapidly placed in a supine head-hanging position, which was maintained for 60 seconds. Next, the head was turned at a 90° angle toward the other (unaffected) side and held for approximately 60 seconds. Following this rotation, the head was subsequently turned a further 90° such that the patient’s head was nearly in a facedown position. This position was also held for 60 seconds. The patient was then brought into an upright sitting position, thus, completing the maneuver. Three cycles of the CRP were performed during the session.
Gait and balance outcome measures
Instrumented gait and balance measurements were recorded by the APDM Mobility Lab System (v2) (Opal sensors, APDM, Portland, OR, USA). Instructions and sensor placement were executed according to the APDM Mobility Lab User Guide. During the tests, three wireless inertial sensors secured by elastic straps for the duration of the testing were positioned on each participant. The lumbar sensor was mounted on the lower back over the posterior surface, at the L5 level. Foot sensors were mounted on the dorsum surface of each foot. The reliability and validity of the Mobility Lab System has been established in various populations including patients with vestibular disorders [32]. All tests were performed by a certified physical therapist.
Outcome measures included the: Instrumented 2-minute walk test (i2MWT) assessed by walking straight down a 30 m long well-lit corridor. The participant was instructed to walk for 2 minutes according to the following instructions: “Cover as much ground as possible in 2 minutes. Walk nonstop if possible, but do not be concerned if you need to slow down or stop to rest. The goal is to feel that at the end of the test, more ground could not have been covered in the 2 minutes”. Gait parameters collected and extracted by the device were velocity, cadence, stride length, double support phase, turn velocity and duration. Height, weight and leg length were measured for normalization. Instrumented Timed Up and Go test (iTUG) requires both static and dynamic balance. The starting point is determined when the subject has been seated in a chair with their back flush against the chair and their arms resting on the arm rests. He/she is then instructed by the examiner to stand up, walk 3 meters, turn around, walk back to the chair and sit down again. The participant was instructed to use a comfortable and safe walking speed. Timing begins when the individual begins to rise and ends when he/she returns to the chair and sits down. Parameters extracted by the mobility lab were total duration, turn duration and turn velocity. The test was performed twice; the first attempt was designated as a practice trial. Static balance - Each subject completed a sequence of four consecutive tests under four different task conditions with a 1-minute break between tasks. Each task was repeated twice, each task for 30 s, with a rest interval period of 30 s. Eyes open/Firm surface - Subjects stood barefoot on the ground (a 10 cm gap between heels; 5° toe-out position) and were instructed to maintain their posture as steady as possible. Eyes closed/Firm surface - Identical conditions as (a) but with eyes closed. Eyes open/Foam surface - Identical conditions as (a) but subjects stood on a foam surface. Eyes closed/Foam surface - Identical conditions as (c) but with eyes closed.
For tasks c,d requiring a foam surface, a 40.6×40.6×7.6 cm piece of medium density viscoelastic foam was used. For each task, the center of pressure (CoP) path length (mm) was recorded. Based on the CoP path length, we performed a sensory ratio analysis that yielded three different ratios: somatosensory (= task b/task a), visual (= task c/task a), and vestibular (= task d/task a). The sensory ratio analysis was based on the sensory organization test, which indicates the contribution of the visual, vestibular and proprioceptive systems to postural control [37].
Statistical analysis
Data analysis was performed using the IBM SPSS statistics software (version 25.0 for Windows, SPSS Inc. NY, USA). Data were initially examined for normality violations, outliers, errors and missing values. A p-value in each case of <0.05 was considered significant.
We focused on three different comparisons: People with BPPV at baseline (pre-CRP) vs. healthy controls, using the t-test for independent samples and continuous variables and the chi-square test for categorical data; Pre-CRP vs. post-CRP using the paired sample t-test. The effect of the CRP on gait and balance performance was examined only in those patients who demonstrated improvement in BBPV signs and symptoms according to the Hallpike-Dix test; Post-CRP versus healthy controls, using the t-test for independent samples. This analysis was computed in order to clarify whether balance and gait performance of the BPPV participants who demonstrated improvement in BBPV signs and symptoms returned to normal after the CRP intervention. As for the sample size calculation, according to the literature, a 0.1 m/s change in walking speed demonstrates a clinically meaningful difference. We set the power at 80% and the alpha at 5%. Using a relatively conservative estimate, 32 subjects were required in order to detect differences between pre-post CRP treatment.
Results
Demographic and clinical data of the 32 people with BPPV and the 15 healthy subjects enrolled in the study are presented in Table 1. No significant differences were observed between the groups in terms of age, gender distribution, height, weight and BMI. Table 2 presents the instrumented gait and balance scores of the BPPV group pre-CRP (n = 32) and the healthy controls. People with BPPV demonstrated an elevated (∼34%) CoP path length (mm) in the eyes closed/foam surface condition, compared with the healthy participants. Similarly, the vestibular ratio was significantly elevated in the BPPV group compared with the healthy subjects. Furthermore, the BPPV participants walked more slowly with shorter strides, compared with the healthy group.
Demographics and clinical characteristics of the study group
Demographics and clinical characteristics of the study group
Mobility and static balance outcome measures in BPPV and healthy control groups
*P-value <0.005. CoP, Center of Pressure; iTUG, Instrumented Timed Up & Go; i2MWT, Instrumented 2-minute Walk Test.
Comparison of gait and balance parameters between pre-CRP and post-CRP scores were examined solely in BPPV patients who had experienced a successful CRP treatment, specifically, the elimination of vertigo signs and symptoms. Classification of a successful or unsuccessful CRP intervention was based on the Dix-Hallpike test. The CRP resolved the vertigo in 90.6% (29 out of 32) of the BPPV subjects (= successful CRP). Three subjects remained with signs and symptoms of vertigo (= unsuccessful CRP). No statistical analysis was performed on the unsuccessful CRP group due to the low number of participants (n = 3).
Table 3 presents the instrumented mobility and postural control scores, pre-post successful CRP (n = 29). Compared with pre-CRP scores, the BPPV subjects demonstrated a reduction in the CoP path length in the eyes closed/foam surface test condition and in the vestibular ratio at the post-CRP evaluation. No differences between pre-CRP vs. post-CRP were found for the CoP path length in the other three conditions, the somatosensory ratio and visual ratio. As for mobility measures, people walked significantly faster, including while turning, at the post-CRP session compared with pre-CRP. Instrumented mobility scores of the BPPV subjects at post-CRP were compared with the healthy controls. Out of the five parameters that were significantly different pre-CRP (CoP path length with eyes closed/foam surface, vestibular ratio, walking speed, stride length, and iTUG total duration), only stride length remained different (shorter) post-CRP. Figure 1 illustrates the main balance and mobility outcome measures of the healthy controls and BPPV participants at baseline and post intervention.
Mobility and static balance outcome measures pre-post in BPPV subjects (n = 29) following a successful canallith reposition procedure
*P-value <0.005. CoP, Center of Pressure; iTUG, Instrumented Timed Up & Go; i2MWT, Instrumented 2-minute Walk Test.
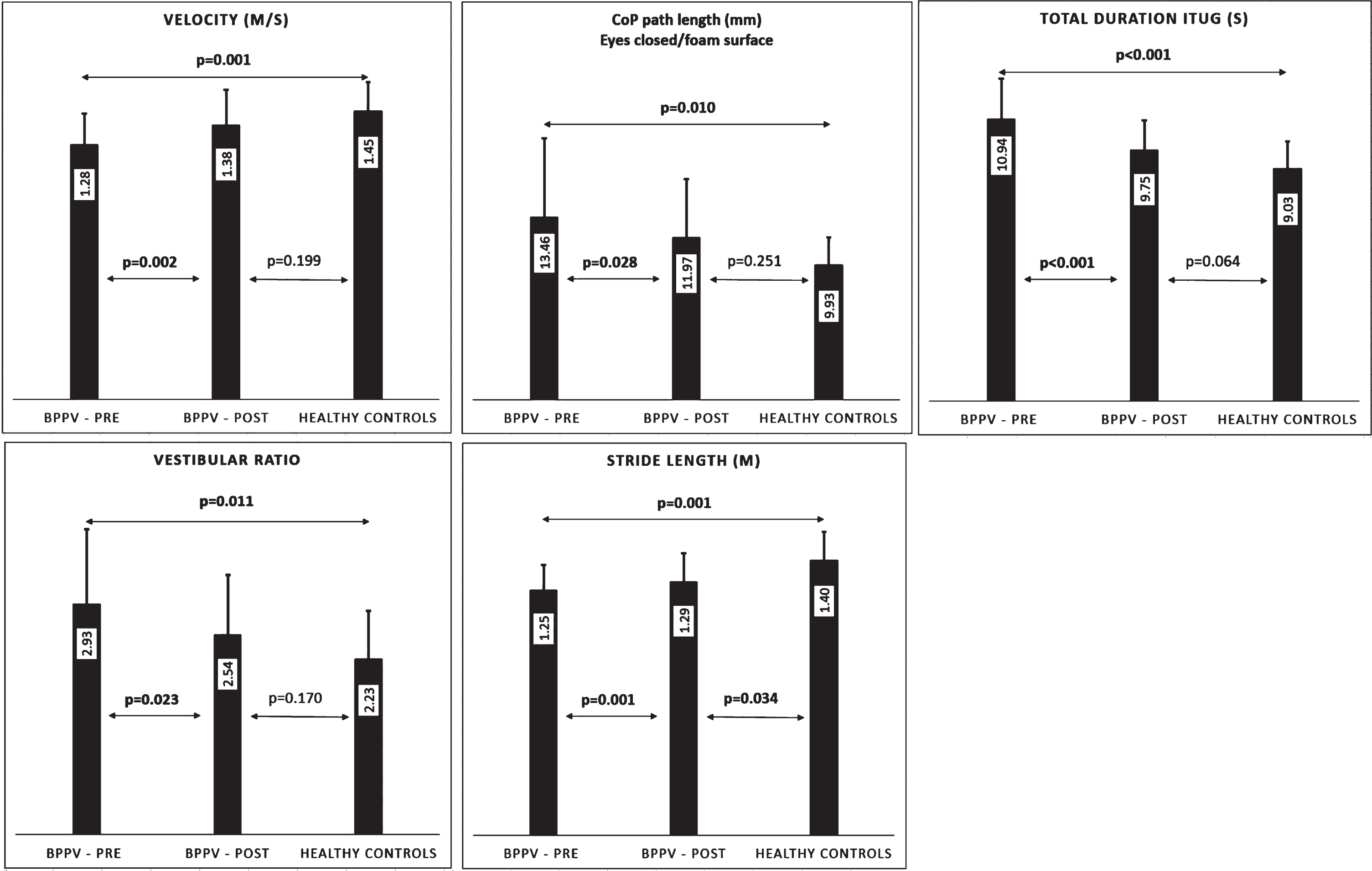
Balance and mobility outcome measures of the healthy controls and BPPV participants at baseline and post intervention.
People with BPPV walk more slowly compared to healthy adults. This finding was demonstrated on a relatively long walking course and the iTUG functional mobility test. Additionally, people with BPPV have poor postural control compared with healthy adults, when balance mainly depended on the vestibular system. In those individuals with a successful CRP outcome, most of the gait and balance scores observed at baseline (pre-CRP) improved post-CRP into values that were similar to the scores of the healthy participants.
The CRP is considered the gold standard for treating BPPV [5]. Its efficacy has been well established in the literature [9, 35]. However, it is worth noting that the efficacy of the CRP has been mostly confirmed by positional tests and subjective dizziness/vertigo reports. Our findings resemble those of Celebisoy [10] who found an increase in walking speed following CRP treatment in 32 people with posterior canal BPPV. However, the walking speed was measured during a 1.5 m tandem walking test and therefore reflects an improvement in dynamic balance and not necessarily in normal walking speed [10].
Our novel contribution to the literature is we found walking speed recovered after t CRP treatment. Patients increased their walking speed by approximately 8% on the long walking test and 11% on the iTUG test post-CRP. Importantly, the change in gait speed of the patients post-CRP was in the range of minimal clinically important difference values for adults with different pathologies (0.08–0.26 m/s) [7]. Interestingly, although stride length increased following CRP treatment it remained significantly shorter compared to that of healthy controls. This finding might be related to patients adopting a more cautious gait pattern [18] in order to increase steadiness and reduce risk of falls.
According to Whitney et al. [36], people with vestibular disorders who score >11.1 seconds on the TUG are five times more likely to report falling during the previous 6-months. Based on this statistic, 40% of the BPPV participants in our cohort performed the iTUG slower (>11.1 s) at the pre-CRP evaluation, whereas, only 14% walked slowly at the post-CRP evaluation, implying that 26% shifted from a high risk of falling to a low risk. This finding is important for health professionals treating people with BPPV. It might be useful to follow up on testing the TUG mobility marker. The iTUG data can help determine which of these individuals are at risk of falling during the period after the CRP treatment. This advice is reinforced by the fact that recurrence appears in 36% of BPPV cases [2]. Balance vestibular rehabilitation therapy, in addition to CRM, might be useful as it has been shown to improve dynamic balance in elderly people with BPPV [30].
An additional contribution of this study relates to the evaluation of the postural control ratios. Only a few studies have included postural control ratios when evaluating people with BPPV [12, 28]. From this perspective, our findings strengthen the results of Di Girolamo et al. [12] who examined a group of 32 people with BPPV, before and after recovery. The authors clearly showed that in BPPV patients there is an impairment in postural control according to the vestibular ratio, which improves after the Semont maneuver. Unfortunately, their study did not compare the BPPV group’s results with their normative values. Our study confirms that not only did the vestibular ratio decrease (indicating improvement) following the CRP, but returned to the similar values of the healthy age-matched controls. Therefore, we encourage vestibular rehabilitation professionals to include postural control ratios in their evaluation programs, as these metrics seem more precise compared with traditional posturographic measures (e.g. sway rate, CoP trajectories) for the BPPV population.
This study is not without limitations. Firstly, there was no waiting list, alternative, or sham treatment versus the CRP. This decision was taken following several ethical restrictions. Due to the severity of the BPPV symptoms, it seemed unreasonable to postpone treatment or provide a sham alternative. Secondly, the sample size was relatively small. Therefore, it was impossible to provide significant information for the BPPV subjects who did not respond well to the CRP treatment (n = 3). Additionally, although the Dix-Hallpike is a specific and sensitive test, some may argue a possible bias since it was performed pre- and post-CRP intervention by the same tester. It is worth noting Cohen et al. (2014) reported when tested a few days apart, the Dix- Hallpike test had similar response frequencies and test outcomes, indicating its reliability [11]. Therefore, we consider the absence of a blinded tester as a minor limitation. Furthermore, we did not include measures of mental health (i.e. anxiety, mood, personality disorders) and rate of falls, which is relatively high in BPPV. Finally, long-term measurements, beyond the short-term recovery, were not included, as this was not the focus of the study.
Conclusions
This study found that besides vertigo and balance difficulties, people with BPPV demonstrate walking modifications. Furthermore, the CRP has a high success rate in improving not only vertigo but also in restoring gait and balance. We advise clinicians to follow vestibular ratio parameters, as these seem highly related to changes occurring during the course of BPPV. Moreover, due to its close relationship with the risk of falling, clinicians should also consider including the TUG as part of the follow-up examination. Nevertheless, additional research is still needed to explore the interactions among balance, gait, and the CRP in the long term in order to optimize treatment for persons with BPPV.
Funding source
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors