
Abstract
BACKGROUND:
While patients with benign paroxysmal positional vertigo (BPPV) commonly develop residual dizziness (RD) after successful repositioning, the factors predictive of RD remain controversial.
OBJECTIVE:
To identify factors predictive of RD onset in patients with BPPV following successful repositioning.
METHODS:
This multi-center prospective cohort study enrolled 243 patients with idiopathic BPPV. Vestibular functional and psychological wellbeing assessments administered before repositioning provided the data used to identify factors predictive of RD with a log-binomial model. The endpoint was RD at 1 week after successful repositioning.
RESULTS:
Of the enrolled patients, 118 reported RD. After adjusting for cofounders, mild [risk ratio (RR), 2.06; 95% confidence interval (CI), 1.39–3.04] or severe (RR, 3.08; 95% CI, 2.17–4.38) anxiety and abnormal vestibular ratio of sensory organization test (RR, 2.68; 95% CI, 1.82–3.95) were identified as risk predictors. Presence of ocular vestibular evoked myogenic potentials responses, either unilateral (RR, 0.55; 95% CI, 0.44–0.69) or bilateral (RR, 0.49; 95% CI, 0.36–0.68), were protective factors.
CONCLUSIONS:
Anxiety and abnormal balance are significant predictors of RD, while the presence of ocular vestibular evoked myogenic potentials responses predicts against it. These findings may help to improve BPPV outcomes by informing prognoses and guiding treatment strategies.
Trial registration:
ChiCTR1800018004 (date of registration: 26 August 2018)
Introduction
The most common type of vertigo, benign paroxysmal positional vertigo (BPPV) has a lifetime prevalence of 3.2% among women, 1.6% among men, and an overall prevalence of 2.4% in the general adult population that increases with age [20, 33]. Although two theories, cupulolithiasis and canalithiasis [8, 25], have been proposed to explain the pathophysiology of BPPV, they may coexist simultaneously, and the latter has garnered wider acceptance as it provides a better account of the symptoms induced by BBPV [4]. According to the canalithiasis hypothesis, BPPV is caused by the mechanical stimulation of vestibular receptors within the semicircular canals (SCCs) by free otoconia dislodged from the utricular macula, which then provoke episodic vertigo attacks. Although BPPV could theoretically occur in any of the three SCCs, the posterior semicircular canal (PSC) is most commonly affected, followed by the horizontal canal (HSC). BPPV treatment involves the canalith repositioning procedure (CRP), which clears dislodged otoconia from the affected canals and immediately resolves vertigo in most cases [3, 8]. However, regardless of its success, CRP can result in periods of residual dizziness (RD), characterized by non-specific symptoms, including dizziness or imbalance, without positional vertigo [7, 26–29].
As the exact cause of RD remains controversial, it has variably been attributed to small remnants of otoconial debris in the semicircular canal, incomplete central nervous system adaptation, sympathetic nervous system dysfunction, mental stress, and otolith organ dysfunction [11, 29]. Several empirical studies have investigated risk factors for RD, including otolith organ dysfunction, as measured by cervical and ocular vestibular evoked myogenic potentials (cVEMP and oVEMP, respectively) [15, 26]; psychological factors, such as anxiety and depression [16, 17]; and demographic or clinical features [17, 27]. However, such studies have yielded inconsistent findings. For example, some studies found that advanced age was associated with a higher risk for RD [17, 31], while others found no link [26, 29].
This study sought to identify RD-predictive factors while addressing the sources of the aforementioned inconsistencies, including small sample sizes, retrospective designs, univariant statistical analysis, and heterogeneity of the study samples, through a well-powered prospective cohort study. Specifically, our investigation examined the relationship between RD and a comprehensive set of variables, including vestibular organ function variables assessed using oVEMP, cVEMP, caloric, and sensory organization tests (SOT) as well as psychological wellbeing variables of anxiety and depression.
Methods
Study design, setting, and patient population
This prospective, multi-center cohort study enrol-led patients diagnosed with PSC or HSC-BPPV from five ear, nose, and throat (ENT) clinics in Shanghai, China, from October 2018 to October 2019. Of the five participating clinics, the sponsoring site was an ENT-specialized hospital, while the other four were clinics within general hospitals. All centers were equipped with the same vestibular examination facilities purchased by the sponsoring site for the purpose of guaranteeing the homogeneity of the test results. Ethical approval was obtained from the institutional review boards of all five participating centers. Informed consent was obtained from all patients before their inclusion in the study. The study was performed in accordance with the Declaration of Helsinki and its later amendments.
We enrolled patients with unilateral idiopathic BPPV. A diagnosis of BPPV was rendered based on the American Academy of Otolaryngology-Head and Neck Surgery guidelines [3]. Briefly, the diagnosis of BPPV requires (i) patient report of vertigo provoked by changes in head position relative to gravity and (ii) a mixed torsional and upward beating nystagmus during the Dix-Hallpike position (for PSC-BPPV) or (iii) a direction-changing horizontal nystagmus beating towards the undermost ear with the head turned to either side during the supine roll test (for HSC-BPPV). The nystagmus presents with short latency, lasts for less than a minute and is characterized by an increase followed by a decrease in its intensity. Patients diagnosed with PSC-BPPV were treated with the Epley maneuver, while those with HSC-BPPV were treated with the Barbecue maneuver. Participants also had to meet the following inclusion criteria: age of 18–80 years, normal cognition, and the provision of consent to undergo the CRP and return for follow-up. Patients were excluded if they had bilateral or multi-canal or superior canal BPPV, considered as emerging and controversial syndromes by the Barany Society for the difficulty of being differentiated from central positional vertigo [32]; if they had a previous history of BPPV; if they are unable to tolerate CRP; if they had other inner ear diseases, such as Meniere’s disease, vestibular migraine, hearing loss (pure tone audiometry≥40 dB), ear surgery history; if they had vertigo caused by brain trauma or vertebrobasilar artery stenosis or of central origin; if they had mental illness such as dementia and schizophrenia confirmed by a psychiatric physician; or they were recipients of medication in the past three months that might have caused dizziness. All eligible patients underwent vestibular testing and psychological examinations (as described in the exposure variable evaluations) before repositioning maneuver was performed. After execution of the CRP maneuver, the patient was reassessed with the Dix–Hallpike test or supine roll test, in cases nystagmus was still present, the Epley or Barbecue maneuver was repeated up to a maximum of three times. We defined the treatment success as absence of nystagmus and positional vertigo.
Exposure variable evaluations
Caloric test
All participants underwent a bithermal caloric test in a supine position. Each ear was irrigated with a 60-second constant flow of air (8 L/min) produced by a GN Otometrics Type Air Irrigator (Otometrics, Taastrup, Denmark). The air temperatures were 49°C and 23°C. Jongkees’ formula was used to detect canal paresis (CP). A CP percentage of >22% was considered an abnormal response, and the normal upper limit of directional preponderance (DP) was 30%. These values were predefined across all study sites.
Sensory organization test
As a metric for the patients’ abilities to employ visual, vestibular, and somatosensory system inputs to maintain balance under different conditions [19], postural performance was examined using the SOT on the Equitest platform (NeuroCom International Inc., Clackamas, Oregon, USA). Six increasingly challenging conditions (from SOT1 to SOT6) were introduced to disrupt balance sensory input or perception of visual surroundings. Three trials were administered for each condition. We calculated the somatosensory (SOM), visual (VIS), and vestibular (VEST) ratios by dividing the scores in conditions 2, 4, or 5 by the score in condition 1, respectively [19]. Normative data are embedded in the system software. The SOM, VIS, and VEST ratios are defined as normal or abnormal according to the cutoffs of the age-specific normative values situated at 1.67 standard deviations below the respective means [19]. Figure 1 provides a SOT report template.
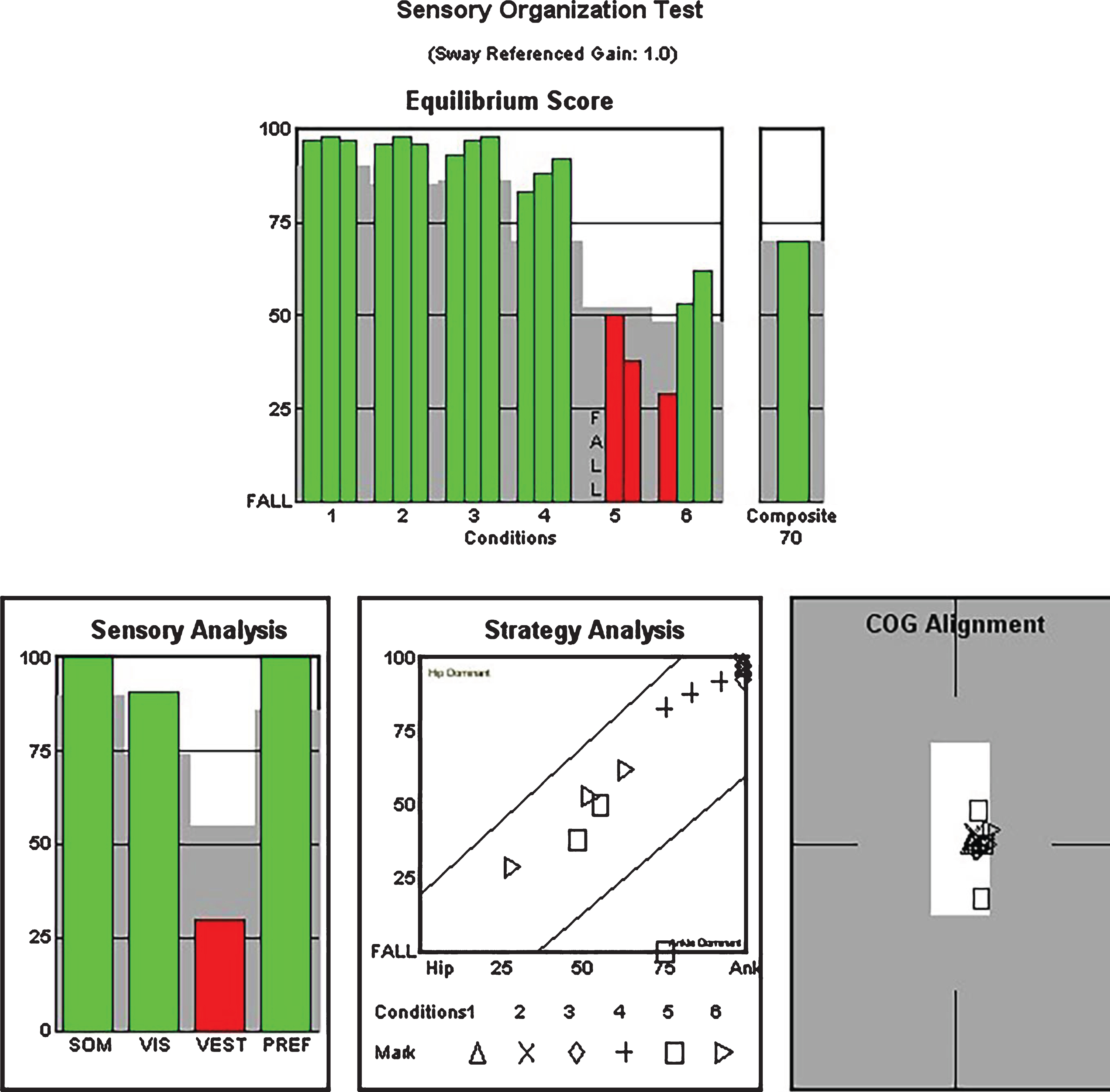
Sensory organization test report sample. The abnormal VEST ratio is presented in red. SOM, somatosensory; VIS, visual; VEST, vestibular.
We recorded oVEMP and cVEMP with a Bio-Logic Navigator Pro auditory brainstem response diagnosis system (Natus Medical Inc., Pleasanton, CA, USA) in a soundproof room. The detailed methods for conducting the VEMPs test have been reported previously [5]. Briefly, air-conducted sound with a 500 Hz short-tone burst was transmitted via inserted headphones. The stimulus intensity started at 95 dB nHL (decibels above normal adult hearing level) and was then decreased by intervals of 5 dB nHL until the VEMP response was no longer elicited. For the cVEMP test, participants situated themselves in a sitting position and rotated their heads away from the stimulated side when a given stimulus was heard. The electromyographic activity in the tonically activated sternocleidomastoid (SCM) muscles was recorded. The cVEMP was defined as the first positive–negative–positive peak (P1–N1–P2). For the oVEMP test, subjects were instructed to lift their heads when they heard a stimulus. The oVEMP was defined as the peak of the first negative and positive biphasic waves (N1–P1). Both VEMP tests were repeated thrice for each patient to ensure the reliability and reproducibility of the results. The absence of a c/oVEMP was defined as the absence or irreproducibility of a meaningful waveform.
Anxiety or depression
The presence of perceived anxiety or depression was evaluated with the Hospital Anxiety and Depression Scale (HADS, Chinese version), which comprises 14 questions evenly divided into anxiety and depression subscales. Each item on the subscale is scored between 0 and 3. The sum of all scores on either subscale yields a subscale score of between 0 and 21. A score of ≤7 indicates no anxiety or depression; 8–10, moderate anxiety or depression; and ≥11, severe anxiety or depression [38].
Outcome variable
The outcome variable of interest was the post-CRP occurrence of RD. The presence of RD was evaluated at a participating clinic one week after CRP was performed. Because RD is an intangible variable that cannot be directly measured, we anticipated that the symptoms would be vague and vary greatly between subjects; hence, we attempted to standardize the interview procedure to ensure the validity and reliability of this variable (Fig. 2). First, the patients were asked: “Have you felt dizzy during the past seven days?” Participants were requested to consider RD as any feeling of unsteadiness, light-headiness, floating, fuzziness, giddiness, swimmy, walking on cotton, etc. If the answer was yes, they were further asked to describe whether these symptoms were continuous or sporadic. For episodic dizziness cases, patients were asked to report the frequency of the symptomatic episodes. If the episodes were very mild with occasional onset, we categorized these patients into the without-RD group. We asked patients who experienced either continuous dizziness or episodic attacks that occurred through most of the day to mark a number indicating his or her perceived severity of dizziness on a Visual Analog Scale (VAS). The VAS used a straight line of 10 cm in length; one end was marked with a 0, indicating “none,” and the other with a 10, indicating “extremely severe.” The numbers between 0 and 10 were marked at equal intervals along the line. Those who responded with three or higher were categorized as having RD, while the others were sorted into the without-RD group. We chose the VAS because of its face validity and our familiarity with its application for the assessment of outcomes in a cohort of patients with dizziness.
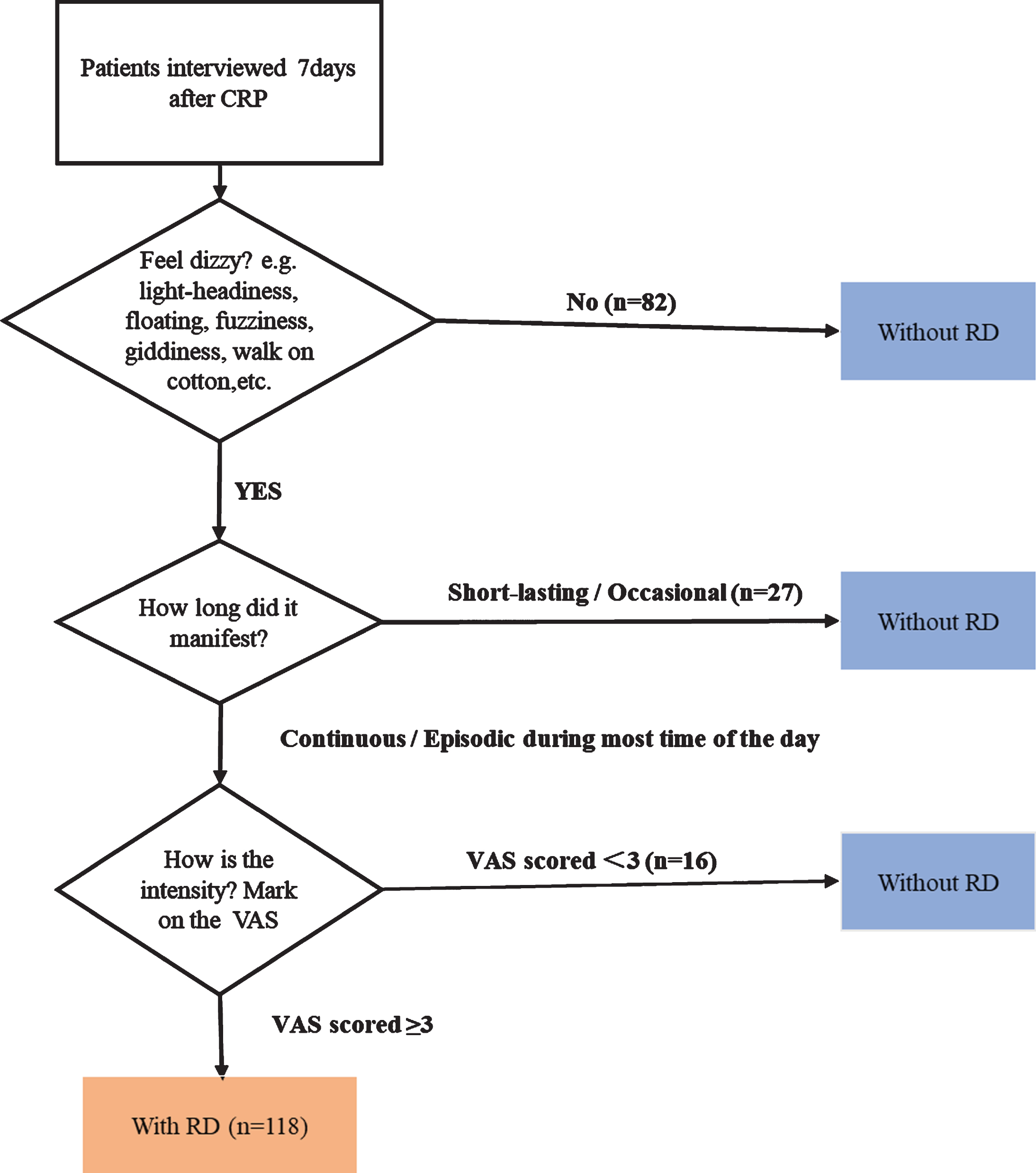
Flowchart assessing outcomes. CRP, canalith-repositioning procedure; RD, residual dizziness; VAS, Visual Analog Scale.
Statistical analyses were performed with Stata/SE (version 16, Stata Inc., College Station, TX, USA). Log-binomial regression (under a generalized linear model) was used to determine the relative risk of associations between exposure variables and RD occurrence. Log-binomial models were performed by considering all assessed exposure factors, including three demographic features (age, sex, and presence of hypertension or diabetics) and 10 clinical features (symptom duration, affected side, affected canal, CRP number, caloric test result, oVEMP response, cVEMP response, SOT, anxiety, and depression). The sample size was calculated based on the rule of thumb: 15 events per variable in the multivariate regression model. As anticipated, at least 60 subjects with RD were needed to ensure adequate statistical power when using four to six significant variables for the multivariate analysis. During data analysis, variables were included in the multivariable log-binomial model based on their association with the outcomes of the univariate analysis (p≤.20). Risk ratio (RR) was determined by controlling for the effect of potential confounders (age, sex, comorbidity, number of CRP, symptoms onset duration). Final statistical significance was established when the 95% confidence interval (CI) of the RR did not cross 1, and the p-value was <0.05.
Results
We recruited a total of 260 participants. We subsequently excluded two patients who remained unresolved after three CRPs and we considered they were erroneously included 10 who were unable to attend follow-ups, and five who developed other medical conditions during the follow-up period. Of the remaining 243 patients, 118 (48.6%) reported experiencing RD. Table 1 compares the demographic and clinical details between the groups with and without RD.
Comparison of characteristics between patients with and without residual dizziness
Comparison of characteristics between patients with and without residual dizziness
Abbreviations: RD, residual dizziness; SD, standard deviation; BPPV, benign paroxysmal positional vertigo.
The caloric test revealed that 107 patients (44.1%) presented with CP; ipsilateral CP was observed in 57 (23.5%), and contralateral CP in 50 (20.6%). DP was observed in 76 patients (31.4%), with similar proportions of ipsilateral (14.5%) and contralateral DP (16.9%). There were no differences between the RD and non-RD groups with respect to DP or CP (Table 2).
Comparison of caloric test results between patients with and without residual dizziness
Abbreviations: RD, residual dizziness; CP, canal paresis; DP, directional preponderance.
The SOT revealed that 141 (58.0%), 18 (7.4%), and 23 (9.5%) patients presented with abnormal VEST, SOM, and VIS ratios, respectively. While the VEST ratio differed significantly between the RD and non-RD groups (p < .001), the SOM and VIS ratios did not (Table 3).
Comparison of sensory organization test results between patients with and without residual dizziness
Abbreviations: RD, residual dizziness; SOM, somatosensory; VIS, visual; VEST, vestibular.
The VEMP tests demonstrated bilateral oVEMP absence in 77 patients (31.7%) and unilateral oVEMP absence in 44 (18.1%). The proportion of participants with bilateral or unilateral oVEMP absence was higher in the RD than in the non-RD group (p < .001). Twenty-five patients (11.0%) featured bilateral cVEMP absence, and 29 had unilateral cVEMP absence. The proportion of the participants with bilateral or unilateral cVEMP absence did not differ between the groups (p = .09) (Table 4).
Comparison of vestibular evoked myogenic potential test results between patients with and without residual dizziness
Abbreviations: RD, residual dizziness; VEMP, vestibular evoked myogenic potentials; oVEMP, ocular VEMP; cVEMP, cervical VEMP.
Eighty-five patients (35.0%) scored≥11 points on the anxiety domain of the HADS, indicating severe anxiety. Severe anxiety was significantly more common among those with RD than those without (p < .001). Sixty-four patients (26.34%) scored ≥11 points on the depression domain of the HADS. No difference in the depression scores was found between the groups (p = .14, Table 5).
Comparison of the severities of anxiety and depression between patients with and without residual dizziness
Abbreviations: RD, residual dizziness.
After adjusting for age, sex, comorbidities, symptom duration, affected side, affected canal, CRP number, caloric test results, and cVEMP response, the log-binomial model revealed anxiety, abnormal SOT VEST ratio, and absence of an oVEMP response as significant predictors of RD. Those with mild (RR, 2.06; 95% CI, 1.39–3.04) or severe (RR, 3.08; 95% CI, 2.17–4.38) anxiety or with an abnormal VEST ratio (RR, 2.68; 95% CI, 1.82–3.95) were more likely to develop RD. A bilateral (RR, 0.55; 95% CI, 0.44–0.69) or unilateral (RR, 0.49; 95% CI, 0.36–0.68) oVEMP response was protective against developing RD (Fig. 3).
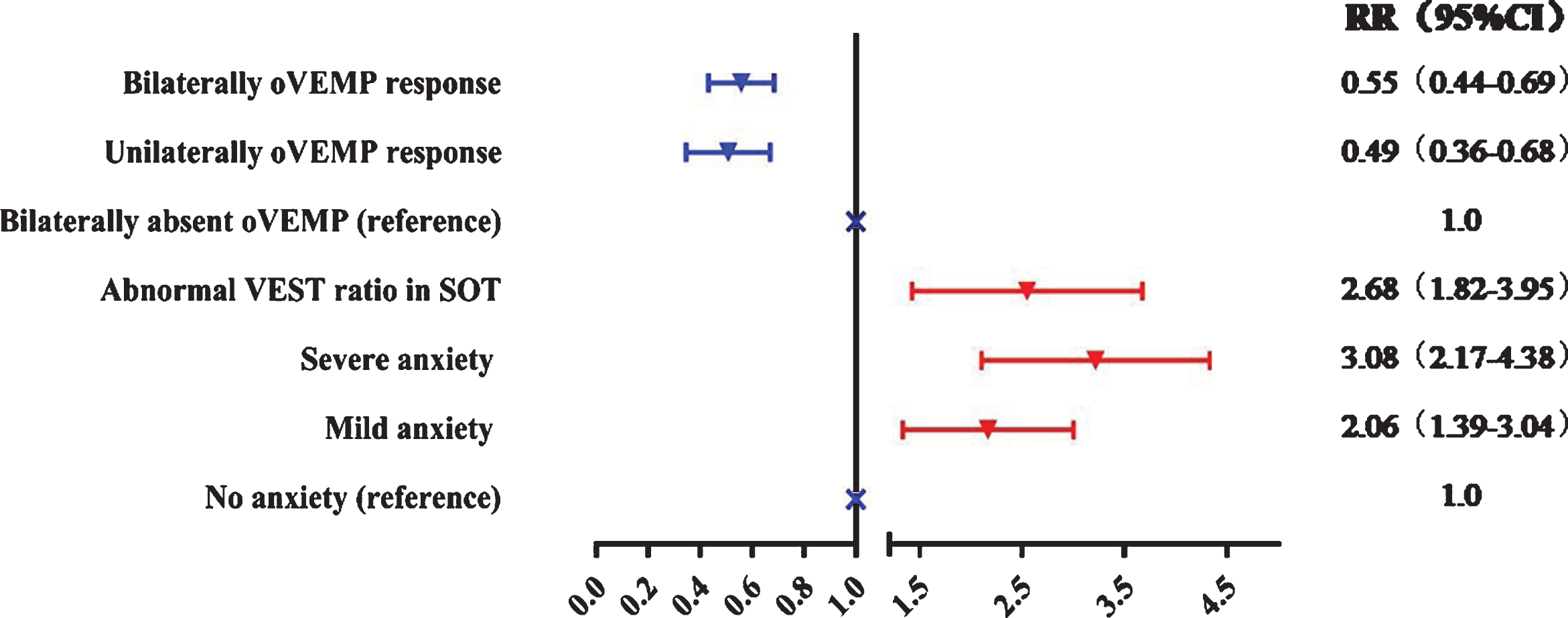
Predictors of residual dizziness after canalith-repositioning procedure. Log-binomial regression analysis for predictors of residual dizziness after administering the canalith-repositioning procedure to patients with benign paroxysmal positional vertigo. Risk ratios are plotted as dots, and horizontal lines represent confidence intervals. SOT, sensory organization test; VEST, vestibular; oVEMP, ocular vestibular evoked myogenic potential.
This study demonstrates that the occurrence of post-CRP RD in patients with BPPV can be predicted from their degree of anxiety, balance performance, and oVEMP response. Unexpectedly, no background factor was found to be significantly associated with the onset of post-CRP RD.
With an incidence ranging from 29.6% to 76.9% [10, 30], post-CRP RD is common among patients with BPPV. The variance in the rate of incidence reported in the literature is a result of different inclusion criteria and inconsistency in the definition of RD duration. To minimize sample heterogeneity, we included only patients with one episode of PSC- or HSC-BPPV and excluded those with secondary BPPV or BPPV with other concurrent inner ear disorders. We also excluded patients with anterior semicircular BPPV, as its underlying mechanism remains unclear. The criterion for the duration of RD varies in the literature. The shortest reported interval of RD was two hours post-CRP by Li et al. [10]; this definition informed an observation of RD in 60.0% (36/60) of their study population. However, when the latency period is too short, patients might still be stressed by the BPPV attack, and reports of their symptoms might be inaccurate. Defining the duration of RD as one month –the longest in the literature –Vaduva et al. reported an incidence rate of 29.6% (107/361) [31]. However, we speculated that a definition of a longer duration might result in the inclusion of cases of dizziness attributable to other vestibular diseases and cause a recall bias, particularly as residual symptoms in patients with BPPV are difficult for the patients to define [31]. Hence, we employed a definition of one week, which informed the presently reported RD incidence of 48.6%. This rate is similar to that observed in a previous study [14].
In agreement with previous studies, anxiety seemed to be the strongest predictor of post-CRP RD in our cohort (RR, 3.08; 95% CI, 2.17–4.38). Teggi et al. found a correlation between RD and anxiety in older BPPV patients (odds ratio, 6.5) [28]. Vaduva et al. observed that almost half of the patients with BPPV who were diagnosed with either anxiety or depressive disorders presented residual symptoms following CRP [31]. A recent study reported that the presentation of anxiety or depression significantly reduced the efficacy of first-time CRP and increased the risk of recurrence [34]. Occasionally considered as a somatoform disorder induced by stressful events, anxiety might manifest itself as dizziness [17]. Intense episodes of paroxysmal vertigo are stressful events owing to their versatility and unpredictability [17]. To the best of our knowledge, our study is the first to have found an association between anxiety and the risk of developing RD, as quantified by the RR. This finding implies that a comprehensive assessment of anxiety is essential for identifying patients at risk of RD, and continued emotional support and long-term follow-up are likely required for those with severe anxiety.
Previous studies have established that patients with BPPV show consistent impairment of postural control [1, 6]. Successful CRP significantly improves postural stability in a majority of patients, but not in all [1]. The SOT revealed that patients with BPPV feature a clear impairment in registering vestibular cues used to maintain balance. This impairment predicted the probability of RD onset after successful repositioning. Although several studies have explored the balance profiles of patients with BPPV, no study to date had examined its effects on predicting the post-CRP development of RD. Our findings indicate that evaluating the dynamic balance performance of patients with BPPV might be necessary to identify those with insufficient vestibular input, which could predict the risk of developing RD following CRP. Future study of the clinical implications of this finding is warranted. If possible, vestibular rehabilitation therapy should be administered proactively to this patient group in tandem with CRP to mitigate residual symptoms, shorten RD duration, and improve their quality of life [2, 24]. The attribution of the bilateral dysfunction of the otoliths in patients with BPPV to the permanent lesion of the vestibular neuroepithelium justifies the use of vestibular therapy in BPPV management. The logic of this approach remains valid even in the case of unilateral symptoms, which also cause positional vertigo and body balance disturbance [11]. Considering the vestibular system’s capacity for repair and adaptation, vestibular exercises can facilitate neural plasticity and stimulate compensatory mechanisms in the neuroepithelium, which optimizes the functional restoration of otolithic organs and promotes new multimodal sensory arrangements as well as patient rehabilitation [2, 24].
Abnormal VEMP findings in patients with BPPV have been widely reported [16, 36], implicating the degeneration of the otolith macula in BPPV etiology. Abnormal cVEMP in BPPV patients has been reported to range between 25.8% and 52% [13, 18]. This heterogeneity is mainly attributable to varying definitions of abnormalities and the use of different equipment. This study strictly defined abnormal c/oVEMPs as the absence of response. In addition, we did not include healthy controls in this study, because differences in VEMP parameters between BPPV patients and controls are too small to be accurately detected [22]. We found abnormal oVEMPs to be more common than abnormal cVEMPs in BPPV patients. Our findings are consistent with those of a recent meta-analysis as well as previous studies that found no relationship between the side on which the abnormal cVEMPs or oVEMPs were detected and the side of the affected ear in BPPV [4, 22]. Hence, unilateral BPPV does not rule out the involvement of the bilateral otolith organs, confounding the localization of the affected side of BPPV with VEMP testing [11].
To date, only three studies have directly investigated the effect of abnormal VEMP test results on residual symptoms after CRP. Seo et al. concluded that oVEMPs are associated with RD [26], while Oh et al. reported that increased cVEMP interaural amplitude difference ratio could predict RD [21]. Yetiser et al. compared cVEMP parameters between BPPV patients who suffered from RD for long or short periods and concluded that those with a long duration of RD had a considerably longer P1 latency [37]. No previous study had included both oVEMPs and cVEMPs in multivariate analysis; therefore, the confounding effects of these two parameters could not have been adequately adjusted. We found that absence of oVEMP, but not cVEMP, responses significantly predicted the development of RD. This finding implicates a damaged utricle as a cause of RD, as was previously suggested [18]. This hypothesis is informed by the understanding that oVEMP predominantly reflects utricular functions and cVEMP saccular functions. Our study found that a bilateral or unilateral oVEMP response is associated with a lower occurrence of RD in BPPV patients, whereas no relationship was observed between cVEMP and RD. Hence, we propose that conducting a cVEMP test with BPPV patients provides limited prognostic information.
Strengths and limitations
This study benefited from having considered all potential plausible factors that might be associated with the risk of developing RD in BPPV patients. To identify predictors, we used multivariate analysis and effectively eliminated confounding variables that appeared significant in the univariate analysis. Moreover, we used the RR, rather than the odds ratio, to improve the robustness of regression estimation, given that nearly half of the participants reported RD. Second, unlike most studies in this field, we used a prospective design and thus avoided recall bias. Third, we recruited a relatively large sample from multiple centers, which allowed for robust analysis with adequate statistical power.
However, the study is subject to limitations. First, our recruitment of participants was limited to five ENT clinics. Hence, caution should be exercised when extending our findings to patients seeking care in emergency or neurology departments, which older patients or those with very disabling symptoms are more likely to attend. Since there is no referral system from general practitioners in China, patients can directly visit a hospital or even a specialist. Second, we did not perform extended follow-up for the patients with RD, future study is warranted to explore the long-term outcomes in this group of patients.
Conclusion
Our study indicates that the degree of anxiety, balance performance, and oVEMP responses could predict RD after successful repositioning in BPPV patients. Abnormal vestibular input of postural balance and the presence of anxiety increase the risk of developing RD, while a bilateral or unilateral oVEMP response lowers it. Consideration of these factors could inform the treatment of patients with BPPV.
Ethical approval
The study was approved by the ethics committees of the Eye and ENT Hospital of Fudan University, Xinhua Hospital of Shanghai Jiaotong University Medical School, Zhongshan Hospital of Fudan University, Shanghai East Hospital, Shanghai First People’s Hospital of Shanghai Jiaotong University Medical School. All patients provided informed consent to participate in the study, which was performed in accordance with the Declaration of Helsinki and its later amendments.
Author contributions
All authors contributed to the study conception and design. Material preparation and data collection and analysis were performed by Peixia Wu, Jun Yang, Xinsheng Huang, Zhaoxin Ma, and Tianzheng Zhang. The first draft of the manuscript was written by Peixia Wu and Huawei Li. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
This study was supported by Science and Technology Commission of Shanghai Municipality [(STCSM), grant No. 184119551900], Shanghai, China.
Conflicts of interest
None.