
Abstract
The sensation of phantom motion or exhibition of bodily sway is often reported in the proximity of an MR scanner. It is proposed that the magnetic field stimulates the vestibular system. There are a number of possible mechanisms responsible, and the relative contributions of susceptibility on the otolithic receptors and the Lorentz force on the cupulae have not yet been explored. This exploratory study aims to investigate the impact of being in the proximity of a 7.0 T MR scanner.
The modified clinical test of sensory interaction on balance (mCTSIB) was used to qualitatively ascertain whether or not healthy control subjects who passed the mCTSIB in normal conditions 1) experienced subjective sensations of dizziness, vertigo or of leaning or shifting in gravity when in the magnetic field and 2) exhibited visibly increased bodily sway whilst in the magnetic field compared to outside the magnetic field. Condition IV of the mCTSIB was video recorded outside and inside the magnetic field, providing a semi-quantitative measure of sway.
For condition IV of the mCTSIB (visual and proprioceptive cues compromised), all seven locations/orientations around the scanner yielded significantly more sway than at baseline (p < 0.01 FDR). A Student’s t-test comparing the RMS velocity of a motion marker on the upper arm during mCTSIB condition IV showed a significant increase in the amount of motion exhibited in the field (T = 2.59; d.f. = 9; p = 0.029) compared to outside the field.
This initial study using qualitative measures of sway demonstrates that there is evidence for MR-naïve individuals exhibiting greater sway while performing the mCTSIB in the magnetic field compared to outside the field. Directional polarity of sway was not significant. Future studies of vestibular stimulation by magnetic fields would benefit from the development of a sensitive, objective measure of balance function, which can be performed inside a magnetic field.
Abbreviations
modified clinical test of sensory interaction on balance
magnetic resonance
magnetic resonance imaging
root mean square
Introduction
The human balance system utilises the integrated input from a number of different sensory systems (vestibular, visual and proprioceptive) to provide both postural stability of the body and image stability of the visual world. The relative dominance of each of these sensory inputs is situation/task dependant and is usually controlled subconsciously, although conscious control can be adopted. The vestibular end organ, located within each inner ear, comprises a system sensitive to rotational motion in various planes (the semi-circular canals) and one sensitive to linear acceleration and/or the Earth’s gravitational field direction (the otoliths). Magnetic resonance (MR) scanners use extremely strong magnetic fields to create bulk magnetisation in the form of alignment of the nuclear magnetic dipoles in the body. Many people report the sensation of phantom motion when in the close proximity of an MR scanner [10]. The mechanism behind this perception is not fully understood [11]. Previous research has identified that people working in and around high-strength magnetic fields (for example, those operating the machines) report a sensation of dizziness [10]. Anecdotally, operators standing at the end of the bore of the 7.0 T magnet can appear to sway when visual fixation is removed; for example upon closing their eyes. This effect is amplified by reducing the accuracy or efficacy of proprioceptive or somatosensory cues, when vestibular cues would become the dominant sense used for postural stability. As such, whilst it is accepted that sway is a multisensory phenomenon, it is proposed that the magnetic field stimulates or modifies the function of an individual’s vestibular system. Considering the physics of magnetic field interactions with biological systems, it is possible to postulate four mechanisms for the transduction of magnetic fields in the vestibular system: forces due to the magnetic susceptibility of vestibular structures [3]; current flow due to a net rate of change of magnetic flux [3]; magneto-hydrodynamic (MHD) effects due to rapid head movement [3, 8] and fluid pressure due to Lorentz forces originating from the interaction between hair cell currents and the magnetic field [7]. Differentiation between these possible mechanisms is not straightforward. In the present experiment we sought to examine only those mechanisms with no temporal rate-of-change of field: as the subject in the present experiment is nominally static (or has negligible velocity), any effects due to induced currents and MHD can be largely ignored [3]. However, there remains a degree of ambiguity in the understanding and interplay between the two significant remaining biophysical mechanisms of susceptibility and Lorentz forces. As the semi-circular canals detect rotational motion in the plane of the canal(s) stimulated and hence initiate a vestibular ocular reflex in the same plane in an attempt to stabilise the visual world during rotation, any erroneous asymmetric stimulation of these would most likely produce a subjective sensation of rotation/vertigo in the plane of the canals involved, centred in the head. Conversely the otoliths signal linear acceleration or gravitational direction, therefore erroneous stimulation of those would likely produce a shift in the vertical axis of the body (static lean) and/or head, and possibly a skew deviation of the eyes which would produce a perceptual shift of visual vertical/horizontal (these effects also happen in the acute stages of unilateral otolithic damage). Some of these mechanisms have been investigated [5, 6], however, the mechanism of susceptibility on the otolithic membranes has not yet been explored. The vestibular receptors of the otoliths are used by the brain to signal linear acceleration and orientation with respect to gravity by use of movement of a weighted overlying substrate. Any interaction of the magnetic field with the vestibular receptors of the cupula might also stimulate the otolithic receptors in a similar way and, if so, this might potentially alter gravitational reference and/or induce sensations of linear acceleration alongside any sense of rotation.
Future advancement in the understanding of vestibular physiology may be associated with potential clinical applications, as it may represent a novel method of vestibular stimulation [11]. Existing techniques cannot provide sustained stimulation of the sensory receptors due to hydrodynamic fatigue (i.e. any physical rotation or thermal stimulation has the effect that the relative difference in motion between the wall of the semi-circular canal, and hence cupula, and the fluid within reduces on prolonged rotation due to inertia effects or due to temperature equalisation).
The modified Clinical Test of Sensory Interaction on Balance (mCTSIB) is an example of a clinical balance test for the identification of vestibular impairment [1, 9]. Participants are observed during upright stance, and their degree of natural postural sway subjectively assessed, under various conditions designed to aid sensory isolation. Hence, assessment is made with and without visual cues (eyes open and closed) and in the presence of effective and compromised proprioceptive and/or somatosensory cues (standing on a firm support surface or on foam). Each condition increases in complexity, such that individuals with no-known vestibular deficit may experience sway across any of the conditions but should be able to maintain their stable stance as the brain effectively uses the most accurate sensory cues available to it in any given situation. In contrast, individuals with known vestibular deficit will typically perform well when appropriate visual and/or proprioceptive cues are available, but their performance will deteriorate more markedly as these cues are removed/compromised and the vestibular cues becomes more important. Evidence of impaired mCTSIB performance has been consistently shown in those with vestibular deficit [2], particularly in Condition IV. Identification of failure to maintain balance during the mCTSIB signifies a high likelihood of vestibular pathology.
This research investigated the potential mechanism behind the phantom sensation of motion when in the proximity of a magnetic field produced by a 7.0 T MR scanner, in semi-isolation from the other components of balance; visual and proprioceptive cues, using the mCTSIB.
The objectives of this study, were to qualitatively ascertain: Whether individuals with self-reported normal balance experience any subjective sensations of dizziness, imbalance or sensation of leaning or shifting in gravity when in the magnetic field Whether or not these individuals exhibit a static off-vertical-axis lean or demonstrably increased bodily sway whilst in the magnetic field vicinity of the MR scanner compared to outside the magnetic field, suggestive of shifted perception of gravity Whether degree and direction of response is reliably and repeatably dependent on direction of magnetic field lines experienced, which potentially would inform the likely dominant underlying mechanism.
Subjective sensations of vertigo/dizziness are typically associated with a relative imbalance between the semi-circular canal inputs from each ear’s vestibular end organ (responsible for the detection of angular acceleration and the subsequent generation of a compensatory vestibular ocular reflex). Otolithic dysfunction may be associated with an inappropriate shift in the body’s vertical alignment, a skew deviation of the eyes and a change in the perceived horizontal/vertical visual reference. All symptoms however vary with time as the brain adjusts to compensate for any perceived sensory conflict.
The effects of any inappropriate/unexpected change in vestibular signals (if not acute/severe) can be masked by proprioceptive and visual cues, since these are more dominant in everyday life. It is therefore more likely to see any effects of vestibular stimulation by magnetic field when a person has these visual and proprioceptive cues removed or compromised (i.e. standing with eyes closed on foam). Increased static lean or tilt while standing on foam with eyes closed would be suggestive of an otolithic effect. If this were observed, or participants were to report a sensation of static leaning or tilting when in the magnetic field, that would be again more consistent with otolithic than with semi-circular canal stimulation.
We hypothesised that individuals with self-reported normal vestibular function who passed the baseline mCTSIB and were naïve to the magnetic field may exhibit an increased degree of lean or sway and/or report increased sensations of vestibular stimulation.
Materials and methods
Participants
Experimental procedures conformed to the World Medical Association’s Declaration of Helsinki and were approved by the University of Nottingham Faculty of Medicine and Health Sciences Research Ethics Committee (reference: 421–1911). All participants gave written informed consent prior to participating in the study.
Ten healthy individuals (7 female; 3 male) were recruited into the study by advertisement. Criteria for inclusion were self-reported normal hearing, vision (or corrected-to-normal using contact lenses) and balance, no history of balance problems and no contraindications for MR. Participants were also not familiar with moving through the magnetic field of an MR scanner, and had never been in the proximity of a 7.0 T MR scanner. Participants were aged between 24 and 56 years, and the mean (±st.dev.) age was 35 (±11). Participant heights were between 158 and 180 cm tall, with mean 167 (±8) cm (individual participant heights are given in Table 1).
Mean and standard deviation values for the individual field strengths (modulus B or |B|) and gradient product (modulus GB or |GB|) experienced by participants. Participant heights given for reference
Mean and standard deviation values for the individual field strengths (modulus B or |B|) and gradient product (modulus GB or |GB|) experienced by participants. Participant heights given for reference
The mCTSIB was used to isolate each component of balance, one at a time. The individual was asked to stand upright and as still as they were able for 30 seconds in each of a series of test conditions. The test is designed such that each successive condition reduces sensory input, in order to help to determine whether or not vestibular balance cues are being used appropriately. The mCTSIB conditions are: standing on firm floor, with eyes open (subject has potential access to appropriate visual, proprioceptive and vestibular cues) standing on firm floor with eyes closed (visual cues are removed whilst proprioceptive and vestibular cues remain appropriate) standing on a foam cushion, eyes open (proprioceptive cues are compromised whilst visual and vestibular cues remain appropriate) and standing on foam cushion with eyes closed (visual cues are removed, and proprioceptive cues are compromised leaving only vestibular cues appropriate)
In healthy individuals with normal visual, proprioceptive and vestibular inputs, postural stability should be possible under all four conditions of the mCTSIB, with no falls and minimal bodily sway. Individuals with a vestibular pathology are likely to fail/perform poorly under condition IV, since their vestibular input is inappropriate and their remaining sensory cues are removed or compromised. Prematurely opening the eyes and/or taking a step would also be considered to cause a fail of any condition.
Scoring and analyses
Performance on the mCTSIB was scored qualitatively by a qualified Clinical Scientist (Audiology) experienced in assessing patients in vestibular audiology clinics in the UK. For each condition (I through IV) of the mCTSIB, and each location/orientation within the magnetic field, the participant was allocated a score for the degree of sway exhibited such that 0 was corresponded to exhibiting minimal sway and 4 corresponded to a large degree of sway. Scores of 0, 1 or 2 would be considered a pass on the mCTSIB when used in a clinical setting. Intra-subject differences were assessed using non-parametric statistical analyses in the form of Wilcoxon Signed Ranks tests performed in IBM SPSS (version 25, IBM, Armonk, NY, USA).
Procedure overview
Functional vestibular performance was first assessed using the mCTSIB in the neutral environment outside the magnetic field of the MR scanner.
Subsequently, individuals were asked to perform the mCTSIB inside the magnetic field produced by a Philips 7.0 T Achieva MR scanner (Philips Healthcare, Best, Netherlands). The mCTSIB was performed at a set of positions (each defined as a location and orientation) around the magnet, chosen for their symmetry or anti-symmetry relative to the magnetic field and head (see Fig. 1). For example, three locations, spanning both ends (‘north’ and ’south’) of the magnet and both sides of the bore were chosen such that the magnetic field profile across the head is identical, yet the polarity of the field is reversed. The susceptibility mechanism would be expected to yield identical subject response, whereas a dominant Lorentz Force mechanism would potentially reverse the effect. The subject additionally repeated the mCTSIB at different orientations in each location, for example parallel to the MR scanner bore and at 90° to the bore, in order to investigate the effect of orientation of head orientation on the measurement.
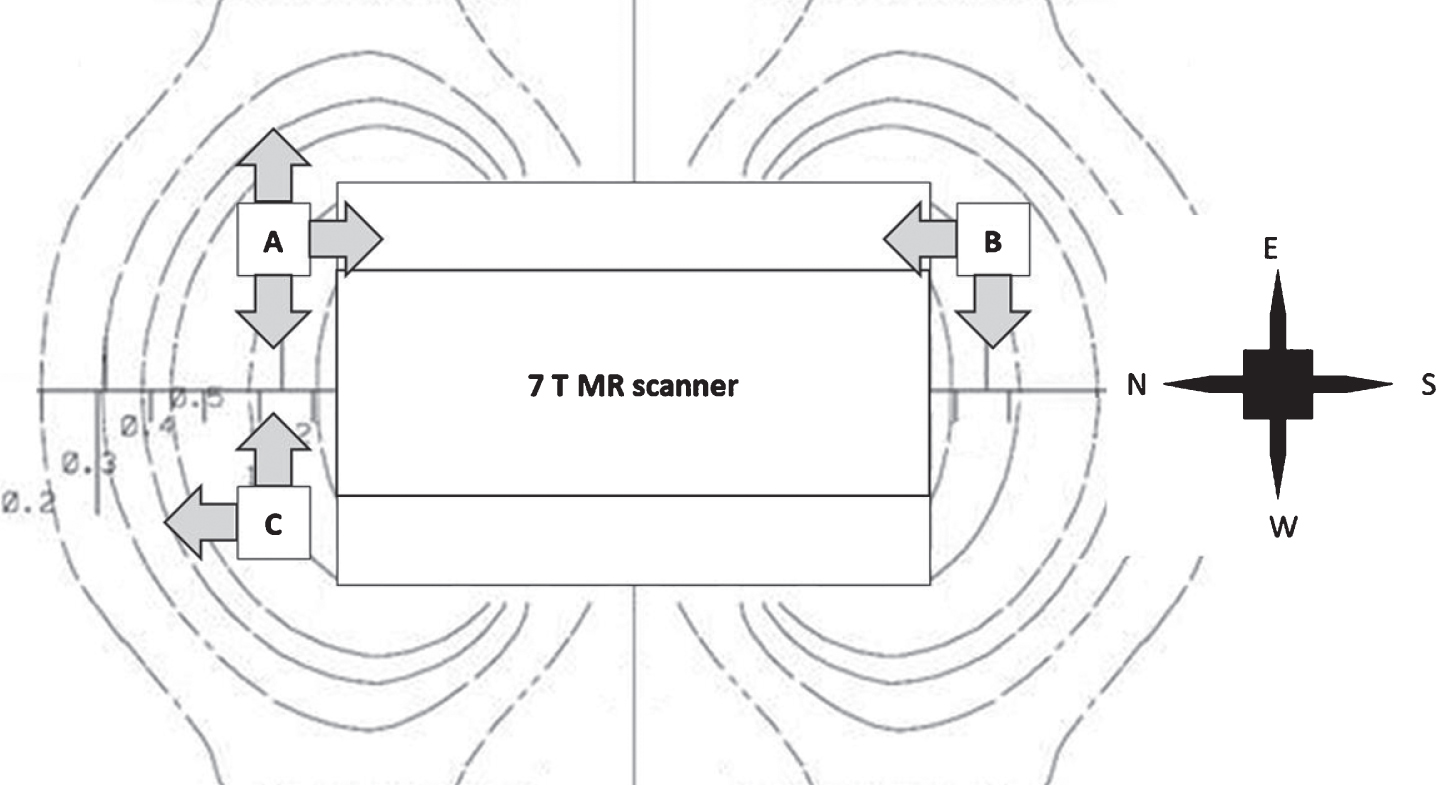
Schematic of the relative locations of mCTSIB trial positions relative to the 7.0 T MR scanner. Curved lines represent approximate field lines produced by the scanner, and numerical labels represent the strength of the magnetic field, in tesla.
A qualitative estimation of the magnitude, latency and direction of participant sway, alongside recording any subjective perception occurred at each location and orientation. Figure 1 shows the 7.0 T magnet hall and three locations for subjects in the magnet hall. Location B is magnetic field polarity reversed relative to location A. Location C is head/vestibular organ symmetric to location A.
In summary, the mCTSIB was performed in the locations given in Table 2. Magnetic field strengths (modulus B or |B|) and the field-gradient product strengths (modulus of gradient of B times B or |GB|) experienced at the location of the participant’s head, together with participant heights are given in Table 2. The mean time spent in the magnet hall (i.e. total duration of in-field testing) was 22 (±7) minutes (range 17 to 40 minutes).
MFT positions (made up of a location and orientation) at which the mCTSIB was performed. Locations A, B and C and compass point directions refer to those marked on Figure 1. The group difference from baseline represents the significance of Wilcoxon Signed Rank tests between condition IV and condition I. ‘n.s.’ denotes a non-significant difference
Video recordings were acquired using a Canon EOS 1100D Digital SLR Camera (Canon Incorporated, Ota City, Tokyo, Japan). Images were acquired at a resolution of 1280×720 pixels and frame rate of 29.97 frames per second. Each participant was recorded for mCTSIB condition IV in the first two trials (i.e. outside the magnetic field and location A, facing West). For both recordings, the camera was placed such that there was a distance of 509 cm from the edge of the foam to the nearest foot of the tripod. Approximately 30 s recording took place for each of these two trials.
During recording, the participant wore a sticker on their upper arm for motion tracking. A frame of one such video is provided in Fig. 2.

Example frame from recording of mCTSIB in MFT location ‘A’, facing West, showing the sticker on the participant’s upper arm that was used for motion tracking.
Videos were processed using in-house software written in Matlab (version 2018a, The MathWorks Inc., Natick, Massachusetts) to extract motion of the cross on the participant’s arm as a proxy for sway. Absolute in-plane displacement of the cross from its position in frame 1 was computed for each frame of each recording. Mean and standard deviation displacement across the first 25-second period of this recording was also computed. Intra-subject differences were assessed using a Mann-Whitney U-test.
Measurement of the local magnetic field
Measurements of the local magnetic field vector, B, and full gradient tensor, G, were made by constructing a small array of 12 Hall-effect sensors (HE144P Asensor Technology AB, Bålsta, Sweden) mounted on a 40 mm cubic block in order to measure the field components required. Measurements were made at locations A and C by placing the magnetic field sensor in the space occupied by the participant’s head just as they stepped off the foam following performing the mCTSIB. Measurements were not made at location B due to the length of the device cable available but can be inferred by symmetry. Mean and standard deviation values for the modulus of B (|B|) and the modulus of the gradient-field product (|GB|) are given in Table 2.
Results
mCTSIB
All (n = 10) participants passed conditions I through IV of the mCTSIB when performed outside the magnetic field both before and after magnetic field exposure. All participants passed condition I of the mCTSIB in all magnetic field test condition (MFT) positions (i.e. locations A-C in all orientations). One participant was assigned two ‘non-zero’ scores when performing condition II; in one position this was a score of 2 (still a pass) and the other position a 3 (a fail). Wilcoxon Signed Rank tests showed these differences in condition II scores were not significant across the group (p = 0.32 in both positions). A different participant was assigned a score of 2 (pass) when performing condition III in one position, which was also not significant across the group (p = 0.32).
For condition IV of the mCTSIB (vestibular cue dominant), all seven MFT positions yielded significantly more sway than at baseline, at a threshold of p < 0.05 using Wilcoxon Signed Rank tests. The significance for each of these comparisons is given in the third column of Table 2. This amounted to six participants being assigned a score of 4 in at least one MFT position (9 positions total scoring 4) and six participants being assigned a score of 3 in at least one MFT position (13 positions total scoring 2). Cumulatively, 7 participants failed a total of 22 conditions. Notably, five out of the ten participants failed both condition IV tests in both orientations of location B (behind the scanner – see Discussion). Four out of the ten participants failed the first position in the magnetic field (location A facing West – see Discussion).
Video recordings of sway
Figure 3 shows plots of displacement of the visual marker on the arm of the participant during mCTSIB condition IV. Black lines refer to the recording made of the trial outside the magnet hall (Table 2, line 1) and grey lines represent the recording made of the first trial inside the 7.0 T magnet hall (location A, facing West). Dashed and dotted lines represent individual sway recordings outside and inside the magnet hall respectively, whereas solid lines represent the group mean.

Plots of displacement of the visual marker on the arm of participants during mCTSIB condition IV both outside (black) and inside (grey) the 7.0 T magnet room. Dashed and dotted lines represent individual sway recordings outside and inside the field respectively, whereas solid lines represent the group mean.
The mean displacement over time, and across the group was 1.20 (±0.82) cm outside the field and 1.40 (±0.86) cm inside the field. The standard deviation of displacement of the marker over time was 0.59 (±0.31) cm outside the field and 0.87 (±0.45) cm inside. The difference between inside and outside the field was non-significant for the mean displacement (p = 0.5) but was significantly higher for the standard deviation of displacement inside the field compared to outside the field (T = 2.41; d.f. = 9; p = 0.04).
A Mann-Whitney U-test test between the group mean displacement outside the scanner (i.e. the solid black line on Fig. 3) and the group mean displacement outside the magnet hall (i.e. the solid grey line on Fig. 3) showed a significantly higher displacement overall occurring in the recording made inside the magnet hall (p < 0.001).
ANOVA statistics showed that there was no significant effect of field direction on the mCTSIB condition IV score. Where there was a demonstrable direction to a participant’s lean or sway during mCTSIB condition IV, this was usually in the forward/back direction. This amounted to 9 occurrences of backward lean/sway, 17 occurrence of forward sway and 16 occurrences of forward/back lean/sway, compared to one occurrence left, one occurrence right and two occurrences left/right out of 46 mCTSIB condition IV trials when lean/sway had a perceptible direction. The remaining 24 mCTSIB condition IV trials did not exhibit lean/sway with a perceptible direction. These data are not clear enough to draw any conclusions from.
There was no correlation between the modulus of the magnetic field (|B|) or the modulus of the gradient-field product (|GB|) and the participant’s score on the mCTSIB condition IV (2-tailed Spearman’s Rank Correlation, p > 0.1 for all locations and directions where local magnetic field measurements were made.
Subjective reports of perception
Participants were asked to comment on any sensations experienced after each completed mCTSIB condition IV trial. Seven out of the ten participants reported “feeling unsteady, “rocking”, “swaying”, “pulling” or “being pulled”, “pushing” or “being pushed” in directions described as “side to side”, “forwards” or “backwards”. Some participants reported sensations of “linear acceleration” or “rotating in a horizontal plane”, whereas others described it as the need “to use knees more”, “lock knees”, to “correct posture” or “correct posture by leaning”. Additionally, one participant reported feeling “tingly fingers on entering the field”.
Based on the limited number of instances where participants could confidently report which direction they perceived the motion/offset to be in, few conclusions can be drawn from the data. The directions of participant-reported perceived motion are given in Fig. 4, for each MFT position (location and orientation) within the field.

Schematic of the relative directions of participant-reported perceived motion at various trial locations and orientations relative to the 7.0 T MR scanner. Stripe directions within the arrows represent the directions the participant was facing at the time, corresponding to the stripes on the compass points. Directions of arrows correspond to directions of reported perceived motion.
Study findings
We report a novel investigation into the effect of a magnetic field of order 1 T with gradient-field products of up to 3 T2m–1 on balance performance in ten healthy adult volunteers with self-reported normal balance function. Across the group, participants performed significantly poorer on condition IV of the mCTSIB (vestibular cue dominant with vision removed and proprioception compromised) and exhibited significantly more motion or sway in video recordings of mCTSIB condition IV relative to their baseline condition. We interpret this as the subject working harder to maintain balance when in the magnetic field as compared to baseline.
Four out of the ten participants failed the first position in the magnetic field (location A facing West). As this was the first position where the mCTSIB was performed inside the magnetic field, and subsequent repeats of the mCTSIB at the same location (albeit different orientations) were failed less often, it may be that participants exhibited some adaptation to the control of their naturally occurring postural sway within the magnetic field. This may reflect a behavioural adaptation or possibly an increased tolerance or familiarity with the sensation of being within the field, which allowed them to maintain balance more easily over time.
This research set out to assess the frequency with which participants failed the later conditions (II, III and IV) of the mCTSIB in the proximity of a 7.0 T MR scanner. However, in individuals with no self-reported balance disorder, the degree of sway was very similar between conditions as measured using the mCTSIB. As such, some attempt was made to use this qualitative measure to differentiate the degree of sway exhibited, but this research shows that the mCTSIB does not provide a reliable enough differentiator of degree of sway. Therefore, we cannot report for certain whether the experimental design in the current study was insensitive to the effect we were attempting to measure, or conversely that there was no effect present to measure.
Participants were not moving with any great velocity while conducting the tests, and any motion exhibited resulting from bodily sway was slow. Therefore, any effects due to induced currents and MHD can be ruled out. As such, only mechanisms with no temporal rate-of-change of field are being considered.
If it were the case that the static magnetic field influenced the otolithic receptor, then we might expect the participant to exhibit a perceived shift in their gravitational reference axis, which would lead to a ‘tilt’ or ‘off-vertical-axis’ stance, and/or potentially a skew deviation of their eyes, rather than an increase in dynamic sway magnitude or a sense of rotation / vertigo.
While the measures used in this study only account for a clear degree of sway exhibited while in the magnetic field compared to outside the field, we also observed many/most participants adopt a different postural strategy when tested in the magnetic field compared to that outside the field (i.e. they tended to tense or lock their knees upon closing their eyes while in the magnetic field i.e. the transition from mCTISB condition I to II or III to IV). Further, many participants exhibited very small amplitude sway, or ‘jiggling’ as a result of their tense or locked knees or continually correcting motion, possibly reflecting a more conscious approach to the maintenance of their postural stability compared to a more natural sub conscious response pattern seen when testing outside the magnetic field. Additionally there may have been some influence of anticipation of a forthcoming vestibular sensation.
Avenues for future research
The present study did not aim to measure stance or any metrics of gaze. The set-up of the foam with eyes closed could additionally be used to observe any off-axis body posture since it would reduce the effectiveness of the proprioceptor cues in assessing ‘true horizontal’ in addition to removing visual room cues for earth fixed vertical/horizontal. If a participant were to fail this test in the magnetic field, having passed it in normal conditions, this would be indication of magnetic vestibular stimulation.
Future research in this area will require the use of quantitative measurements with sensitivity and specificity for objectively identifying the presence off-vertical axis postural positioning and/or a change in natural body sway in the presence of the externally applied magnetic field. Unfortunately, the mCTSIB is a qualitative not quantitative measurement technique. Further, whilst analysis of the video recordings of sway do provide a quantitative measure, the implementation of the technique in this study does not provide the required sensitivity to judge whether or not there is an effect to detect.
As mentioned previously, the recording method used may not be sensitive enough to detect this small degree of very rapid motion. This may present an opportunity for investigation of electromyography recordings in the legs between the two locations. However such recordings are likely to be plagued by artefacts caused by the magnetic field that one would expect to correlate very highly with motion. Alternative forms of motion marker could be developed in order to increase the sensitivity of the motion video recording measure, while still ensuring that the test can be performed inside a strong magnetic field. For example a mirror attached directly to the knees that would reflect the path of a laser light onto a wall for amplification of the degree of motion thus significantly increasing the sensitivity of the technique to detecting the very small degrees of rapid motion observed and reported anecdotally.
Conclusion
This initial study using qualitative measures of sway demonstrates that there is evidence in favour of MR-naïve individuals exhibiting a greater amount of postural sway while performing the mCTSIB in the magnetic field compared to outside the field (baseline). While the mCTSIB does not provide sufficient quantitative evidence for this effect, video recordings provide increased sensitivity. Due to the subtle nature of the effect, we were not able to confidently differentiate between the two biophysical mechanisms of susceptibility and Lorentz forces. As such, higher still sensitivity will be required in future studies to determine which mechanism is responsible for the effect. Understanding these mechanisms further would benefit from the development of an objective and highly sensitive quantitative measure of balance function that can be performed inside a strong magnetic field.
Financial disclosures/conflicts of interest
This research was funded/supported by the NIHR Nottingham Biomedical Research Centre and carried out at/ supported by the NIHR Nottingham Clinical Research Facilities. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. No conflicts of interest are declared.