
Abstract
BACKGROUND:
Dizziness affects 20–30%of the general population. A subgroup of dizzy patients with chronic migraine suffers vertigo implying that the migraine has a vestibular component. Vestibular migraine remains a diagnosis of exclusion based on history.
OBJECTIVE:
A link between headaches and dizziness suggests that these individuals would demonstrate dizziness and instability in complex, dynamic visual environments as a result of an inability to correctly process conflicting visual and vestibular signals.
METHODS:
A convenience sample of 74 patients (22 men and 52 women; average age 56.2 years) who presented with complaints of dizziness participated. Effects of Visual-Vestibular Mismatch (VVM) were measured using a modified VVM questionnaire. Visual dependence was measured as the error to subjective visual vertical using a computerized Rod and Frame test.
RESULTS:
Forty-two participants (56.8%) tested positive for VVM. Of these, 68.9%were patients with concomitant complaints of headaches. Visual dependence was present in 41.5%of all patients but showed no significant correlation with headache. 22.2%of patients had visual dependence and complained of headaches.
CONCLUSIONS:
These results demonstrate that sensory reweighting occurs in patients experiencing dizziness and headache, supports the role of vestibular involvement in this disorder, and provides future direction for novel interventions.
Introduction
Dizziness is one of the most common complaints of patients presenting to primary care, and affects 20–30%of the general population [36]. Dizziness is a symptom of an underlying disorder, which can involve multiple organ systems, including the central nervous system and the peripheral vestibular system [13]. One of the most common conditions associated with dizziness is migraine, which affects 40%of the adult population [31]. A subgroup of migraine patients suffer from vestibular migraine or migrainous vertigo including chronic migraine with vertigo, gaze instability, and sensitivity to visual and head motion [26]. Vestibular migraine (VM) remains a diagnosis of exclusion [19]. Many patients with VM receive only partial alleviation of their symptoms with medication and lifestyle management [2]. The criteria for treatment of this disorder with vestibular rehabilitation are inadequate, and efficacy of traditional vestibular therapy modalities for migraine-related vertigo is poor [38].
Recent evidence suggests dizziness and instability can be generated by complex visual environments (e.g., the grocery store) or wide-field of view visual motion (e.g., movie screen). due to the inability to correctly process conflicting visual and vestibular signals (visual-vestibular mismatch or VVM) [4] which falls under the diagnosis of persistent perceptual postural vertigo in the Classification of Vestibular Disorders of the Bárány society [4, 19]. Similar stimuli can trigger vertigo in patients with migrainous vertigo, suggesting that a common neurologic pathway might underlie both conditions [6, 21]. However, the prevalence of VVM in patients with non-specific dizziness is unknown [14].
The aim of this study was to explore the prevalence of VVM in a convenience sample of participants with complaints of idiopathic dizziness. The protocol was developed to explore the association between dizziness and the presence of visual-vestibular mismatch and visual dependency. We hypothesized that individuals with headache will test positive for visual-vestibular mismatch and exhibit increased weighting (sensitivity) of visual information on the Rod and Frame test [1]. The presence of VVM and visual dependency in these individuals was tested using the VVM questionnaire and the Rod and Frame protocol, respectively.
Methods
Participants
A convenience sample of 74 patients (52 females (23 –78 years old) and 22 males (23–82 years old)) was acquired from all patients presenting to the outpatient Otolaryngology clinic at a tertiary care hospital between the period of April 2018 and August 2018. Those willing to participate provided informed consent including permission to access the results of prior vestibular testing. This study was approved by the Institutional Review Board of the university (protocol #25913).
Participants were first evaluated by the attending neurotologist, including comprehensive medical history and physical examination (Table 1). Evaluation of presence and absence of headache, frequency of headaches, symptoms of aura, and prior diagnosis of migraine were abstracted from the medical records on all patients. Physical examination included full otolaryngologic and neurotologic evaluations as well as evaluation of strength, gait, tandem Romberg, and Fukuda step test.
Demographics of Participants (n = 74)
Demographics of Participants (n = 74)
aBPPV = benign paroxysmal positional vertigo.
Audiometry (including pure tone and bone conduc-tion thresholds, speech audiometry, and word recognition) was performed on all patients. Additional audiometric testing, including distortion product otoacoustic emissions and auditory brainstem res-ponse (ABR), was performed as indicated. Following clinical and audiometric evaluation, patients were consented for enrollment in the protocol. At the same visit, patients were evaluated for visual dependency (VD) and visual-vestibular mismatch (VVM) as described below.
Patients with Dix-Hallpike evaluation consistent with benign paroxysmal positional vertigo (BPPV) without evidence of other vestibular issues were not further evaluated with vestibular testing (n = 6, 8.1%). Vestibular testing was ordered for all other patients as indicated by patient history and complaints; 23 (31%) of the 74 participants did not appear for their vestibular testing. Clinical testing included vestibulonystagmography (including bithermal caloric, supine roll, Dix-Hallpike, post-headshake nystagmus, positional nystagmus and oculomotor testing) (n = 37, 50%), caloric testing alone (n = 3, 4.1%), video head impulse testing (vHIT) (n = 22, 29.7%), cervical vestibular evoked myogenic potentials (cVEMPs) (n = 25, 33.8%), and electrocochleography (n = 3, 4.1%) (Table 2). Values for abnormal test results were established by the clinical laboratory as a directional preponderance of 25%or greater with caloric testing, a vHIT gain of 0.7 or less, and cVEMPs with 30%or greater asymmetry.
Distribution of Gender with Headache, VVM, and VD
Abbreviations: VVM = Visual-Vestibular Mismatch; VD = Visual Dependence.
VVM testing
The Visual-Vestibular Mismatch Questionnaire [14, 21] was administered to each participant. This is a validated assessment tool that returns a positive or negative result based on five situational questions that provoke dizziness. VVM questions were posed to the participants in a non-leading fashion; the questions were asked as a history-taking to avoid biasing responses. Participants were scored as positive for VVM if any three questions of the five questions were answered affirmatively.
VD testing
Following completion of the VVM questionnaires, participants were seated on a backless stool with a footrest in a dimly lit room. Participants then placed a head-mounted display (HMD) (Oculus Rift, CA) over their eyes with a strap around their heads. Field of view (FOV) of this device is greater than 90 deg horizontal. The resolution is 1280×800 (16:10 aspect ratio), yielding resolution of 640×800 per eye (4:5 aspect ratio); the image is mapped for each eye. Vision of the physical world was blocked to eliminate visual cues to gravitational vertical. Correction of perspective and stereo projections for the computer graphics was provided by a 3-degree of freedom head tracker with a < 20 msec latency image update.
The Rod and Frame task was powered by Virtualis software (https://virtualisvr.com/en/) projected on the HMD. At the beginning of each trial, the virtual rod was set randomly to a left or right 45-degree angle (Fig. 1). The rod was then slowly moved toward vertical by the investigator and the participant raised their hand to signal when they perceived that the rod had achieved a vertical position. The software required that the procedure be repeated four times and these trials were then averaged for further analysis.

Illustration of visual vertical deviation on the Rod and Frame test in a visually independent (A) and visually dependent individual (B).
A logistic regression model was used to examine whether the presence of VVM or visual dependency could serve as a predictor of headache with dizziness. We evaluated the goodness of fit for our model by comparing the residual deviance (6.93) to a χ2 distribution with n–p (1) degrees of freedom [10].
Odds ratios are frequently used to quantify the strength of association between risk factors and outcomes in the clinical literature [29, 34]. Odds ratios are considered a simple quantitative interpretation to understand the magnitude of an effect [10, 30]. Odds ratios and the 95%confidence intervals (95%CI) were calculated for the three main variables (i.e., VVM, VD, and headache) to measure the association between exposure and outcome. Gender differences in the categorical variables were examined with a Chi-square test of independence.
A two-predictor logistic model (R Studio© version 1.1.414) was fitted to the categorical data to test whether the presence of headache is associated with the incidence of VVM and visual dependency. A positive coefficient for this predictor would suggest that the subject with VVM is more likely to have headache. Below is the logit model in which the response variable (VVM) is log-odds [ln (odds)]:
where p is the probability of interested outcome, α is the intercept parameter, β is a regression coefficient, and χ is a predictor. Based on our statistical expectations, a positive VVM was the indicator variable; therefore, the odds of having headache was increased by 1.3 in a subject with VVM (Table 3).
Summary of Logistic Regression Analysis
Summary of Logistic Regression Analysis
aOdds Ratio (OR). *p < 0.05.
The Rod and Frame test produces a classification of individuals as visually dependent or not visually dependent depending on the size of the error of the rod from a pure vertical orientation. All Rod and Frame data were checked for missing values and missing values were substituted via mode imputation. Results on the Rod and Frame test were compared to results previously collected from 8 young (21–50 year old) and 12 older (60–68 year old) healthy adults [32]. Based on that study, participants who set the rod more than 10 degrees off-vertical were identified as visually-dependent (Fig. 1).
Demographics of the 74 patients who participated in this study are presented in Table 1. Of these patients, 45 complained of having had significant headaches (61%), including 67.3%of female (n = 35) and 45.5%of male (n = 10) participants. Fifty-five participants had more than one clinical diagnosis following completion of evaluation and any indicated testing.
The results for clinical vestibular testing are presented in Tables 4 5. Forty-five patients had vestibular testing performed. Six patients with obvious BPPV and no other issues on history or physical examination did not have vestibular testing. One patient had severe congenital nystagmus, which precluded vestibular testing. Other patients with other obvious diagnoses which did not require vestibular testing were not tested (otitis media with effusion (n = 3), acoustic neuroma (n = 1), dense cerumen impaction onto tympanic membrane with alleviation of symptoms after debridement (n = 1), Meniere’s disease with typical abnormalities on repeat audiometry and negative MRI (n = 1), and acute viral labyrinthitis (n = 1)). Fourteen patients did not follow up for vestibular testing.
Vestibular Testing Results
Vestibular Testing Results
aAbnormal testing was defined as abnormal findings on vestibular testing, including abnormal results on VNG, vHIT, calorics, and cVEMPs. %, percentage; c/o headache, patients with any complaints of headache; final diagnosis migraine, patients with any final diagnosis of migraine, including primary diagnoses v. secondary ones.
Vestibular Results and VVM
Note: Only patients who underwent the testing and had abnormal results are reported. 125%or greater directional preponderance. 2gain of 0.7 or less. 330%or greater asymmetry.
Of those 45 patients who underwent vestibular testing, 22 (48.9%) had abnormal results on at least one component of their vestibular testing. Both caloric and vHIT results were normal in 25 of the participants (33.7%). Two participants had an abnormal vHIT test (2.70%) and 10 participants had an abnormal caloric test result (13.51%). Only three participants exhibited an abnormal cVEMP result. Fifty-five participants had more than one clinical diagnosis.
Headache was present in 34%of participants. In patients complaining of headache, vestibular testing was abnormal in 17 of the 29 patients tested (80%of those complaining of headache). In those 36 patients with a final primary or secondary diagnosis of migraine, 13 of 14 had abnormal vestibular testing results. More women than men had complaints of headache (35 vs. 10); likewise, more women than men had a final diagnosis of migraine (30 vs. 7). Normal hearing was present in 28%of participants and 22%had bilateral sensorineural hearing loss.
Rod and Frame testing indicated that 87%of all participants were visually dependent. Of these, 69%of participants with headache tested positive for VVM and 22%of participants with headache exhibited visual dependency (Fig. 2). Results of the VVM questionnaire were positive in 57%of the predominantly female (81%) participants: 34 of the 42 participants who tested positive for VVM were female (Table 2).
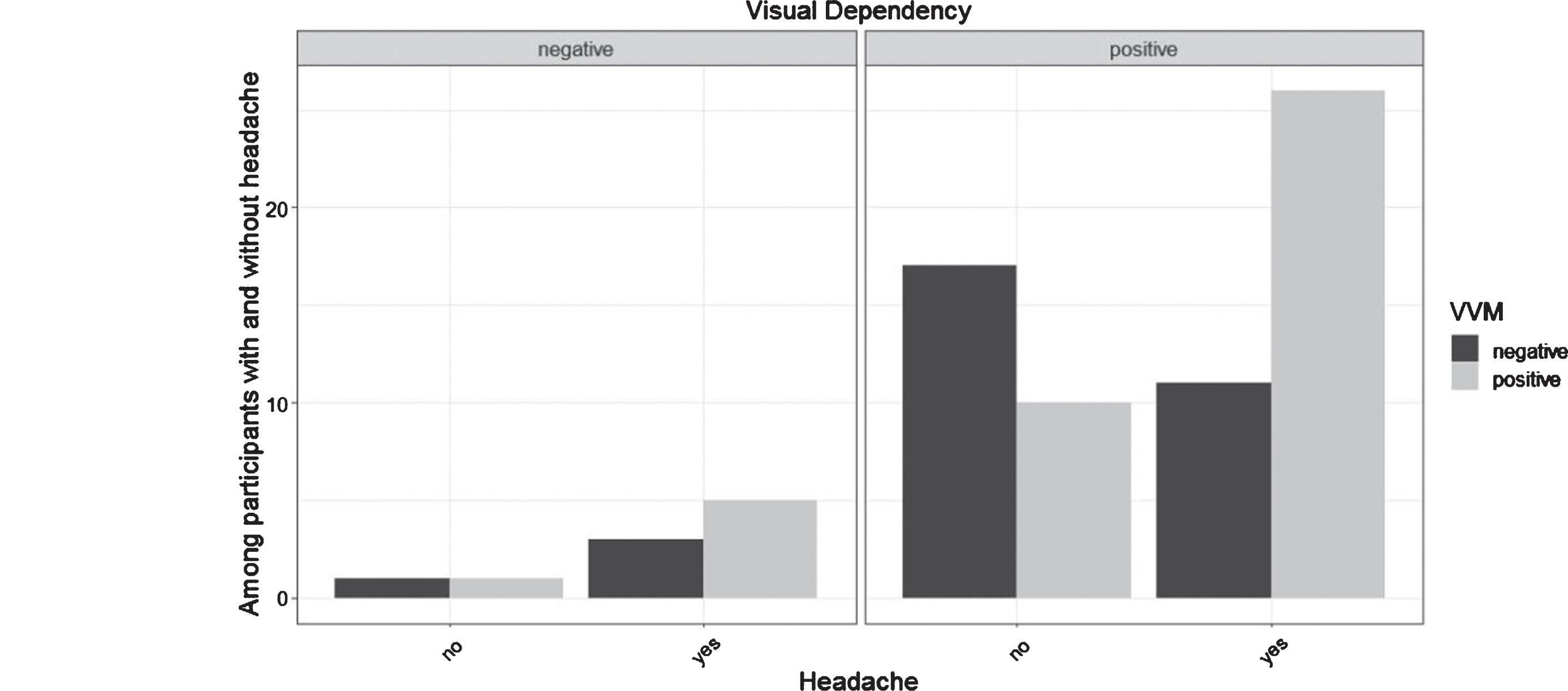
Distribution of visual-vestibular mismatch (VVM) and visual dependency (VD) among participants with and without headache.
The logistic regression model revealed that VD (P = 0.19) is not a statistically significant variable in this population. VVM, however, was significant (p = 0.01) suggesting that the presence of a headache disorder is highly associated with the presence of VVM. There was a significant reduction in residual deviance as each individual variable (i.e., VVM and VD) was added (Table 6). Significant differences between males and females were also present for VVM (p < 0.02).
Summary of Deviance of Goodness of Fit
Response variable (Headache) **p < 0.01.
The odds of having VVM among patients with headache were 3.6 times the odds of not having VVM among patients without headache. The odds of having VVM among subjects with VD were 0.85 times the odds of not having VVM among subjects who were not visually dependent.
Dizziness is one of the most common complaints leading to clinical evaluation [5, 23]. Dizziness is a symptom associated with different diseases, and is often associated with vestibular disorders [16]. Participants in this study reported experiencing dizziness an average of 2.5 years before they received the appropriate diagnosis. To our knowledge, this study was the first to investigate whether patients with headache and dizziness exhibit the signs of visual-vestibular mismatch and visual dependency. If these signs are present, then we might assume that the symptom of dizziness is generated by dysfunction in the vestibular system [9, 37]. We found that VVM, but not visual dependency, was positively associated with those patients who complained of dizziness with a history of headache.
Although not formally diagnosed as having migraine, the participants in this study meet the criteria for vestibular migraine described by the International Headache Society Classification Committee and the Committee for Classification of Vestibular Disorders of the Bárány society [4, 19]. Vestibular migraine (VM) is a challenging diagnosis as it is based on a history of exclusion [27]. A VM diagnosis may include patients without headache or without vertigo; but both classifications have identified “dizziness” as a feature of VM [19, 27].
Our discovery of a relationship between headache and VVM opens a new window of conservative management for patients with dizziness and associated headache. Optokinetic stimulation is gaining support as a treatment for alleviation of perceptual and postural symptoms in a population with VVM [35]. Optokinetic stimulation training is based on two physiological mechanisms. One physiological mechanism is central habituation, which involves systemically the short-term depression (STD) of a primary stimulus-response pathway [18, 28]. This approach to treatment focuses on provoking repeated symptoms of the central nervous system (CNS) to enhance desensitization and, therefore, compensate to the provocative stimulus. Electrophysiological studies indicate that during the habituation process, the vestibular nucleus (VN) often exhibits an opposite response pattern to repeated stimuli [7, 28]. Thus, repeated exposure to the stimulus will result in a decreased response to that stimulus.
The second physiological mechanism that can be used by physiotherapists to induce dizziness in optokinetic stimulation is combining conflicting stimuli from visual and vestibular systems to generate the feeling of dizziness [6, 33]. However, age, origin of dizziness, and duration of symptoms are factors that should be taken into account while administrating optokinetic stimulation [22, 35].
The presence of visual-vestibular mismatch often goes unrecorded during clinical exams. The only tool developed specifically to identify this syndrome is a subjective tool (the Visual-Vestibular Mismatch questionnaire [21]) that has not yet entered into general clinical use [14]. Robust optokinetic stimulation is currently gaining favor as an intervention for VVM; however, a number of individuals still poorly compensate for visual-vestibular conflict after this treatment [24, 39] and the underlying cause is unclear. It could also be that the dosages of this stimulation are not appropriately defined. Defining procedures that measure the optokinetic exposure tolerance of subjects with dizziness would contribute to developing a more individualized vestibular rehabilitation program [7, 22]. Finally, the Rod and Frame test has been shown to be an efficient utricular assessment tool by assessing subjective visual vertical which measures the degree to which a subject uses available visual cues to locate gravitational true vertical [11]. Thus, combined results of VVM and VD testing could help distinguish the vestibular mechanisms generating an individual’s symptoms. Dizziness and headache are separate symptoms; however, the co-presentation of both symptoms might be an indication of a visual-vestibular mismatch suggesting a disorder in central processing rather than at the level of the vestibular receptor [17].
The appearance of VVM was significant in patients with headache suggesting a potential association between VVM and vestibular migraine and a greater weighting of visual inputs in patients with headache in general. An association between headache and VVM implies that a novel rehabilitation management strategy may be useful for treating these patients. In particular, visual habituation exercises should be examined in controlled trials for efficacy in management of vestibular migraine and nonspecific dizziness, in which, patients may use uncommon terms or struggle to describe their symptom of dizziness.
Limitations in this study are mostly related to sample size and participant adherence. An odds ratio for predicting headache from VD (Positive) was in the expected direction, but it was statistically non-significant (p = .19). Future studies with a larger sample size are needed to replicate our results. Some patients did not receive vestibular testing because they did not show up for their appointment despite multiple reminder calls and letters; others had additional physical disorders preventing the completion of the full battery of vestibular tests. Lastly, ocular vestibular evoked myogenic potential (oVEMP) testing was not available.
Future studies should include the development of efficient methods that examine the balance system more fully in patients with vertigo and concomitant headaches, including those with migraine and vesti-bular migraine. Additionally, patients with chronic dizziness should be screened for VVM and VD.
Footnotes
Acknowledgments
The work was supported by Saudi Arabia Culture Mission (SACM).