
Abstract
BACKGROUND:
Chronic motion sensitivity (CMS) is a combination of autonomic symptoms provoked by exposure to motion. The correlation between anxiety and CMS is not yet well understood.
OBJECTIVES:
1) To compare median anxiety levels between young adults with and without CMS. 2) To examine the effect of anxiety on postural stability with immersion virtual reality. 3) To compare anxiety levels between sexes.
METHODS:
Participants included 60 adults (20–40 years), with and without CMS. After determining their current and general anxiety levels, postural stability was measured.
RESULTS:
There were significant differences in median (minimum, maximum) state- and trait-anxiety scores between participants with and without CMS, but no significant differences in median state- and trait-anxiety scores between males and females with CMS. There was a significant inverse relationship between state- and trait-anxiety scores and postural stability (ρ= –0.28, p = 0.03, and ρ= –0.32, p = 0.01, respectively). The stepwise regression analysis showed the Motion Sickness Susceptibility Questionnaire-Short Form score to be the only variable contributing significantly to postural stability (R2 = 26.2%; t = –4.5, p < 0.001).
CONCLUSIONS:
Young adults with CMS are more anxious, although anxiety does not contribute to postural stability in this group. Anxiety levels do not appear to differ between young adult males and females with CMS.
Introduction
Chronic motion sensitivity (CMS), or motion sickness, is defined as a combination of autonomic symptoms and signs provoked by exposure to passive motion as well as perceived motion, similar to that experienced in movie theaters or playing virtual reality video games [21]. The signs and symptoms of CMS include dizziness, vomiting, cold sweats, pallor, increases in salivation and drowsiness, nausea, and postural instability [4, 53]. CMS is a common condition, with 28.4% of travelers experiencing motion sensitivity [48]. In addition, Sharma [40] reported that the prevalence of CMS is 28% among Tibetans and Northeastern Indians, and 26% among Northwestern Indians. Studies have shown that the incidence of CMS is greater in females than in males [17, 34]. According to Sharma [40], females (27.3%) are more susceptible to CMS than males (16.8%). Moreover, studies have found that CMS declines with age and physical activity, including participation in sports activities [8, 40]. Furman [13] reported that CMS could have a detrimental effect on quality of life, particularly when it interferes with the ability to work, travel, or engage in leisure activities.
The underlying cause of CMS is unknown; however, sensory conflict is a widely accepted theory for explaining CMS [53]. Sensory conflict occurs when sensory inputs (visual, vestibular, and somatosensory) are mismatched [38]. Akiduki et al. [2] examined the most common conflict, which is between the visual and vestibular systems, by using virtual reality; they reported that visual-vestibular conflict provoked motion sickness symptoms and postural instability.
Paillard et al. [33] reported that the vestibular system is heavily involved in CMS. According to Eagger et al. [12], the vestibular system’s involvement in CMS makes sufferers susceptible to anxiety. This is supported by many studies describing the relationship between anxiety and vestibular dysfunction [9, 52]. This relationship is reinforced by “links between balance control and anxiety based on neural circuits that are shared by pathways mediating vestibulo-autonomic interactions and anxiety [5].”
Persistent postural perceptual dizziness (PPPD) is a more recently described vestibular dysfunction, the diagnostic criteria for which were published by Staab et al. [43]. PPPD is strongly associated with anxiety, often to a greater extent than other vestibular conditions [42, 54]. Since PPPD is a type of vestibular dysfunction and the vestibular system plays an important role in CMS, anxiety in adults with CMS requires further investigation [33]. In addition, unsteadiness while standing or walking is one of the primary symptoms of PPPD, which has also been correlated with CMS [3, 14]. Therefore, the relationship between anxiety and postural instability in adults with CMS warrants further investigation. Powell et al. [37] reported that PPPD is a “complex neurological condition that includes broad perceptual factors and may suggest that some brains are predisposed to generalized cross-modal sensory-overload. This may give rise to vulnerability to severe PPPD should a vestibular insult occur.”
According to Paillard et al. [33], there is a weak relationship between anxiety and CMS scores, with females having higher CMS and trait-anxiety scores than males. After comparing state- and trait-anxiety scores between individuals with extreme scores and individuals who had never experienced motion sensitivity on the motion sickness questionnaire, Collins and Lentz [11] found higher levels of trait-anxiety in participants with CMS but did not report an increase in state-anxiety before rotatory vestibular stimulation. Tucker and Reinhardt [49] found that individuals with airsickness have higher levels of state-anxiety.
Owen et al. [32] appraised the role of anxiety in the relationship between reported motion sensitivity susceptibility and responses to disorienting perceptual-motor conditions; they showed that although postural sway and anxiety were correlated, none of the correlations were significant. In contrast, in every condition, postural sway was significantly correlated with motion sensitivity and its reported symptoms in disorienting environments, with the correlation being strongest under conditions of inaccurate somatosensory and visual information.
Space and motion discomfort (SMD) [26] experienced by some patients with anxiety disorders is parallel to that experienced by people with CMS who do not suffer from anxiety disorders. Potentially disorienting motion environments, in which the perceptual systems involved in orientation provide ambiguous information about self-motion, induce both CMS and SMD [24, 51]. Jacob, Redfern, and Furman [25] assessed postural sway in response to optic flow in the visual field of patients with anxiety disorders and SMD; they found significant differences between anxiety and SMD patients and individuals in the control group in the degree of sway induced by the moving scenes.
Previous studies suggest that young adults with CMS have a higher dependence on visual stimuli to maintain postural stability [3, 14]. Additionally, the role of anxiety in individuals with CMS is not well understood. Building on previous research on young adults with CMS, the purposes of our study were: 1) to compare median anxiety levels between young adults with and without CMS, 2) to examine the effect of anxiety on postural stability with immersion virtual reality, and 3) to compare median anxiety levels between males and females in the CMS group.
Methods
Participants
A total of 60 young adults aged 20–40 years from Loma Linda University and the surrounding local community (30 males and 30 females with a mean age of 26.8±4.3 years and a body mass index (BMI) of 24.9±4.6 kg/m2) were recruited for this study via e-mail, word of mouth, and flyers posted around campus. Participants who had a history of neurological or musculoskeletal disorders, vestibular impairments, diabetic peripheral neuropathy, or those who were taking medications that affect balance were excluded. All participants signed an informed consent form prior to participation in the study. The study protocol was approved by the local Ethics Committee of Loma Linda University, as it complied with the ethical standards of the Declaration of Helsinki.
Group assignment
The Motion Sickness Susceptibility Questionnaire-Short Form (MSSQ-SF) was used to assign participants to one of two groups [18]. The MSSQ-SF is a valid and reliable tool used to predict individual differences in CMS caused by different types of motion [19]. The MSSQ-SF showed the following: a Cronbach’s alpha reliability of 0.87, a test-retest reliability of approximately r = 0.9, Section A (child) with Section B (adult) r = 0.68, and predictive validity for motion susceptibility r = 0.51 [19]. The MSSQ-SF score ranges from 0 to 54 points, with no cut-offs; therefore, the authors contacted the author of the MSSQ-SF, who recommended that the current authors set cut-offs based on practical or theoretical grounds. The lowest MSSQ-SF score found in a previous study of CMS participants was 7 points [14]. Accordingly, the authors decided that participants scoring 7 points or higher on the MSSQ-SF would be assigned to the CMS group, whereas those who scored 5 points or lower would be assigned to the non-CMS group. In other words, participants with MSSQ-SF scores below 7 points were considered to not have CMS. Participants who scored 6 points on the MSSQ-SF would be excluded to create a “gap” between the two groups; however, no participants scored 6 points. Thirty participants (17 males and 13 females) had CMS, while 30 participants (13 males and 17 females) did not.
Questionnaires
The State and Trait Anxiety Inventory (STAI) was used to measure the presence and severity of current state and general trait-anxiety. The STAI includes two subscales: the State-anxiety Scale (state-anxiety), which evaluates the current state of anxiety by asking participants how they feel at the time, using 20 statements that measure their subjective feelings of apprehension, tension, nervousness, worry, and activation/arousal of the autonomic nervous system. The Trait-anxiety Scale (trait-anxiety) evaluates general aspects of participants’ anxiety proneness using 20 general statements that measure their calmness, confidence, and security. The range of scores for each subscale was 20–80, with higher scores indicating greater anxiety. A score of 39 or higher implies clinically significant symptoms for the state-anxiety scale [1, 27].
A simple questionnaire was developed and used to determine participants’ activity levels to control for the potential influence of physical activity on CMS. Participants rated their exercise frequency on a scale that ranged from 1 to 3 (1 = never; 2 = sometimes; 3 = often). Several studies have demonstrated that physical and sports activities may improve postural stability and reduce anxiety levels (state- and trait-anxiety) [7, 50].
Apparatus
Bertec Balance Advantage computerized dynamic posturography with immersion virtual reality (CDP-IVR; Bertec Corporation; Columbus, OH) was used to measure postural stability during visual conflict. Participants stood within an immersive environment and a curved virtual reality projection screen emitted an optokinetic visual flow of an infinite tunnel, in the form of alternating black and white circular patterns moving toward the participant. The objective was to create a visual sensation that the participant was moving in an anterior direction towards the infinite tunnel. The density and velocity of the circular pattern were constant for all participants, and the laboratory lights were turned off to further reduce external visual influences (Fig. 1). The CDP-IVR test-retest reliability composite score was 0.92, and the validity composite score was 0.84 [47]. The CDP-IVR calculates center of gravity displacement and postural sway to provide an overall postural stability score, reported as an equilibrium score, calculated as follows: Signals from the participants’ efforts to maintain balance are sampled and analyzed at 1,000 Hertz, and the sway path is computed. The testing protocol calculates the sway path with equilibrium scores that are quantified by how well the participant’s sway remains within the expected angular limits of stability during each testing condition. The following formula was used to calculate the equilibrium score:

Participants were fitted with a safety harness, placed on a stable platform, and exposed to computerized dynamic posturography with immersion virtual reality.
Equilibrium Score (ES) = ([12.5 degrees –(the taMAX–the taMIN)]/12.5 degrees) *100 [41].
The ES uses 12.5° as the normal limit of the anterior-posterior sway angle range; taMAX is the theta maximum, and taMIN is the theta minimum. Theta is a Greek symbol often used to represent angles in two different planes. In the case of computerized dynamic posturography, angle theta is used to describe the maximum and minimum anterior and posterior sway angles in degrees. The sway angle was calculated as follows: Sway Angle = arcsin (COGy/[0.55*h]), where y = anterior-posterior sway axis, and h = the subject’s height (in centimeters or inches). The inverse sine of the center of gravity was divided by 55% of the participant’s height. Participants exhibiting lesser sway achieved equilibrium scores near 100, whereas participants whose sway approached their limits of stability achieved scores near zero [6].
Before measuring postural stability, each participant took off their footwear and was fitted with a safety harness. Postural stability was measured on a stable platform with the participant’s eyes open, while they focused on a virtual reality infinite tunnel visual flow (Fig. 1). Participants in both groups received one familiarization trial to acquaint them with the equipment [20]. Postural stability was measured three times, with each measurement lasting 20 seconds; the mean of the three measurements was recorded. During testing, the position of the participant’s feet was monitored. In addition, the participant was instructed to stand with their arms at their sides.
Statistical analysis
Data analysis was conducted using the Statistical Package for the Social Sciences (SPSS) for Windows, version 22.0 (SPSS, Inc., Chicago, IL). The sample size needed for this study was estimated using a medium effect size of 0.50, a power of 0.80, and a level of significance (α) of 0.05. The mean±standard deviation (SD) or median (minimum, maximum) was computed for quantitative variables and frequency (percentage) for categorical variables. A Chi-square test of independence was used to examine the association between gender and physical activity by group. To assess the normality of the quantitative variables, Shapiro–Wilk tests and box and whisker plots were performed. To compare mean age, height (m), weight (kg), and BMI (kg/m2) between the CMS and non-CMS groups, an independent t-test was used. Since the distribution of anxiety levels was not approximately normal, the differences in median STAI scores by group type were examined using the Mann-Whitney U test. Among adults with CMS, we examined differences in median STAI scores between males and females using the Mann-Whitney U test. To examine the effect of anxiety on postural stability, Spearman’s correlation was conducted. To determine whether STAI and MSSQ-SF scores were significant predictors of postural stability, a stepwise regression analysis was performed. The level of statistical significance was set at p < 0.05.
Results
There were no significant differences in mean height (m), weight (kg), or BMI (kg/m2) at baseline between participants with CMS (n1 = 30) and those without CMS (n2 = 30) (t = –0.4, p = 0.173; t = 1.4, p = 0.173; and t = 0.2, p = 0.828 respectively; Table 1). The frequency distribution of gender and physical activity was not significantly different by group (χ2 = 1.1, p = 0.219 and χ2 = 0.6, p = 0.432, respectively). However, there was a significant difference in mean age between the two groups (t = 2.1, p = 0.04, Table 1).
Mean (SD) of general characteristics by group (N = 60)
Mean (SD) of general characteristics by group (N = 60)
*p < 0.05. Abbreviations: CMS = chronic motion sensitivity; BMI = body mass index; MSSQ-SF = Motion Sickness Susceptibility Questionnaire-Short Form; SD = standard deviation. aChi-square test of independence; bIndependent t-test; cMann-Whitney U test.
There was a significant difference in median (minimum, maximum) state-anxiety scores between participants with CMS and those without CMS (26.0 [20, 47] and 21.5 [20, 48], respectively; Z = –2.3, p = 0.024; refer to Fig. 2). In addition, there was a significant difference in trait-anxiety scores between the two study groups (33.5 [20, 49] and 28.5 [21, 62], respectively; Z = –2.4, p = 0.016; refer to Fig. 3). These results did not change after controlling for age.
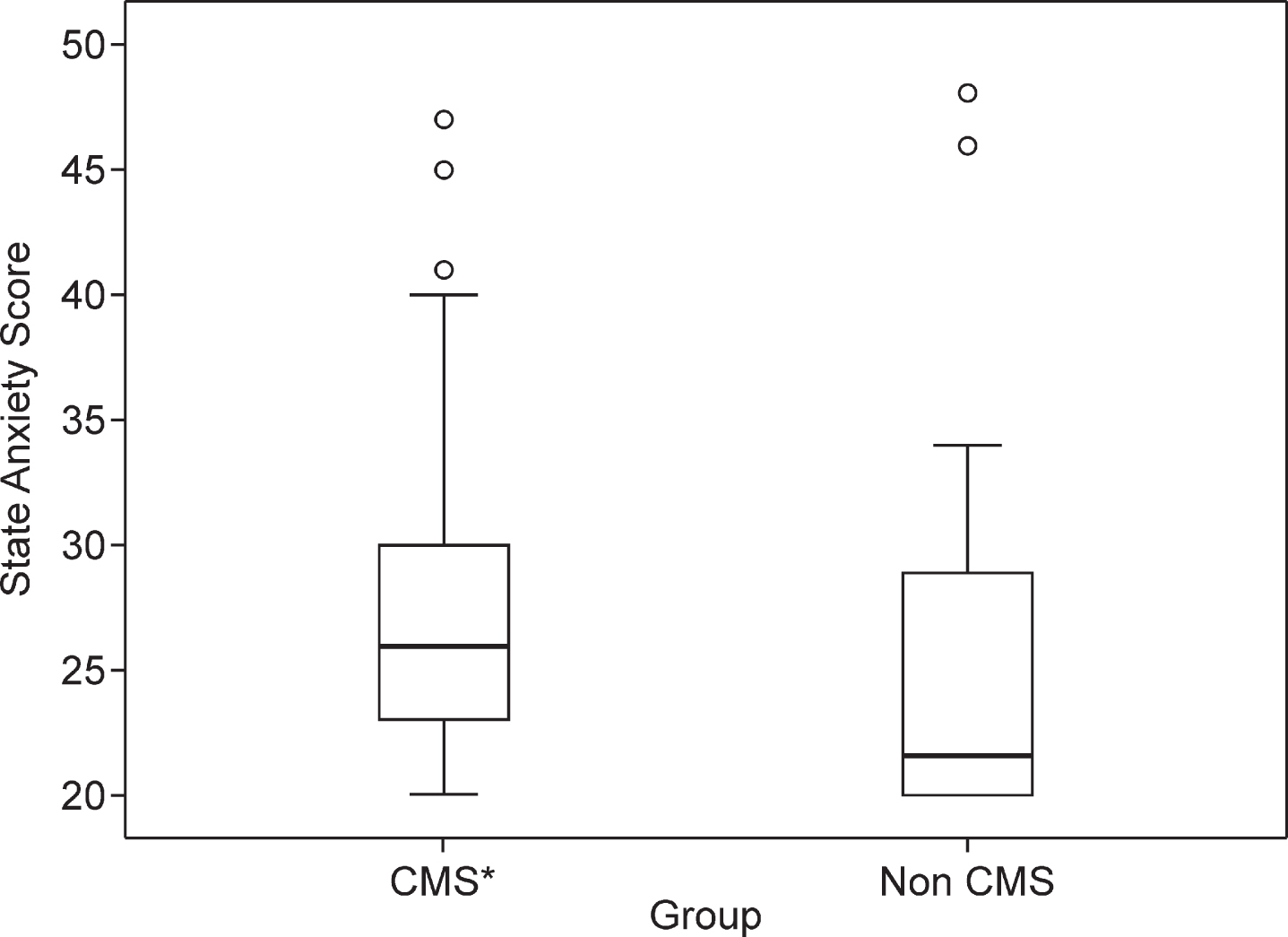
Box and Whisker plot of state-anxiety score by group (N = 60).
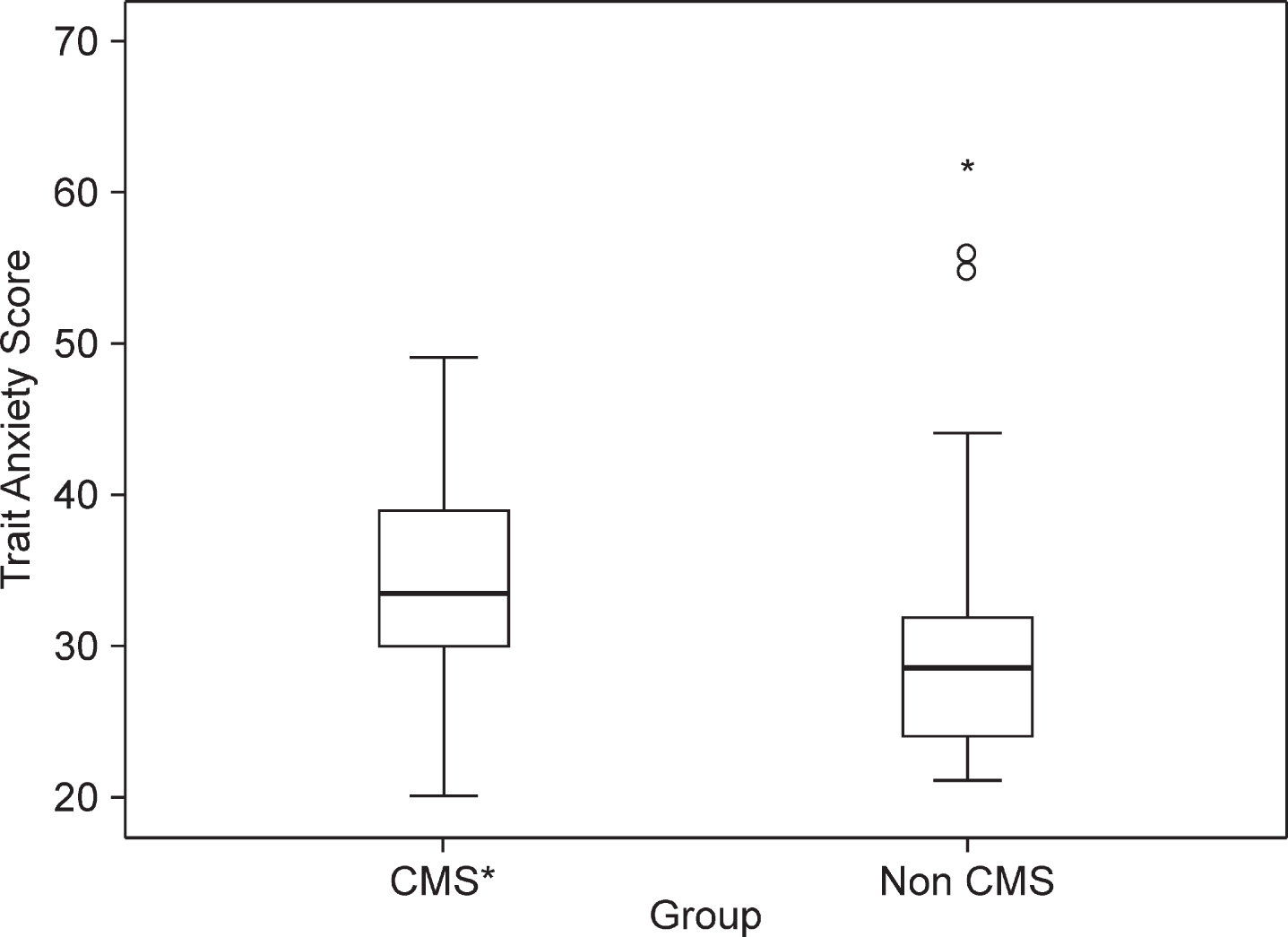
Box and Whisker plot of trait-anxiety score by group (N = 60).
Among adults with CMS, there was no significant difference in median state-anxiety scores between males and females (25.0 [20, 47] and 27.0 [20, 45], respectively; Z = –0.04, p = 0.97). Similar findings were observed for median trait-anxiety scores (37.0 [20, 49] and 31.0 [23, 45], respectively; Z = 1.23, p = 0.21).
In terms of the effect of anxiety level on postural stability, there was a significant inverse relationship between state- and trait-anxiety scores and postural stability (ρ= –0.28, p = 0.03 and ρ= –0.32, p = 0.01, respectively). The results of the stepwise regression showed that the MSSQ-SF score was the only variable that contributed significantly to postural stability (B = –0.21, SE (B) = 0.05, 95% confidence interval (CI) (–0.30, –0.11), R2 = 26.2%; t = –4.5, p < 0.001; Table 2). Further, 26% of the variability in postural stability is explained by its relationship with the MSSQ-SF score. State- and trait-anxiety scores, however, were not significant predictors of postural stability (p = 0.467 and p = 0.329, respectively). There was no collinearity among the variables in the regression model (Tolerance = 1.0).
Results of stepwise regression analysis for predicting postural stability
Abbreviations: MSSQ-SF = Motion Sickness Susceptibility Questionnaire Short-Form; SE = Standard Error.
In the present study, the median state- and trait-anxiety scores were compared between young adults with and without CMS. The results demonstrated that young adults with CMS had higher scores than those without CMS, suggesting that young adults with CMS are more anxious than those without CMS. For state-anxiety, the findings of this study are consistent with those of Tucker and Reinhardt [49], who compared the state-anxiety level between individuals with and without airsickness. However, the results of this study contradict the findings of Collins and Lentz [11], who used the STAI-X. The STAI-X was revised in 1983 to the STAI-Y, used in the present study. The STAI-Y is a simplified version of the original measure, with improved differentiation and stabilization among the anxiety factors compared to the STAI-X [54, 41]. The revised version may have facilitated the detection of the difference between the two groups despite the tool used for assigning the groups. Moreover, state-anxiety scores measure the individual’s anxiety level at the time of testing; the lab environment, including the CDP-IVR, may play a role in increasing state-anxiety because the participants may feel that the CDP-IVR could provoke sickness, which was mentioned in the informed consent. Examining state-anxiety is important in this situation because it mimics the real situations that individuals with CMS experience. Regarding trait-anxiety, the results of the present study agree with studies showing that there is a correlation between anxiety and CMS, and that individuals with CMS are more anxious than those without CMS [11, 32]. Even though participants with CMS had significantly higher median anxiety scores than those without, the score did not reach the cut-off point of the questionnaire. The median score for participants with CMS was 33.5, but only a score of 39 or higher indicates a need for medical attention.
Postural instability was shown to be correlated with CMS, especially when the visual and somatosensory inputs are misleading [32]. We previously found that participants with CMS depend on visual stimuli to maintain postural stability [18]. An infinite tunnel was used in the present study to examine the correlation between anxiety and postural stability when the visual information was misleading. Although there was a correlation between anxiety and postural stability, anxiety did not mediate the responses to misleading visual information. These findings are consistent with those of Owen et al., [32] who had similar results regarding the role of anxiety in postural stability. However, the results obtained by Owen et al. differ from the results of our study in terms of the relationship between anxiety levels and postural stability. Our study suggests that anxiety does not play a role in postural stability among young adults with CMS. Given the complexities of multi-modal sensory processing, as described by Staab et al. [43], more research is needed to determine the precise relationship between anxiety and postural stability.
Females are reportedly more susceptible to CMS than males; however, the cause of this difference is unknown [17, 34]. Paillard et al. [33] reported that females have higher trait-anxiety scores than males. However, the results of our study show that there is no difference in median state- and trait-anxiety scores between male and female participants with CMS. The lack of statistical significance may be attributed to an insufficient sample size. The results suggest that anxiety levels are not influenced by gender among adults with CMS.
Conclusion
The results of this study suggest that young adults with CMS are more anxious than those without CMS; although this anxiety level was higher among individuals with CMS, their anxiety did not require medical attention. Moreover, this anxiety does not mediate postural instability. In addition, anxiety levels are not influenced by gender among adults with CMS.
A limitation of the present study was using a simple self-report questionnaire concerning exercise frequency levels. It is plausible that minimizing avoidance behaviors and engaging in physical activities would improve postural stability and anxiety levels. Further studies should include a valid physical activity questionnaire to further explore its impact on anxiety and CMS. Future samples should also include older adults to expand the population range concerning anxiety and CMS.
Footnotes
Acknowledgments
The authors thank the University of Tabuk and Loma Linda University for supporting this research. There are no conflicts of interest to declare.