
Abstract
BACKGROUND:
Obstructive sleep apnea (OSA) could influence peripheral vestibular function adversely via intermittent hypoxia and its consequences.
OBJECTIVE:
This study aimed to evaluate the risk of peripheral vestibular disorders in OSA using a nationwide population-based retrospective cohort study.
METHODS:
The National Health Insurance Service–National Sample Cohort represents the entire Korean population from 2002 to 2015. OSA was defined as individuals who had used medical services twice or more under a diagnosis of OSA(G47.33 in ICD-10). A comparison cohort consisted of socio-demographically matched non-OSA subjects in a ratio of 1:4. The incidences of benign paroxysmal positional vertigo(BPPV), Meniere’s disease, and vestibular neuritis were evaluated in each cohort.
RESULTS:
A total of 2,082 individuals with OSA and 8,328 matched non-OSA subjects were identified. The incidence rates(IRs) of peripheral vertigo in OSA and non-OSA were 149.86 and 23.88 per 10,000 persons, respectively (Ratio of IR, IRR = 6.28, 95%CI 4.89 to 8.08). In multivariable analysis, the risk of peripheral vertigo was significantly higher in OSA(adjusted HR = 6.64, 95%CI 5.20 to 8.47), old age(adjusted HR = 1.03, 95%CI 1.02 to 1.04), female sex(adjusted HR = 1.92, 95%CI 1.48 to 2.50), and comorbidities(adjusted HR = 1.09, 95%CI 1.003 to 1.19). The IRRs of each vestibular disorder in the two groups were 7.32(95%CI 4.80 to 11.33) for BPPV, 3.61(95%CI 2.24 to 5.81) for Meniere’s disease, and 9.51(95%CI 3.97 to 25.11) for vestibular neuritis.
CONCLUSIONS:
Subjects diagnosed with OSA had a higher incidence of peripheral vestibular disorders than those without OSA, according to national administrative claims data. It is recommended to take peripheral vertigo into account when counseling OSA.
Introduction
Obstructive sleep apnea (OSA) syndrome is one of the most prevalent chronic respiratory disorders, which is characterized by recurrent pharyngeal collapse during sleep. Repetitive episodes of airflow limitation causing oxygen desaturation and hypercapnia lead to increased respiratory drive followed by frequent arousal [19]. Intermittent hypoxia, hypercapnia, and disturbed sleep architecture are associated with various pathological phenomenon resulting from OSA [19]. Previous literature showed that OSA increased the risk of systemic diseases including hypertension, stroke, myocardial infarction, heart failure, diabetes, headache, etc [10].
Several laboratory studies have shown that peripheral vestibular end-organs and the vestibular nucleus can be damaged by hypoxia or reactive oxygen species [4, 35]. Previous cross-sectional studies reported that caloric responses were decreased in subjects with OSA, especially in cases with worse apnea-hypopnea index [8, 13]. In a population study, the risk of vertigo was significantly higher in individuals with OSA [29]. In addition, the incidence of Meniere’s disease was reported to be higher in female and in middle-aged subjects with OSA [14]. Thus, not only may subjective dizziness be related to daytime somnolence and OSA, but peripheral vestibular disorders may also be associated with OSA [8, 29]. So far, however, there has been a lack of studies assessing the incidence of specific vestibular diseases in individuals with OSA.
In the present study, we hypothesized that the incidence of peripheral vestibular disorders would be affected by preexisting OSA. A population-based cohort study using the Korean National Health Insurance Service (KNHIS) Sample Cohort database was designed to compare the incidence of peripheral vestibular disorders in individuals with OSA and matched non-OSA subjects. Disorders causing peripheral vertigo included BPPV, Meniere’s disease and vestibular neuritis, which are known to be due to pathologies of the otolith organs, endolymphatic system, and vestibular pathway, respectively. In short, this study aimed to evaluate the risks of peripheral vestibular disorders in individuals with OSA using a nationwide claims data.
Methods
Study population and data collection
The NHIS system of South Korea is a single-payer insurance system covering the entire registered Korean population. This study used the NHIS–National Sample Cohort, which was established to represent the entire Korean population of 50 million by systematic stratified random sampling [17]. The Sample Cohort was comprised of 2.2%of the total Korean population (1 million) in 2002 and has been followed since.
The cohort database included personal information, diagnostic codes, procedures and prescription codes, socio-economic information (residence and income), records of medical service use, and death records. After it was established, the relevance of the Sample Cohort was verified by comparing its data with that of the entire Korean population.
This study obtained permission for use of the NHIS Sample Cohort database, which consists of data from January 2002 to December 2015 (http://nhiss.nhis.or.kr/bd/ab/bdaba021eng.do). The diagnostic classifications followed the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10).
The authors declare no conflict of interest with the NHIS. This investigation was approved by the local ethics review board (Hanyang University Institutional Review Board, HYU-2020-047) and performed in accordance with the Declaration of Helsinki and good clinical practice guidelines.
Study design and selection of cohorts
A total of 3,037 individuals diagnosed and managed with OSA were identified from 1 Jan 2002 to 31 Dec 2015 (Fig. 1). Participants who had been diagnosed with dizziness-related disorders (H81, H82, and H83, peripheral vertigo; R42, subjective dizziness; I63 and I61, cerebral infarction and hemorrhage) before the study was initiated were excluded.
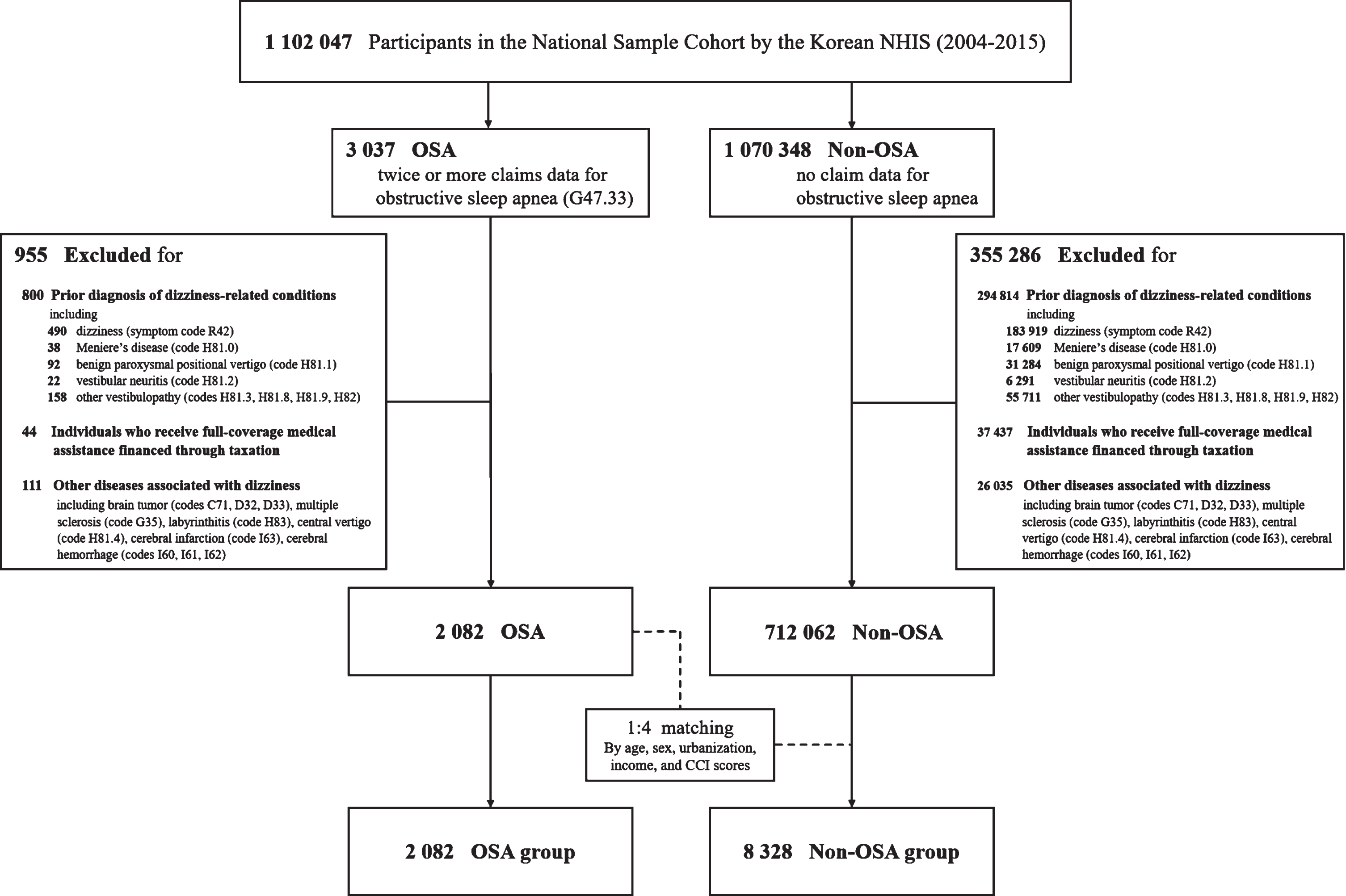
Flowchart of the construction of the cohorts.
The OSA patients were matched 1:4 with comparison participants who had never been diagnosed with OSA [1, 26]. The matching process was conducted for age, sex, income, dwelling place, and Charlson Comorbidity Index (CCI) scores. The latter is calculated based on the presence of seventeen selected medical conditions including congestive heart failure, dementia, diabetes, liver disease etc [6]. The score ranges from 0 (no comorbidities) to 33 after weighting each item according to the validated method [6]. To prevent selection bias during the matching process, the participants were sorted using a random number order, then selected from top to bottom. It was assumed that the comparison participants were involved at the same time as the corresponding matched OSA patient. Propensity score matching was performed.
In a total of 2,082 OSA patients and 8,328 matched non-OSA subjects, development of peripheral dizziness was evaluated from the time of enrollment to December 31, 2015.
To receive insurance benefit in South Korea, the medical records have to be submitted to the NHIS system by the health care providers at each medical use. Thus, claims data include major diagnoses of disease given by the physicians according to ICD-10 codes. The OSA group was defined as individuals with the diagnostic code of OSA (G47.33) in ICD -10 who used medical services twice or more under the diagnosis. Peripheral vertigo was defined as subjects with the diagnostic codes of Meniere’s disease (H81.0), BPPV (H81.1), or vestibular neuritis (H81.2). Diagnostic codes of other peripheral vertigo (H81.3), other disorder of vestibular function (H81.8), disorders of vestibular function, unspecified(H81.9) and vertiginous syndromes in disease classified elsewhere(H82) were also assessed.
Statistical analysis
Data were analyzed with the use of SAS Enterprise Guide software version 7.1 (SAS Institute, Inc., Cary, NC). To reduce possible sample variability in the large comparison cohort, 1:N (1 to 4) propensity score matchings were performed for age, sex, urbanization, income, and CCI scores [1, 26]. As the consisted comparison groups showed good comparability with standardized mean differences for all factors of < 0.1, the 1:4 matching method with the smallest standardized mean differences of gender was selected for the analysis. The demographic characteristics of the study population are presented as percentages for categorical variables and medians and interquartiles for continuous variables. The standardized difference was calculated to assess the balance of covariates after matching. Incidence rates (IR) per 10,000 person-years were calculated with 95%confidence intervals. The ratio of IR (IRR) for occurrence of peripheral type dizziness was calculated in the sleep apnea cohort relative to the non-sleep apnea cohort. A Cox proportional hazards regression model was used to analyze the risk of dizziness (Hazard ratio, HR).
Data availability
This study used the Korean NHIS Sample Cohort database with permission. Data will be shared on request with any qualified investigator for purposes of replicating procedures and results.
Results
Demographic characteristics of the study population
During the study period, a total of 3,037 individuals used medical services twice or more under a diagnostic code of OSA. Excluding subjects previously diagnosed with dizziness-related conditions, 2,082 individuals with OSA and 8,328 matched comparison participants were identified (Fig. 1). About 83%of study cohorts in both groups were male (Table 1). The average follow-up periods in the two groups were 4.8 years and 5.4 years, respectively (Table 1).
Comorbidities and sociodemographic characteristics of the study cohort
Comorbidities and sociodemographic characteristics of the study cohort
OSA, obstructive sleep apnea. SD, standardized difference. Continuous variables are presented as median (25th–75th quartile). Categorical variables are presented as N (%).
For peripheral vertigo, including BPPV, Meniere’s disease, vestibular neuritis, and other peripheral vestibulopathy, the overall IR of the OSA group was 149.86 per 10,000 persons, 6.28-fold (95%CI of IRR 4.89 to 8.08) that of the non-OSA group (23.88 per 10,000 persons) (Table 2). The incidence in the OSA group was meaningfully higher for both males and females, as well as for ages under and over 50 years (Table 2).
The incidence rates (IR) and incidence rate ratios (IRR) of peripheral vestibular disorders in the OSA and non-OSA cohorts
The incidence rates (IR) and incidence rate ratios (IRR) of peripheral vestibular disorders in the OSA and non-OSA cohorts
Peripheral vestibular disorders including benign paroxysmal positional vertigo, Meniere’s disease, vestibular neuritis, and other peripheral vestibulopathy. OSA, obstructive sleep apnea. aIR: incidence rate (per 10,000 persons). bIRR: incidence rate ratio. Clinically meaningful differences of IRR are highlighted in
In a multivariable analysis of the whole cohort, pre-existing OSA was a significant risk factor for developing peripheral vertigo (adjusted HR = 6.64, 95%CI 5.20 to 8.47) (Table 3). In addition, older age (adjusted HR = 1.03, 95%CI 1.02 to 1.04), female sex (adjusted HR = 1.92, 95%CI 1.48 to 2.50), and higher comorbidity score (adjusted HR = 1.09, 95%CI 1.003 to 1.19) appeared to increase the risk of peripheral vestibular disorders (Table 3).
Multivariate analysis of risk factors for the development of peripheral vestibular disorders during the follow-up period in the whole cohort
Peripheral vestibular disorders including benign paroxysmal positional vertigo, Meniere’s disease, vestibular neuritis, and other peripheral vestibulopathy. Clinically meaningful differences are highlighted in
The incidence of each diagnosis was meaningfully higher in OSA cohort than non-OSA group: BPPV, IRR = 6.28 (95%CI 4.89 to 8.08); Meniere’s disease, IRR = 3.61 (95%CI 2.24 to 5.81); Vestibular neuritis, IRR = 9.51 (95%CI 3.97 to 25.11); other peripheral vestibulopathy, IRR = 6.70 (95%CI 4.71 to 9.62) (Table 4). For any of diagnoses, there was no meaningful difference of IRR between males and females, or those over and under 50 years (Table 4).
The incidence rate ratios (IRR) of benign paroxysmal positional vertigo, Meniere’s disease, and vestibular neuritis betweenthe OSA and non-OSA cohorts
The incidence rate ratios (IRR) of benign paroxysmal positional vertigo, Meniere’s disease, and vestibular neuritis betweenthe OSA and non-OSA cohorts
OSA, obstructive sleep apnea. aIR: incidence rate (per 10,000 persons). bIRR: incidence rate ratio. Overall values in each diagnosis are highlighted in
This study evaluated the incidence of peripheral vestibular disorders in individuals with OSA using nationwide medical claim data. Individuals diagnosed with OSA showed meaningfully higher incidence of peripheral vertigo than subjects without OSA (IRR = 6.28, adjusted HR = 6.64). The incidences of BPPV, Meniere’s disease, and vestibular neuritis in the OSA group were more than 6, 3 and 9 times higher, respectively, than in the non-OSA group. To the best of our knowledge, the present study is the first to assess the risk of specific peripheral vestibular disorders in individuals with OSA using a population database. The results support a positive association between OSA and risk of peripheral vertigo.
OSA is a very common sleep-related breathing disorder characterized by recurrent episodes of hypoxia and reoxygenation. Chronic exposure to intermittent hypoxia and the resulting activation of the sympathetic nervous system contribute to damage to the systemic cardiovascular and endocrine systems [5]. The peripheral vestibular system may also be affected by hypoxia and the endothelial changes [4, 35]. Previous literature showed that poor sleep quality in OSA was also associated with vertigo [15, 33]. In a population study using the National Health Insurance Research Database of Taiwan, people with sleep apnea had a significantly higher cumulative incidence of vertiginous syndromes (code 386 in the ICD-9-CM system; includes peripheral vertigo, Meniere’s disease, labyrinthitis, labyrinthine fistula, vertigo due to central origin) than those without sleep apnea (HR = 1.71) [29]. In our study, the diagnostic codes were narrowed to specific peripheral vestibular disorders including BPPV, Meniere’s disease, vestibular neuritis, and other peripheral vestibulopathy. As a result, the hazard of developing peripheral vertigo was notably higher in people with OSA (HR = 6.64) and in females (HR = 1.92).
One of the hypotheses explaining the general effects of OSA on peripheral vestibular function is nocturnal cerebral ischemia. In OSA, cerebral blood flow increases and decreases along with concomitant changes of arterial pressure during repetitive apnea [3, 30]. Due to the rapid changes of blood pressure and flow, it is difficult for the cerebral autoregulation system to avoid cerebral ischemia. As the inner ear structure is supplied by terminal branches of the anterior inferior cerebellar artery without collateral circulations, the vestibular end-organs would be particularly vulnerable to circulatory alternations causing tissue ischemia. With regard to BPPV, previous literatures have been suggested that vascular insufficiency of the inner ear is a possible cause [11, 34]. Periodic experimental hypoxic stress in marine vertebrates has been reported to significantly alter the chemical composition of the otolith [23]. Since otolith homeostasis is maintained by the balanced production of reactive oxygen species by NADPH oxidase-3 (NOX3), it is possible that dysregulation of NOX3 in response to ischemia-reperfusion leads to defective otoconial homeostasis which may cause otolith to be easily dislodged [16, 21]. In Meniere’s disease, a histopathologic temporal bone study showed that a circulatory disturbance may be the cause of abnormal endolymph homeostasis [12, 27]. As the volume of endolymphatic fluid increases, the cochlear lateral wall containing capillary networks is compressed against the bony labyrinth, and the increased cochlear outflow resistance may lead to ischemia-reperfusion injury. For this reason, subjects with preexisting problems of microvasculature could be susceptible to inner ear damage caused by endolymphatic hydrops [7]. In addition, a clinical study revealed that OSA patients with Meniere’s disease benefited from solitary continuous positive airway pressure therapy for managing vertigo and hearing loss [24]. In vestibular neuritis, although the etiology of acute unilateral peripheral vestibular deficit still remains unclear, it could be suggested that the chronically repeated hypoxic episodes would affect the neuronal activities of the vestibular nucleus [35] as well as immune responses to herpes virus [36].
The prevalence of peripheral vestibular disorders is known to be higher in women than in men [9]. In our study, as expected, the incidence was higher in females than in males for BPPV, Meniere’s disease, and vestibular neuritis (Tables 2, 4). The multivariable analysis showed that women had 1.92 times the hazards of developing peripheral vestibular disorders compared to men. The ratio of incidence rate between the OSA and non-OSA cohorts, however, did not meaningfully differ according to gender, meaning that effect of OSA on the incidence of peripheral vestibular disorder would be similar for both women and men.
The strength of this study is that it is a nationwide population-based cohort study that careful excluded possible confounding risk factors for peripheral vestibular disorders and built a control cohort strictly matched for socio-economic factors and comorbidity index. However, this study also has several limitations. First, we used diagnostic codes in administrative claims data. Although medical accessibility in South Korea is excellent [25], people who were unaware of their sleep problems or not willing to visit hospitals could not be included in the analysis. Also, vestibular migraine was not evaluated not only because it tends to be the result of central rather than peripheral pathology but also because the ICD-10 system did not designate a separate diagnostic code for it. In addition, issue of diagnostic accuracy inevitably follows, which is thought to have little impact on the reliability of the comparison results, as this can occur with similar trends in both the OSA and matched comparison groups. Second, the claims data did not include any relevant information about the severity of OSA, polysomnography results and whether subjects had been treated properly. Finally, individuals with OSA who were followed by otorhinolaryngologists or neurologists were more likely to be diagnosed when they developed dizziness. Although there are limitations, the higher incidence of peripheral vertigo in individuals with OSA was consistently observed, with a more than six-fold increased risk, and further studies are needed to follow. We expect that large-scale prospective clinical studies will provide further insights into the causal relationship between OSA and peripheral vertigo in the future.
Conclusion
In this population-based cohort study using nationwide administrative claims data, people with a diagnosis of OSA had a higher incidence of peripheral vestibular disorders, including BPPV, Meniere’s disease, and vestibular neuritis, than socio-demographically matched people who had never been diagnosed with OSA. It is recommended to consider peripheral vertigo when counseling and managing OSA.
Footnotes
Acknowledgments
None.
The Disclosure Statement
Authorship contribution
All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Jae Ho Chung: study design, interpretation of data and revise the draft.
Hayoung Byun: writing the first draft of manuscript, interpretation of the results and study design.
Seung Hwan Lee: study design and interpretation of data.
Jin Hyeok Jeong: study design and interpretation of data.
Jiin Ryu: data analysis, interpretating results and drawing figures.