
Abstract
BACKGROUND:
fHIT is an easily applicable test battery that indirectly evaluates the vestibulo-ocular reflex (VOR) from a functional perspective.
AIMS/OBJECTIVES:
The aim of this study was to Individuals determine the correlation between age and the percentage of correct answers (%CA) obtained in the functional head impulse test (fHIT) in healthy individuals.
MATERIAL AND METHODS:
A total of 105 volunteers, 50 males and 55 females, between the ages of 18 and 70 years, participated in the study. A Beon Solution fHIT system (Zero Branco (TV), Italy) was used in the study.
RESULTS:
In our study, a decrease in the mean %CA was observed in all semicircular canals (SCCs) with increasing age. Between age and mean %CA, a significant negative moderate (–0.311) correlation was observed in lateral SCCs, and a significant negative low (–0.257) correlation was observed in posterior SCCs (p < 0.05). In anterior SCCs, there was no statistically significant relationship between age and mean %CA (p > 0.05).
CONCLUSIONS:
The present study performed in a healthy population will be helpful in terms of making comparisons in studies to be conducted in various vestibular diseases. It will also be a guide for identifying pathological consequences in vestibular diseases.
Introduction
There are various test batteries that evaluate the vestibular system. Although the pathology in vestibulo-ocular reflex (VOR) arch can be detected with the available vestibular tests, we may not obtain complete information about the functional task of this reflex in the frequency range of our movements during daily life activities. Even if VOR gain is normal, blurred vision may occur with head movement. Due to insufficient visual processing (slower visual processing speed or decreased retinal deviation), a sufficient time for optimum visual stabilization may not be attained during head impulse [8, 12]. Visual stabilization is achieved through a complex combination of eye movements that consist of an optimal balance between head position and head velocity compensation at any moment of head movement [36]. Therefore, in testing the functional effectiveness of VOR for head impulses, vHIT may be insufficient, which necessitated the research for alternative measurement techniques to evaluate the effectiveness of VOR in clear vision. There are 2 test methods that evaluate the functional performance of VOR: Dynamic Visual Acuity (DVAT) and functional head impulse test (fHIT).
fHIT was developed by taking the VOR function as a goal and addressing the limitations of other tests [6, 52]. The fHIT with its fast and simple application technique evaluates the rotational VOR in terms of functional performance at high speed and acceleration by focusing on the gaze stabilization ability. The test consists of a system in which the gyroscope is attached on the forehead with a rubber band. The gyroscope has the ability to measure acceleration in 3 planes. Therefore, VOR function can be evaluated in six SCCs. Via fHIT, the person’s ability to read the optotype displayed on the computer screen during the rotational movement of the head is measured. It is a system where the direction of the Landolt C optotype is rotated randomly. Static visual acuity (SVA) is measured first. After determining the SVA, the minimum threshold value obtained is increased by 0.6 LogMAR (log of the Minimum Angle of Resolution) to the level that the person can see most comfortably. The percentage of correct answers (%CA) is calculated by determining the amount of correct answer for the optotypes shown on the screen. The head impulses performed in each SCC plane involve different accelerations in the range of 1000–7000 °/s2head acceleration. The difference of fHIT from vHIT and videonystagmography (VNG) is that fHIT does not measure eye movements, but measures VOR function indirectly, so fHIT is a perceptual test with this feature. [6, 52].
In the temporal bone anatomical examination performed in 150 individuals in an age range 0–97 years, otoconia, sensory neuroepithelium, Scarpa’s ganglion, vestibular nerve, vestibular nuclei, and Purkinje cells in the cerebellum were reported histologically as signs of degeneration in the vestibular system [21]. Changes in vestibular cells have also been indirectly demonstrated by vestibular test batteries measuring VOR. In studies using the caloric test, no age-related changes were observed in caloric test results [26, 57]. In another study, healthy individuals aged 7–81 years were assessed with the sinusoidal rotation test and caloric test, and sinusoidal test results showed a decrease in response amplitude and less decrease in response phase compensation with increasing age, while no change with age was observed in caloric test results [38]. In a study conducted with vHIT, a gradual decrease in VOR gain was observed in young individuals as the speed of impulse increased [29]. In studies investigating the relationship between dynamic visual acuity (DVA) and age; DVAT scores were found to be significantly correlated with increasing age [19, 54].
There is no study examining the relationship of the fHIT with age in a healthy population. In our study, we aimed to determine the relationship between fHIT values and age in healthy individuals.
Material and method
This study was approved by a local university medical and health sciences research board and non-Invasive clinical research ethics committee, Date: 11/12/2019 and #19/26 (Project No: KA19/384). Each participant was informed about the study and signed an informed consent form. The study was conducted at a local university hospital, neurotology department.
The sample size of this study was determined by power analysis. A total of 110 healthy individuals, including 53 males and 57 females, between the ages of 18 and 70 years, participated in the study. Three males and two females were excluded from the study because they could not adapt to the fHIT assessment. In total, 105 individuals, 50 men and 55 women, were included in analyses (Table 1).
Descriptive data about participants
Descriptive data about participants
The inclusion criteria were being in the age range of 18–70 years, having results in normal range from pure-tone audiometry, air- and bone-conduction audiometry, and acoustic immittance measurement, and having normal cognitive function based on the Standardized Mini-Mental State Examination (SMMSE). Then, they were examined by an ENT specialist. Spontaneous nystagmus, cerebellar tests, positional tests, and walk test were performed after detailed anamnesis taken to rule out vestibular system pathology. fHIT was administered in individuals who met the inclusion criteria. The exclusion criteria were having psychological or neurological condition that would interfere with participation in the study; having a history of dizziness; having a history of motion sickness; having a history of a head injury/ear surgery; and, the presence of a cervical pathology or visual impairment. No imaging method was used. In addition, they were asked not to drink alcohol and use any drugs, unless medically compulsory, no later than 48 hours before the test day.
A Beon Solution fHIT (Zero Branco (TV), Italy) system was used in our study. The individual sits on a chair 1.5-meter away from the computer monitor. The test begins by measuring the SVA, which is primarily evaluated using an eye chart shown on the monitor. The assessment is attained by showing letter sizes scaled according to the individual’s viewing distance. The test starts when the individual sees a white spot in the middle of the screen. Then the Landolt C character is displayed where the white point is on the screen.
At this stage, the individual is asked to adjust the white dot until it is large enough for the Landolt C character to be visible. The Landolt C character is then displayed on the screen in 8 different orientations. The individual is asked to tell the direction of the character by pressing the keys on the numeric keyboard. The Visual Acuity Test is terminated when the individual cannot determine the direction of the fifth third of the Landolt C characters on the screen or when all the characters were identified correctly. At the end of this test, the visual acuity level of the individual is recorded. In the next step, the sensor is attached to the individual’s head with an elastic band. During the test, the patient is held by his/her chin by the tester. During the test, it is avoided to touch the sensor. With the correct adjustment of the sensor, graphs including the gyroscope’s speed and angular acceleration are displayed on the screen. After this stage, the SCC pair to be evaluated is determined. After the calibration is done for the determined SCC, the patient’s head is positioned in accordance with the position of the evaluated SCC pair. Before the test, the individual is asked to leave their neck and head free. They are asked not to take their gaze away from the target during the impulses. For lateral SCCs, the head of the individual is positioned in a flexion position of 30°, and impulses are made in accordance with the head acceleration range of 1000–7000 °/s2 (10°–20°).
After the evaluation of the lateral SCCs, RALP (right anterior-left posterior) and LARP (left anterior-right posterior) tests are performed. The important point here is to bring the SCC to the anatomically appropriate position and then performed the impulses. In our study, we positioned the chair to the right at an angle of 45° to the screen for the RALP test. Then, we performed the impulse to the left (towards the screen) 45°, keeping the angular position of the head (in the RALP plane). For the LARP test, the chair was positioned to the left at an angle of 45° to the screen. Then we performed the impulse to the right (towards the screen) 45°, keeping the angular position of the head (in the LARP plane). In this test, the same test method we used in visual acuity test was employed. The individual is told to identify the orientation of the Landolt C character that appears on the screen by pressing the relevant numbers while keeping eyes on the white dot and making an impulse movement is made on the head. The Landolt C character is displayed as the individual’s head is moved. The percentage of correct answers (%CA) is calculated by determining the number of correct answers in the identification of the optotypes shown on the screen. The fHIT device calculates the mean %CA in the acceleration range of 4000–6000°/s2 for lateral SCCs and 3000–6000°/s2 for vertical SCCs. Since we wanted to see the values in all head accelerations in our study, at least 2 swings were performed in each head acceleration (1000–2000–3000–4000–5000–6000–7000°/s2) (Figs. 1–3).

fHIT lateral SCC analysis output.
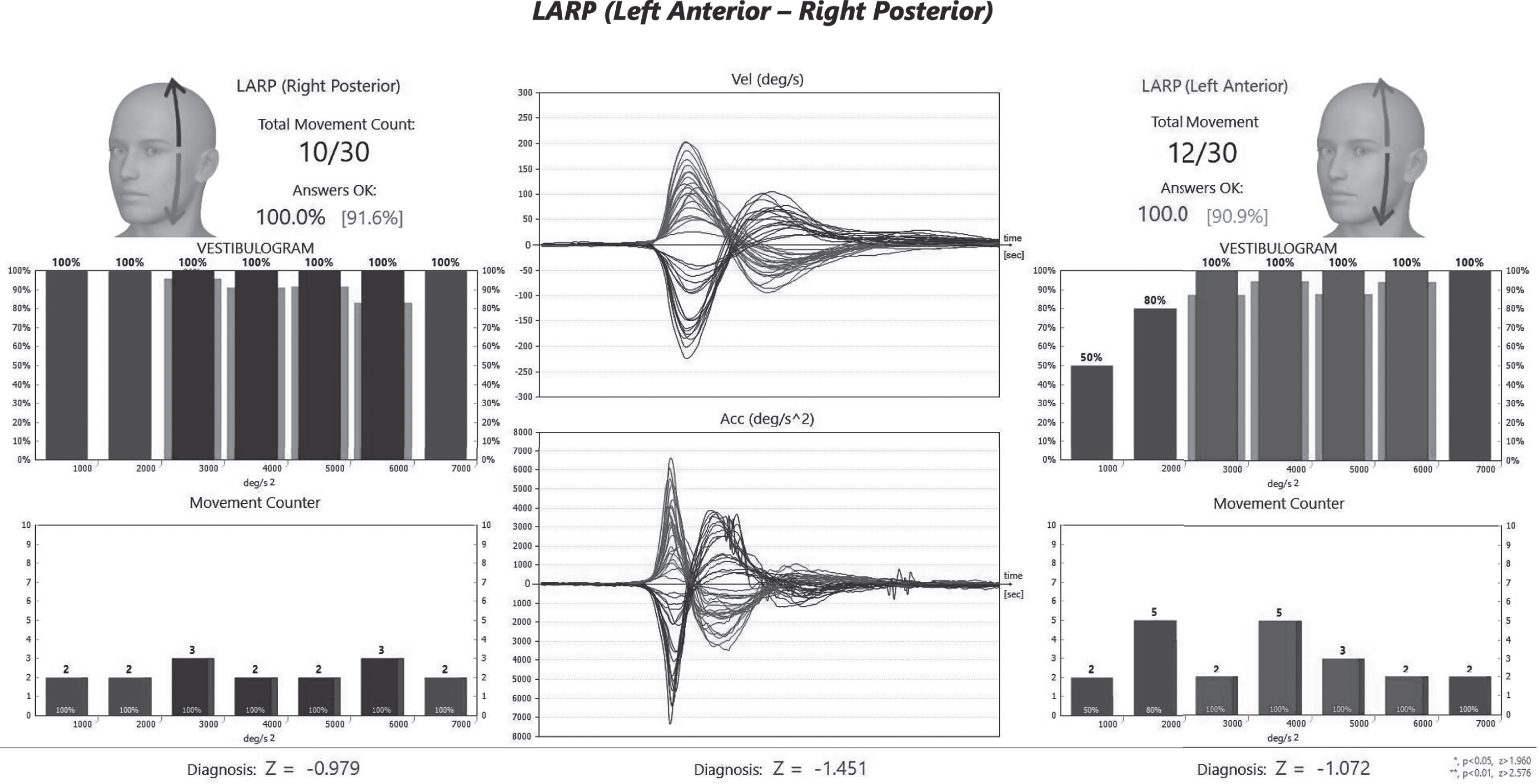
fHIT LARP SCC analysis output.
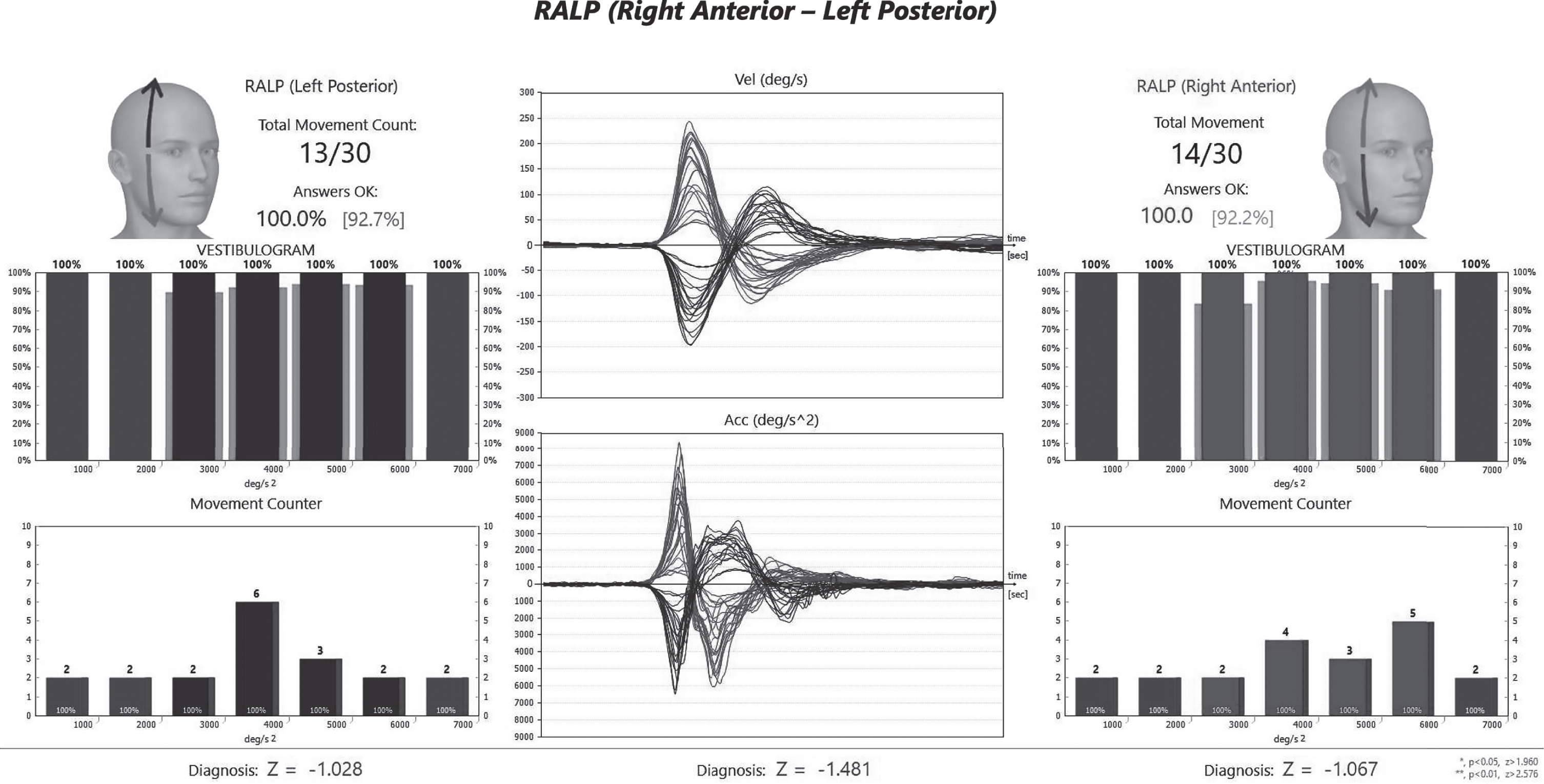
fHIT RALP SCC analysis output.
SPSS (Statistical Program in Social Sciences) 25 was used for the analysis of the data. Normal distribution tests were checked with the Kolmogorov Smirnov Test. The significance level (p) was set as 0.05 for the comparison tests. Comparisons between groups were performed by ANOVA. Variance homogeneity was checked by the Levene test (p > 0.05). Since variance homogeneity was not provided, Tamhane’s T2 test was performed with in-group comparisons. Pearson Correlation Coefficient, “Point-Double-Series Correlation value was used to check the relationship between measurement values, and η (Eta) statistic was calculated.
Results
Relationships of age groups and sex with mean correct response rate (%CA) in SCCs
No statistically significant relationship was observed between sex and mean %CA in SCCs (p > 0.05) (Table 2).
Relationships of age groups and sex with mean %CA in SCCs
Relationships of age groups and sex with mean %CA in SCCs
*p < 0.05; There is a statistically significant relationship, °/s2(degree/second square).
A statistically significant relationship was found between age and the mean %CA obtained from lateral and posterior SCCs (p < 0.05). However, no statistically significant relationship was found between age and the mean %CA obtained from anterior SCCs (p > 0.05) (Table 3).
Correlation coefficients in SSCs by age variable
Correlation coefficients in SSCs by age variable
r; Pearson correlation coefficient, *p < 0.05 there is a correlation between variables.
A statistically significant difference was found between the mean %CA obtained in lateral, anterior, and posterior SCCs and age groups (18–35 years, 36–54 years, and 55–70 years) (p < 0.05, Table 4).
Comparison of mean %CA in SCC by age groups
Comparison of mean %CA in SCC by age groups
*p < 0.05 a statistically significant difference between groups, a; ANOVA test result F test value, SD; standard deviation, °/s2(degree/second square).
As variances were not homogeneous (p < 0.05, Table 5), in determining which age groups were different, Tamhane’s T2 Test was used for paired comparisons within groups.
Results of in-group paired comparisons according to age per canals
*p < 0.05; There is a statistically significant difference between groups, °/s2(degree/second square).
The higher mean %CA in the 18–35 age group compared to the mean %CA in the 55–70 age group was statistically significant only in the lateral canal (p < 0.05, Table 5). Mean %CA in the 36–54 age group was statistically higher than the mean %CA in the 55–70 age group only in the lateral, anterior, and posterior canals (p < 0.05, Table 5).
The graph shows the %CA distributions of the participants in the lateral, anterior and posterior SSKs in 1000 °/s2, 2000 °/s2, 3000 °/s2, 4000 °/s2, 5000 °/s2, 6000 °/s2ve 7000 °/s2 head accelerations (Table 6).
Mean %CA by head acceleration
Mean %CA by head acceleration
SD; standard deviation, °/s2(degree/second square).
In Table 7 and 8 are given the comparison of %CA according to age groups and head accelarations (Table 7, 8).
Comparison of %CA in SCCs according to age groups and head accelerations
Comparison of %CA in SCCs according to age groups and head accelerations
*p < 0.05 There is a statistically significant difference between groups, a; ANOVA test result F test value, SD; standard deviation, °/s2(degree/second square).
Pairwise comparison of groups differing in ANOVA test results
*p < 0.05; There is a statistically significant difference between the groups.
The mean %CA of the right and left ear lateral, anterior, and posterior SCCs are given in Fig. 4.

Mean %CA of the right and left ear lateral, anterior, and posterior SCCs.
The average numbers of head impulses in all head accelerations in lateral, anterior, and posterior SCCs (1000°/s2–7000°/s2) in the right and left ear are given in Table 9.
The mean number of head impulses in each head acceleration rate in lateral, anterior, and posterior SCC
The mean number of head impulses in each head acceleration rate in lateral, anterior, and posterior SCC
SD; standard deviation, °/s2(degree/second square).
The HIT, one of the methods used in the evaluation of vestibular functions, was first used by Halmagy and Curthoys in 1988 [18]. The fHIT is a new test battery based on the HIT mechanism, and covers the acceleration range of our movements during daily life activities, and evaluating the vestibular system functionally. There is no study examining the relationship of the fHIT with age in a healthy population. In our study, we aimed to determine the relationship between fHIT values and age in healthy individuals.
There are several studies reporting the loss of vestibular receptor cells and primary afferents with increasing age [2–4, 41]. There are many receptors in SCCs in healthy adult individuals. The number of receptors decrease with increasing age [34, 40]. VOR is predicted to decrease with the loss of receptors occurring with age. In fact, while serious functional deficits are expected with the loss of receptors and neural declines, the body tries to adapt to the current situation by developing functional compensation mechanisms [13]. Cerebellum is of great importance at this point. Oculomotor responses are controlled by the cerebellum [43, 44]. Many studies on VOR show that it has an important function by activating the cerebellum compensation mechanism on issues related with age and vision [43, 44]. In our study, the decrease in mean %CA with increasing age was significant, negative, and moderate (–0.311) in lateral SCCs, and significant, negative, and low (–0.257) in posterior SCCs (p < 0.05), and the decrease (–0.180) was not significant in anterior SCCs (p > 0.05).
The HIT evaluates VOR (to which high frequency, short duration rapid impulse movements are applied) with the findings obtained from the eye; and it is based on the observation of open saccades caused by a peripheral disorder in the SCC induced [18]. The HIT evaluates VOR at a higher frequency than the caloric test. However, it is a subjective test because open saccades are determined by the observation of the tester [22]. With the determination of the importance of the HIT in defining vestibular hypofunction, the importance of grading eye movements with mathematical evaluations emerged. However, an important point at this point is the feelings of the patient during daily life activities. Although the vestibular test results of the patient are normal, sometimes the complaints of vestibular complaints can still continue. This can be caused by different disturbances ranging from inadequate visual processing to a sufficiently long period of optimum visual stabilization during head impulse [8, 12]. fHIT is based on the HIT physiology, and it gives us data about whether the individual has complaints during daily life activities. It yields functional outcomes regarding the pathology by calculating the percentage of the individual’s correct identification of the optotype shown in different angular accelerations (1.000–7.000 °/ s2). The fHIT is not a test that measures eye movements, but it is a perceptual test. Since it is a functional test, it focuses on the individuals’ quality of life.
The caloric test, which is one of the tests evaluating VOR in the clinic, is one of the widely used evaluation methods for peripheral vestibular pathologies. However, the caloric test only assesses lateral SCCs in the frequency range of 0.002–0.004 Hz (non-physiological) [37]. In studies conducted with the caloric test, no age-related changes were observed [26, 57]. During daily life activities, SCCs are stimulated with 4000°/s2 stimuli between 0.5–5 kHz frequencies, which are compatible with the stimuli frequency occurring when the person walks and turns their head, in three planes. While head velocity is 550°/s during normal daily life activities, this velocity increases up to 6000°/s when head movement speed increases [48]. Therefore, reliable objective test methods that can test the peripheral vestibular system at a broader frequency of daily living activities were needed. The fHIT is a system based on the %CA of the individual during VOR, in the head acceleration range of 1000–7000°/s2, every thousand intervals. In our study, no statistically significant difference was found between age groups in terms of mean %CA measured at 1000°/s2 and 2000°/s2 values in lateral, anterior, and posterior SCCs (p > 0.05, Table 2). In other words, while the decrease in %CA was found significant with the increase in age at high frequencies (p < 0.05), this decrease was not found significant in low frequencies (p > 0.05). It is considered that the reason for this mismatch may be related to the type of hair cell that is induced, which is named as “cell type theory” or “dual frequency theory”. According to this theory, type I hair cells are associated with irregular afferent fibrils, and type II hair cells are linked with regular afferent fibrils. Irregular afferents encode high frequency and high acceleration head movements, while regular afferents encode low frequency and low acceleration head movements. Specifically, VOR can be primarily driven by regularly firing afferent fibrils when low frequency stimuli are encountered, and by irregular afferents when the organism is subjected to high frequency motion. This ideally makes irregular afferents more sensitive to high speed and accelerated head movements [15, 31].
In a study in which all SCCs were evaluated and VOR gain relationships were evaluated using the vHIT, which included volunteers in the age range of 10–89 years, it was observed that only individuals between the ages of 80–89 had decreased VOR gains [33]. In another study, it was stated that there was no link between age and VOR gain until the age of 70 years, and VOR gain value decreased in the 71–90 age range [29]. In our study, the mean %CA in the 36–54 age group was significantly higher than that in the 55–70 age group in all three SCCs (p < 0.05). Since the fHIT we used in our study includes higher frequencies, we think that one reason for this difference may be due to head impulse velocities. Age-related VOR changes have also been shown in the literature to be associated with head impulse velocity [1, 32]. Studies have shown that linear VOR gain remains constant up to the age of 70 for head impulses of 180–200°/s, up to the age of 79 for impulses of 160–180°/s, and up to the age of 90 for head impulses less than 160°/s [1, 32]. In our study, no statistically significant difference was found between the age groups in terms of mean %CA measured at 1000°/s2 and 2000°/s2 head acceleration in lateral and anterior SCCs (p > 0.05). However, a statistically significant difference was found between the age groups in terms of mean %CA measured at 3000°/s2, 4000°/s2, 5000°/s2, 6000°/s2 and 7000°/s2 (p < 0.05). For posterior SCCs, no statistically significant difference was found between the age groups in terms of mean %CA measured at 1000°/s2, 2000°/s2 and 3000°/s2 head acceleration (p > 0.05). However, in terms of mean %CA measured at 4000°/s2, 5000°/s2, 6000°/s2 and 7000 °/s2, there was a statistically significant difference between age groups 18–35 years, 36–54 years, and 55–70 years (p < 0.05). In addition, since the fHIT we used in our study is a perceptual test, the decrease in %CA was found to be significant with the increase in frequency in earlier ages (55–70 age group) compared to other studies conducted with the vHIT [1, 32]. Low VOR gain decreases visual acuity by causing blurring of the image depending on the stimulus (head speed, stimulus duration, etc.). We believe that the reduction in fHIT scores cannot be attributed solely to a decrease in VOR function and that it is associated with the general physical condition, functional state of the other senses, central nervous system integrity, memory, motor coordination, and cognitive ability, which are associated with a decline with age [14, 56].
In a study comparing vHIT and fHIT results in patients with acute unilateral vestibulopathy, it was shown in both tests that compensation occurred after 3 months of follow-up. The data obtained from the two tests were not correlated with each other. The fHIT detected more abnormalities than the vHIT when comparing patients in the acute phase and 3 months later. The fHIT data may indicate that the VOR is functionally impaired although gain values on the healthy side are close to normal. Compensation mechanisms may result in that gain values improve more than the ability to read while moving [11]. Therefore, the fHIT and vHIT are a complementary method for evaluating vestibular rehabilitation outcomes in vestibular diseases.
Many studies with the DVAT, which is an indirect measure of VOR, have reported a decrease in vestibular function with age [55]. The DVAT, similar to the fHIT, is based on measuring the threshold for the recognition of the optotype that flashes briefly during head movement. Both are an indirect and perceptual measures of vestibular function. The decrease in VOR gain results in a lower DVAT score. This decrease may reflect oculomotor function and cognitive activity as well as VOR function [19, 54].
Guinand et al. used the DVAT test on the treadmill with low speed (maximum 30°/ s) head impulse (about 2 Hz) [17]. The fHIT is a test method that measures faster and higher frequency head movements compared to the DVAT [39, 52]. In a case study with vestibular implantation, DVAT scores and fHIT scores were compared. With vestibular stimulation, a significant improvement was observed in high frequency DVAT [49]. In another study involving 23 bilateral vestibulopathy patients in which the fHIT and DVAT were compared on treadmill, 78% of the patients who received the fHIT showed abnormal results, while 17% of the patients who received the DVAT on treadmill at all speeds showed abnormal results. In addition, the fHIT could be completed by all 23 patients, while 11 patients could not complete the test on the DVAT treadmill. All four patients with abnormal DVAT treadmill results showed abnormal bilateral fHIT results. In this study, obtaining more abnormal results in the fHIT was attributed to several factors [51]. First, the compensation ability is less during the fHIT. When walking on the treadmill, patients can use compensation mechanisms to improve gait or gaze stabilization. Second, unlike passive movement during the fHIT, an active movement is made during the DVAT on treadmill. Passive movements have been shown to be more useful in distinguishing healthy subjects from patients with bilateral vestibular loss [50, 54]. This is because during walking there is an efferent copy of the command that produces the walking motion, which causes patients to anticipate retinal deviation as a result of the head movement [5]. Third is the difference in the stimulus. While fHIT selectively stimulates a SCC plane during passive head movements at high frequencies (> 150°/ s), the DVAT treadmill includes an active motion that stimulates all SCCs and otoliths simultaneously [39], and the frequency of the stimulus depends on walking speed [35]. In this study, they reported that the fHIT may be an appropriate assessment method to measure oscillopsia in patients with bilateral vestibulopathy, and with these features, the fHIT and DVAT treadmill tests could not be used interchangeably, but could be used as a complementary test method [51].
Gaze stabilization exercises are used for VOR adaptation in the vestibular rehabilitation program. These exercises are performed to increase VOR gain, and they provide visual stabilization during active and passive head movements. This dynamic exercise process is provided by visual inputs. The occipital lobe, midbrain, and cerebellum are active in this process to recalibrate VOR gain [16]. Studies have shown that VOR exercises improve dynamic visual acuity (DVA) [46, 47]. The fHIT may also be used in the future in vestibular rehabilitation patients to measure functional progress of exercises. It can also be used as a guide for the rehabilitation program with its feature of detecting the head acceleration in which the individual experience functional disability.
Based on our experience, manual impulses on the device can be difficult to perform. It is not always possible to achieve the desired target head acceleration. Only a very experienced practitioner can achieve the desired target impulse momentum. The test taker’s dominancy (right or left hand) and the difference in muscle strength in the right or left arm can also affect the test results. For this reason, a mechanical system can be added to the device to allow impulses for each thousand head acceleration. There exists no study regarding hand dominancy in the vHIT and fHIT. Matino-Soler et al. stated that leftward impulses cause higher acceleration, which may be related to using the right hand dominantly [29].
There is only one study in the literature that presents the mean the number of head impluses in each head acceleration [45]. However, our study is more inclusive in this regard, as the participants of that study consisted of only athletes. We believe that our study will guide future studies in this regard.
One of the limitations of our study was that those who were over 65 years old could not be included in the study because of Covid-19 related risks. Covid-19 was first seen in China in 2019, and cases have been seen in our country since March 2020. Since being over the age of 65 is a transmission risk factor for COVID-19, some restrictions have been made for individuals over the age of 65 in Turkey. For this reason, in our study, which we started on December 11, 2019, we could not include any individual over the age of 65 after March 15, 2020. In this time period, we were able to include only six individuals over 65 years of age who met our inclusion criteria. Another of our limitations was the laboratory tests that we did not add to the inclusion criteria (such as vHIT, caloric test, cVEMP and oVEMP). This may indicate the possibility of an asymptomatic vestibular deficit in the study population.
In vestibular studies showing the relationship with age in the literature, comparisons have been made in different age groups [10, 42]. According to the classification of the World Health Organization, young individuals are between the ages of 18–65. There is no subclassification for standardization in the normalization studies of vestibular tests in this age range. The vast majority of individuals in our study were also in this range. For this reason, we made statistical evaluations by dividing the participants into approximately 3 equal divisions, since we wanted to see the group distinction of the differences between the ages of 18–70 in our study. In future studies, we plan to investigate fHIT, which evaluates VOR in terms of functionality, by dividing the participants into smaller age ranges with larger populations in this age group.
The fHIT device, whose mechanism is based on indirect measurement of VOR functionality over VOR gain, helps us to obtain faster and safer results in the diagnosis and rehabilitation processes when combined with other test batteries. In our study, in which the relationship of fHIT values with age was evaluated, a decrease was observed in mean %CA, which functionally reflects VOR, with the increase in age in all SCCs. This study will also be a guide in terms of making comparisons and determining pathological results in studies to be carried out in various patient groups in a healthy population.
By adapting the fHIT to rehabilitation programs, daily life activities of individuals with vertigo and their quality of life can be improved. By adding a mechanical system allowing impulses at the desired acceleration, errors that may arise from manual impulses in the test can be minimized. In the fHIT, the effect of using the right or left hand dominantly on test results can be investigated in future studies. In addition to the gyroscope mechanism, a vestibular system evaluation test battery can be developed in which saccades and functional evaluation are performed together by adding goggles as in the vHIT system.
Conclusion
There is no study that evaluates the relationship of functional head impulse test device with age in a healthy population. In our study, we aimed to determine the relationship between fHIT values and age in healthy individuals. The present study performed in a healthy population will be helpful in terms of making comparisons in studies to be conducted in various vestibular diseases. It will also be a guide for identifying pathological consequences in vestibular diseases.
Footnotes
Acknowledgments
The authors are grateful to all participants in this study.
Disclosure statement
No potential conflict of interest was reported by the authors.