
Abstract
BACKGROUND:
The mastoid vibration (MV) has been used to investigate unilateral vestibular dysfunction by inducing nystagmus. Additionally, this MV can be used to quantify the effect of deterioration by aging on the vestibular system during walking. Could such MV be used to assess the uni/bilateral vestibular deterioration by aging during standing?
OBJECTIVE:
This study attempted to determine the feasibility of using MV for identifying the uni/bilateral vestibular deterioration by aging during standing.
METHODS:
Fifteen young and ten old adults’ balance control patterns were assessed by three random MV conditions: 1) No MV; 2) Unilateral MV; 3) Bilateral MV. The dependent variables were the 95% confidence ellipse areas and the sample entropy values, which were calculated based on the center of gravity displacement within each condition.
RESULTS:
Significant main effects of MV and aging were found on all outcome variables. A significant interaction between aging and different MV types was observed in the 95% confidence ellipse area (p = 0.002) and the length of the short axis (anterior-posterior direction, p = 0.001).
CONCLUSIONS:
We concluded that the MV could be used to identify different vestibular dysfunctions, specifically in old adults.
Introduction
Maintaining a successful standing balance essentially depends on the somatosensory system, the vestibular system, and the visual system. Specifically, it has been suggested that when standing on a firm surface, 20% of balance control attributes to the vestibular system [32]. Additionally, when standing on an oscillated surface, the contribution of the vestibular system for balance control increases to 70% through sensory recalibration [32]. This result points out the importance of the vestibular system, particularly when other sensory systems become unreliable. It is worth mentioning that the vestibular system dysfunction on the unilateral or bilateral side leads to different patterns of visual control for self-spatial orientation [19, 21]. For instance, for patients with the chronic unilateral vestibular dysfunction (UVD), an increased visual-shift-angle towards the ipsilateral-lesioned side (deficits of spatial orientation) in the subjective visual vertical and horizontal tests was observed [21]; however, such a result is not found in patients with the bilateral vestibular dysfunction (BVD) [19], probably due to symmetrical loss of vestibular inputs. This finding suggests that spatial orientation deficits in patients with BVD are not a simple sum of the effects of two UVDs.
Similar phenomena are observed when using objective measures, such as the body sway measures in BVD and UVD [5, 25]. A study shows that patients with BVD increase their body sway than healthy subjects even when simply standing on a fixed platform with eye-opened condition [25]. However, for patients with UVD, the significant increment of balance sway is only observed when other sensory systems are perturbed [33]. These phenomena can be explained by a Bayesian model, which describes that the reduced accuracy of sensory signals resulting from internal or external perturbations may lead to a more imprecise postural estimation and subsequently reduces the accuracy of postural correction [39]. However, the abovementioned studies only focus on chronic patients with UVD and BVD.
To investigate the effect of the acute unilateral vestibular dysfunction on balance control during standing, the bilateral bipolar galvanic vestibular stimulation (GVS) has been widely used [11]. This GVS technique is based on delivering the current (∼1 mA) with an anodal electrode on the mastoid process behind one ear and a cathodal electrode behind the other ear. When applying this kind of GVS on a human during standing, the significantly medial-lateral body sway toward to anode side is observed because the GVS evokes an automated response to stabilize the head [43]. However, for understanding the effect of the acute bilateral vestibular system on balance control, the bilateral monopolar GVS with electrodes of the same polarity at both sides of the mastoid process needs to be used. When each side of the vestibular system is perturbed simultaneously, the significant body tilt in the anterior-posterior direction is observed [6].
Nevertheless, applying the GVS on the mastoid process has inevitable side effects: skin irritations, burns, and discomfort pain underneath and around the stimulus electrodes [42]. Moreover, using GVS through experimental trials increases the level of anxiety even in the one data collection [30]. These side effects could bias the outcomes [34]. Therefore, there is a need to find a validated replacement to assess and evaluate the function of the vestibular system during standing.
Many studies have shown the feasibility of using mechanical mastoid process vibration (MV) to diagnose patients with a unilateral vestibular loss [14–17, 44] but not patients with bilateral vestibular loss. This technique induces instantaneous horizontal nystagmus, an indicator of asymmetry of vestibular function and the side of the vestibular loss when patients sit on the chair. To assess the uni/bilateral vestibular functions during walking, our previous studies showed that applying MV made the patterns of dynamic postural control more irregular when either unilateral or bilateral vibrations were activated in comparison with the control condition, particularly in the anterior-posterior direction in both young [7] and old adults [8]. Notably, when vibration was activated on bilateral sides, the dynamic postural control became even more irregular than when vibration was activated on the unilateral side in both young and old adults. Besides, no participants complained of the sensation of itch, burns, or pain. These results suggested that 1) the usability of the mechanical vibrations, as a replacement of GVS, for determining the function of the vestibular system between different age groups, and 2) the patterns of dynamic postural control were different when the unilateral or bilateral function of the vestibular system was perturbed. Could such mastoid vibration be used to identify the uni/bilateral vestibular dysfunctions during standing?
One of the most common techniques to measure standing balance control is to measure the center of gravity displacement (CoG, the center of gravity is an imaginary point at which body weight is evenly dispersed) [5]. In order to quantify the CoG displacement, one of the effective methods is to calculate the 95% confidence ellipse area, which encloses approximately 95% of the CoG points during each standing trial [40]. A larger 95% confidence ellipse area represents worse balance control. However, 95% of the CoG confidence ellipse area can only represent overall (the amount) performance in a certain period but can’t tell the CoG displacement changes with time series. More recently, increasing evidence has found that investigating the motions through time series can detect subtle changes, which traditional measures, such as CoG displacement, can’t find [26]. Using the entropy to assess the regularity/predictability with CoG time series is one of many ways to understand the balance control in time series [26]. A regular pattern of CoG movement represents a more predictable pattern and produces lower entropy values and vice versa. For instance, higher entropy values (irregular movement) during standing have been observed in old adults [20], in old fallers [20], in patients with concussion [36], in patients with stroke [31], and in patients with Parkinson’s disease [29] in comparison with controls.
To answer the abovementioned essential research questions, the attempts of this study were 1) to determine the patterns of balance control under uni/bilateral vestibular vibrations, and 2) to identify the balance control by using the traditional measures (95% of ellipse area) and the time series measure (sample entropy). We hypothesized that the MV could lead to different balance control patterns by acutely producing uni- and bilateral vestibular perturbations, particularly in old adults.
Methods
Participants
Fifteen young and ten old adults (Table 1) participated in this study. Participants were free from any musculoskeletal impairments and had no history of extremity injuries that may have affected their gait. Also, all participants needed to obtain a zero score in the dizziness handicap inventory to participate in this study. This study was carried out in accordance with the relevant guidelines and regulations of and upon approval by the University of Nebraska Medical Center Institutional Review Board (IRB# 340–10-FB). Informed consent was obtained from all participants before the experiments began.
Participant demographics: means (standard deviation)
Participant demographics: means (standard deviation)
A Balance Master System 8.4 (NeuroCom International Clackamas, OR, USA) was used to measure the pattern of balance control. Two 22.9×45.7 cm force plates were used to record the center of gravity’s movement at 100 Hz sample frequency. Foot placement was standardized based on participants’ height, according to manufactory guidelines. Mastoid vibration (MV) was generated by a mechanical vibrotactile stimulus using two electromechanical vibrotactile transducers (tactors; Engineering Acoustics, FL, USA.) that were placed on the mastoid processes bilaterally (Fig. 1).

The tactors and control unit. The tactors were fasten on each mastoid process and the frequency and amplitude of vibration was controlled by control unit. The control unit was controlled by laptop wirelessly.
These tactors are designed for mounting within a seat or cushion and can produce high force and displacement levels that allow the vibration to be easily felt even through layers of padding. The tactors were connected to controllers, and they provided optimal efficiency of vibration at low frequencies (50–140 Hz). They had a diameter of 4.8 cm and a thickness of 1.9 cm. The frequency and amplitude of the stimulation were communicated wirelessly from a computer to the tactor controller unit, which transmitted the signals through cables to the tactors. The frequency and amplitude of MV were set to 100 Hz and 17.5dB, respectively [7, 8]. These specific settings were selected based on examining available literature [7, 8]. Extensive pilot experimentation verified that these settings were the most effective to consistently induce changes in eye movement and sway during standing without producing any discomfort. A pulsed firing pattern with an active period duration of 0.4 s and a resting period duration of 0.6 s was used to prevent saturation of the vestibular sensation [7, 8]. Three conditions of MV were used: unilateral (Uni), bilateral (Bi), or none (No). For unilateral stimulation, the right-side mastoid process was selected for all participants to receive a consistent outcome.
A total of three trials were randomly assigned to participants in one visit. We limited the trials because this study attempted to understand the effect of the acute vestibular stimulus on the patterns of balance control. Therefore, the learning effect from the saturation of mastoid vibration was required to be minimum. The foot placement was determined according to the manufacturer’s instructions with barefoot. Participants were instructed to “standstill as possible as you can.” Each trial lasted 90 seconds. Between the trials, participants had one-minute rest to stretch and relax. A verbal warning command was given to subjects 10 seconds before the initiation of each trial, and another verbal command was given at the trial initiation. After each trial, the participant was asked if they felt an uncomfortable sensation such as flushing, cold sweat, increased salivation, stomach discomfort, nausea, vomiting, dizziness, headache, and drowsiness. The data collection would be stopped if they felt any uncomfortable sensation.
Data processing
All calculation scripts were written in Matlab 2016b code (Mathworks Inc., Natick, Massachusetts).
95% confidence ellipse area [35]
A 95% confidence ellipse area was calculated by the formula below [35]:
Where
Sample entropy [26]
Sample entropy is a measure to evaluate the complexity of a system and is the negative natural logarithm of the conditional probability that two subseries similar for m points remain similar for m + 1: SampEn (m, γ, τ, N), where m is data points length, γ is tolerance, τ is the time delay, and N is a time-series data set of length. First of all, A time-series data set of length N ={ x1, x2, x3 …… x
N
} with a constant time interval τ was taken. Then, the template vector of length m was defined, such that Xm(i) = X1, Xi +1, Xi +2, ... . ... , Xi +m - 1 and the distance function d[Xm(i), Xm(j)]. Therefore,
Statistical analysis
A two-way mixed ANOVA (3 MV conditions×2 age groups) was used to investigate the effect of different types of MVs, the effect of aging, and the interaction between these two effects on each dependent variable. The dependent variables were the 95% confidence ellipse area, the length of the long-axis of 95% ellipse confidence ellipse area, the length of the short-axis of 95% confidence ellipse area, and the sample entropy values of CoG displacement in both anterior-posterior and medial-lateral directions. If there existed an interaction in each dependent variable, post hoc comparisons were performed using the Tukey method for comparing the effect of MV in each age group. Besides, the Tukey-Kramer test was performed in SPSS when the group sizes were unequal, which compared between age groups in each MV condition. The significant level was set at 0.05. Statistical analysis was completed in SPSS 20.0 (IBM Corporation, Armond, NY). To understand the effect size, we used the partial eta squared method as this method is widely used for measuring the effect size, based on Cohen’s guideline 0.138 for a large effect size, 0.059 for a moderate effect size, and 0.01 for a small effect size [9].
Results
No participants reported side-effects as follows: skin irritations, burns, and discomfort pain.
Effect of unilateral or bilateral MV on patterns of balance control (Fig. 2)
A significant effect of MV was found on 95% confidence ellipse area (F2,46 = 15.23, p < 0.0001), the length of short axis (anterior-posterior direction, F2,46 = 20.19, p < 0.0001), the length of long axis (medial-lateral direction, F2,46 = 9.25, p < 0.0001) and the values of Sample Entropy in the anterior-posterior direction (F2,46 = 5.43, p = 0.008). Marginal post hoc comparisons showed that applying Uni-MV and Bi-MV significantly increased the 95% confidence ellipse area (p = 0.0061, p < 0.001 respectively), the length of short axis (p = 0.02, p < 0.001 respectively), the length of long axis (p = 0.01, p = 0.001 respectively), but decreased the value of Sample Entropy in the anterior-posterior direction (p = 0.01, p = 0.001 respectively). More detail was shown in Table 2.
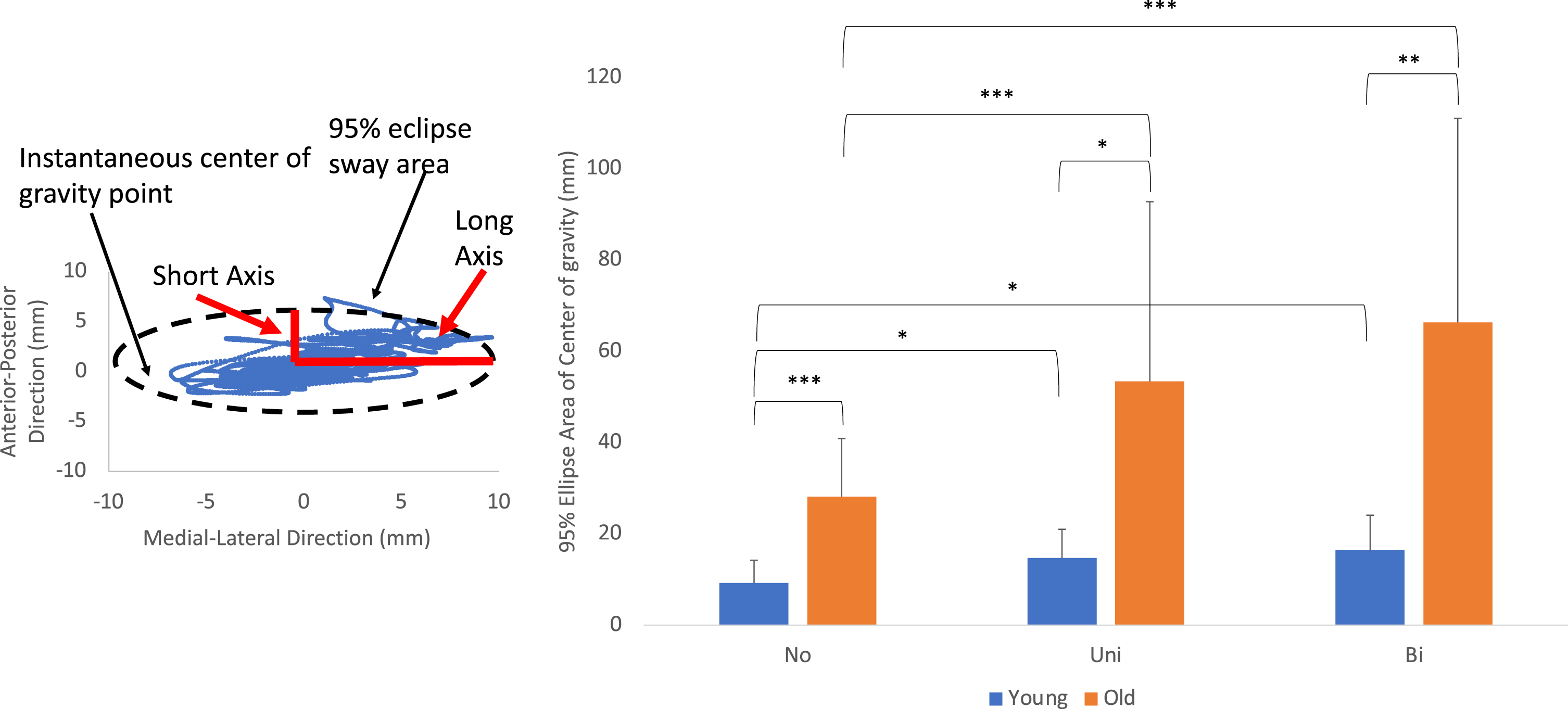
The diagram of a 95% confidence ellipse area.
The pairwise comparisons
No: no mastoid vibration, Uni: unilateral mastoid vibration, Bi: bilateral mastoid vibration, AP –anterior-posterior, ML- medial-lateral, SE- sample entropy values.
A significant effect of aging was found on 95% confidence ellipse area (F1,23 = 64.25, p < 0.0001), the length of short axis (anterior-posterior direction, F1,23 = 149.99, p < 0.0001), the length of long axis (medial-lateral direction, F1,23 = 445.19, p < 0.0001), the values of Sample Entropy in the anterior posterior direction (F1,23 = 129.69, p < 0.0001) and the value of Sample Entropy in the medial-lateral (F1,23 = 123.82, p < 0.0001). More detail was shown in Table 2.
Interaction between the effect of MVs and the effect of aging on patterns of balance control (Fig. 3)
A significant interaction was found in 95% confidence ellipse area (F2,46 = 7.02, p = 0.002), and in the length of short axis (anterior-posterior direction, F2,46 = 8.27, p = 0.001). Post hoc showed that not only both Uni-MV and Bi-MV increased the length of short axis (p = 0.019 in young, p = 0.013 in old; p = 0.024 in young, p = 0.008 in old) but also Bi-MV increases the length of short axis more than the Uni-MV (p = 0.05 in old). More detail was shown in Table 2.
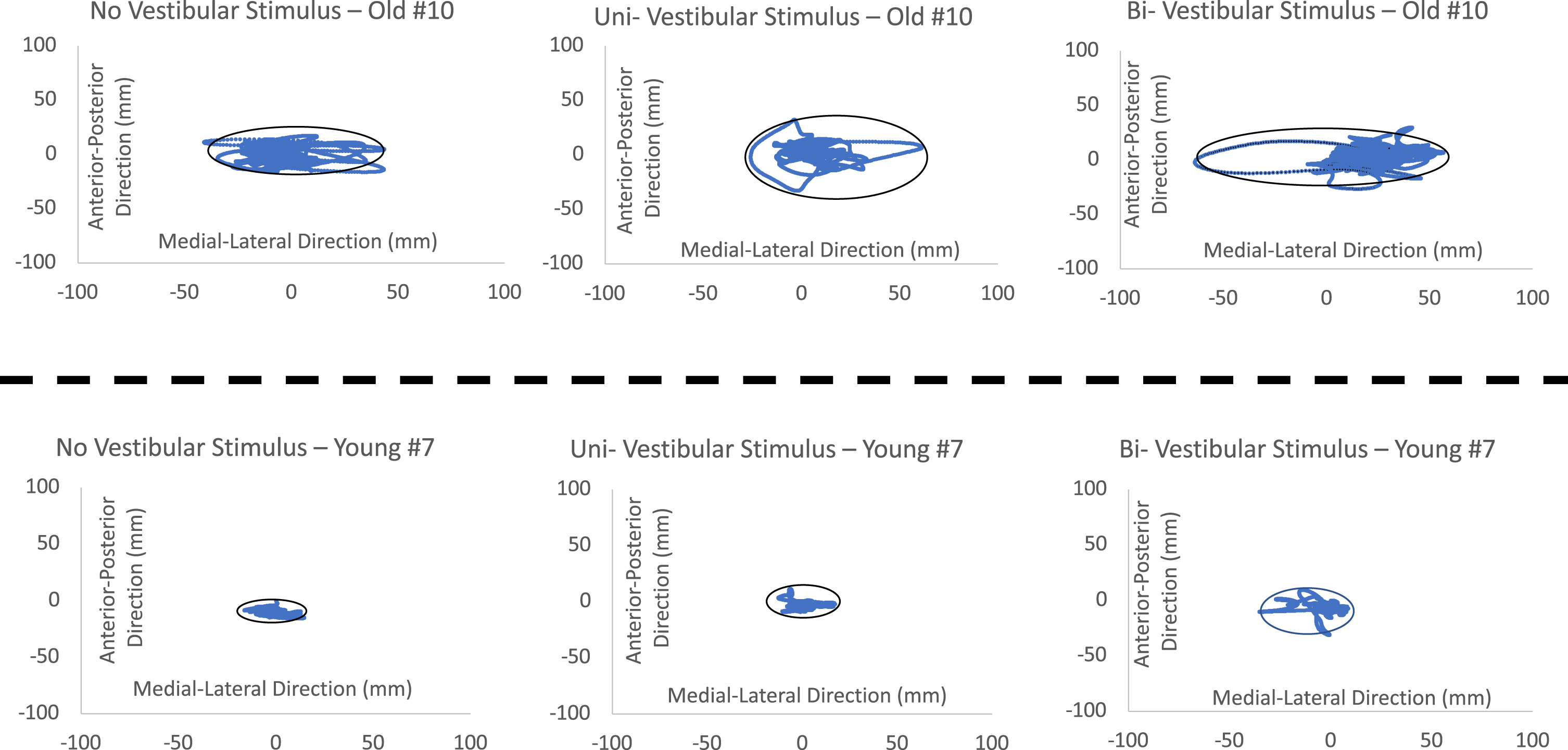
The individual’s representation of the results. The results clearly showed the differences between young and old individual and also demonstrated the differences among different mastoid vibrations.
This study aimed to determine the usability of MV for assessing the acute dysfunction of the vestibular system during standing. The results had an agreement that applying MV indeed could lead to different patterns of balance control by acutely producing uni- and bilateral vestibular perturbations.
Any MV increased the body sway and regularity of balance control
Like other studies, which applied GVS on young and old adults, the increased body sway of balance control was the sign of acute/temporary vestibular dysfunction in the current study. The increased 95% of ellipse area was observed in both young and old adults when either unilateral MV or bilateral MV was given to participants. This result confirmed that the mechanical mastoid vibration indeed could trigger the acute/temporary vestibular dysfunction like other studies. Secondly, these unilateral and bilateral MVs affect balance control patterns in both the anterior-posterior direction and the medial-lateral direction. This unexpected result expressed the fundamental differences between the effect of GVS and the effect of MV on unilateral/bilateral sides. For GVS on the unilateral side, a current passes through the anode side to the cathodal side. This direct electrical stimulus induces out-of-body experiences [23], termed as vestibular illusions. This vestibular illusion leads to spatial disorientation, particularly in the horizontal reference (medial-lateral direction) [43], and this is why humans deviated from the straight pathway but still think they standstill or walk straightly under unilateral GVS [18]. However, for applying unilateral MV, this stimulus majorly activated the proprioceptive afferents from the trapezius and sternocleidomastoid muscles [13, 24]; furthermore, it activated the afferents from semicircular canals and otoliths to induce the rotation sensation [37]. This rotation sensation further increased the body sway in both anterior-posterior and medial-lateral directions, which were observed in this study. Additionally, when applying the bilateral MV on participants, the length of the short-axis (anterior-posterior direction) increased approximately 50% from the control condition (No MV) in all participants. However, the length of the long-axis (medial-lateral direction) only increased by approximately 30% in all participants. Moreover, the effect of bilateral MV on balance control in time series only was observed in the anterior-posterior direction but not in the medial-lateral direction. Two rationales may explain this increment of body sway and irregularity in the anterior-posterior direction: 1) binaural monopolar GVS effect and 2) active lateral control.
Séverac Cauquil et al. [6] applied the binaural monopolar GVS on each mastoid process and showed that it is possible to purely induce a center of pressure deviation in the anterior-posterior direction. They further suggest that central nervous system processing of the GVS-evoked signal depends on the differences between the right and left vestibular inputs. In other words, the head/body movement is tilted or translated based on the differences between the right and left vestibular inputs. Based on this hypothesis, if the amplitude and frequency MV vibrations were given equally on both mastoid processes, the body sway in the medial-lateral possibly was offset, but the body sway in the anterior-posterior direction might be increased doubly. This may be the first explanation for the abovementioned observations in the current study.
It also can be explained by the active lateral control hypothesis [28]. Based on this hypothesis, the balance control is directional dependence. O’Connor and Kuo [28] find higher sensitivity of balance control in the anterior-posterior direction than in the medial-lateral during standing. They explain that the high demand for active control during standing may be due to the configuration of the lower extremity. In the sagittal plane, there is an inverted pendulum needed to be controlled, which is composed of multiple segments, such as hip, knee, ankle, and metatarsophalangeal joints; however, in the frontal plane, a four-bar linkage composed of two legs, pelvis, and ground may need less active control than an inverted pendulum. Therefore, this might be the rationale that less sensory inputs (bilateral vestibular dysfunction) induced more active control in the anterior-posterior than in the medial-lateral direction due to the complex low extremity mechanism in the sagittal plane in the current study.
Surprisingly, the MV decreased the irregularity as aging. This result indicated two-fold rationales as follows: 1) this decreasing irregularity might represent an easier way to maintain balance, and 2) either increasing or decreasing regularity demonstrated the aging strategies for standing. For rationale #1, unlike many studies investing the balance between young and older adults [3, 26], applying MV induced the lower irregularity because it might be the easier way for old adults to maintain balance with the perturbed vestibular system on both sides. It can be explained that when the loss of accurate vestibular information, the easiest way for old adults to do was to attempt to stand as still as possible as they could. In other words, these old adults may sacrifice their degree of freedom (more regular motion) to compensate for the sensory conflict [12]. This phenomenon is also observed when learning a new skill or dealing with a novel situation [27]. For rationale #2, it has been hypothesized that there exists an optimal movement variability in a healthy biological system [41]. Decrease or increase causes movement less adaptable to perturbations (the conflicts of sensory information and the loss of sensory systems) and is associated with unhealthy status [41]. This hypothesis has been supported by that too much, or too little step width variability is associated with a fall history in older adults who walk in normal conditions [4]. Besides, increasing gait variability may not imply impaired stride-to-stride control of walking in healthy older adults [10].
Bilateral MV had a stronger effect than Unilateral MV in old adults
It was not novel that old adults demonstrated more body sway in both the anterior-posterior and medial-lateral directions and more irregular patterns of balance control in comparison with young adults. Apparently, there was a significant difference in the 95% of the ellipse area between young and old adults among three different MV conditions in the present study. Compared with young adults, 95% of ellipse area for old adults was 205% greater in normal standing. Interestingly, this difference was enlarged even more when Uni- and Bilateral MVs were provided in old adults in comparison with young adults, increasing to 263% and 305% respectively. These results might imply that the natural deterioration of the vestibular system by aging leaded the distinct alternations in balance control. Recent epidemiological evidence estimates that approximately 30% of adults above 40 might experience some form of vestibular dysfunction [1]. Specifically, the decreased density of labyrinthine hair cell receptors shortly after 30 years old has been reported, followed by a drastic drop of the vestibular receptor ganglion cells from 55 to 60 years old [2, 38]. By the age of 70, only 60% of vestibular hair and nerve cells remain intact [2, 38]. Another interesting finding was that applying bilateral MVs had a stronger effect on 95% of the ellipse area than applying unilateral MV on balance control in old adults but not in young adults. It might be because, in healthy young adults, the intact visual and somatosensory system might compensate for the acute/temporary dysfunction of the vestibular system unilaterally or even bilaterally. Therefore, there was no difference in balance control between when receiving unilateral and when receiving bilateral MVs in young adults. It might also be explained by the Bayesian hypothesis that less sensory information (deterioration of the visual, somatosensory, and vestibular system by aging) induced increased uncertainty and further increased the body sway.
Limitations and future works
The limitation of this study apparently was the sample size of participants. Therefore, the effect size was calculated by using the partial eta squared method. Partial Eta Squared values for the interaction between aging, and different types of MV were 0.234 in the 95% confidence ellipse area and 0.265 in the length of the short axis, indicating a large effect size. Another limitation was the amplitude and frequency combination of mechanical vibrations. This combination of 100Hz and 17.5dB was suggested by our previous studies [7, 8] and a review in the skull vibration-induced nystagmus test of vestibular function [13]. The future studies should 1) determine how different frequency and amplitude combinations of MV affect the balance control, 2) determine how to balance control would be altered under MV with other sensory perturbations, and 3) applying these MVs to identify the patients with different vestibular disorders because 30% of patients with vestibular symptoms can’t be diagnosed using currently available tests or instruments [1].
Footnotes
Acknowledgments
This study was an extended analysis of Dr. Jung Hung Chien’s doctoral dissertation. All data collections were performed at the Department of Biomechanics at the University of Nebraska Omaha. We sincerely thank the generosity of this Department of Biomechanics for using the equipment.
Author contributions statement
J.C. designed and carried out the experiments. Y.L. and J.C. wrote the main text. Y.L. M.M, N.S. and J.C. reviewed and revised the manuscript.
Competing financial interests
The authors declare no competing financial and non-financial interests. The authors don’t receive any support from organizations that may gain or lose financially through this publication. The authors don’t have any stocks or shares in companies that may gain or lose financially through publication. The authors don’t have the consultation fees or other forms of remuneration from the organization that may gain or lose financially. There were no patents or patent applications. The authors don’t anticipate employment by any organization that may gain or lose financially through this publication. The authors do not have unpaid membership in a government or non-governmental organization, due membership in an advocacy or lobbying organization, or an unpaid advisory position in a commercial organization. The authors are not writing or consulting for an educational organization, or acting as an expert witness.