
Abstract
Background:
Unilateral vestibular hypofunction (UVH) may lead to modifications on metabolism and body composition. Vestibular rehabilitation (VR) demonstrated its effectiveness in ameliorating balance function and several other daily-living aspects.
Objectives:
The aim of this study was to evaluate metabolic composition, by means of bioelectrical impedance analysis (BIA) and daily activity, with the use of a wrist-worn movement tracker, in UVH participants before and after VR, and to compare data with a healthy control group (CG) of adults.
Methods:
46 UVH and 60 CG participants underwent otoneurological testing, self-report and performance questionnaires, BIA, and wore a device tracking daily movement and energy expenditure for one full day; this was performed before and after VR.
Results:
UVH participants demonstrated a significant (p = 0.008) increase in muscle mass after VR, and, when compared to CG, no differences were present with respect to visceral fat and muscle mass. UVH adults reported a significant increase in energy expenditure spent in movement (p = 0.008) and during the day (p = 0.009), daily number of strides (p = 0.009) and calories spent in sweeping (p = 0.009) and stairing (p = 0.008).
Conclusions:
Results from this study show that VR provided an improvement of metabolic function and body composition of people with UVH, possibly by contrasting structural modifications in neural pathways stemming from the vestibular nuclei and connected to autonomous function.
Keywords
Introduction
Although the underlying mechanisms are only partly understood, the vestibular system is known to play a role in the modulation of body composition, as regards fat, bone and muscle [30]. Indeed, recent evidences point to a significant effect on body composition mediated by extensive connections between the vestibular system and brainstem circuitry regulating metabolism, energy homeostasis, feeding behaviour [17] as well as respiration, blood pressure and heart rate, via anatomic projections from vestibular nuclei to brainstem autonomic centers [49]. Experimental evidence for connections between the vestibular and melanocortin system –especially in the context of a deep neuronal rearrangement following vestibular deafferentation –have been further corroborated by clinical experiences. These showed that individuals affected by unilateral vestibular hypofunction (UVH), when compared to healthy controls, demonstrated a significant shift in body composition [36], resting-state and movement energy expenditure, with less time spent upright and a lower walking distance per day, when compared to healthy people [6].
Body composition analysis devices, such as bioelectrical impedance analysis (BIA), are widely used in research settings and also in homecare, to monitor weight loss therapy or the outcome of leisure, strength or endurance exercise [11]. Such devices are cheap, not invasive and easy to use, while capable to offer several outcome parameters [11] and have been demonstrated to be reliable and accurate, especially when equipped with foot-to-hand eight-point tactile electrodes [47]. Moreover, the demand for personal physical activity tracking devices has soared, due to the possibility of an easy assessment of daily living activities. In this light, studies confirmed the reliability of up-to-date wrist-worn physical activity trackers, which rely on multiparametric assessments (accelerometers, photoplethysmography and descending algorithms) and are able to provide a wide variety of daily-living parameters [6, 13].
Vestibular rehabilitation (VR) uses several strategies to enhance neuroplasticity, such as adaptation, habituation, and substitution, with the goal of controlling residual symptoms and improving static and dynamic balance [9]. In the context of UVH, vestibular rehabilitation may also help at reducing comorbid depression and anxiety, thus ameliorating general quality of life. Moreover, it demonstrated effectiveness on multiple vestibular-related domains [9, 32].
If normal vestibular output is not gained back, a persistent shift in metabolic activity could further increase the detrimental impact of UVH to physical performance and quality of life [45]. No study, to now, investigated how VR may impact on body composition, energy expenditure and behavioural changes in daily-living movement, for individuals affected by chronic uncompensated vestibular weakness. The aim of the present study is to evaluate these aspects by using the association of BIA and wrist-worn activity tracking in a group of chronic UVH adults with a body mass index (BMI) lower than 25 [2] before and after a VR protocol and when compared with an equally balanced group of healthy participants, serving as a control group (CG).
Materials and methods
The diagnosis of chronic UVH was achieved by bithermal caloric irrigations, with a reduction in vestibular response of at least 25% on one side when calculated by means of Jongkees’ formula, at least 3 months after the onset of symptoms [4]. A study sample of 51 consecutive participants with a BMI < 25 was enrolled from February 2019 to March 2021. By using a frequency-matching procedure a population of 60 gender- and age-matched healthy subjects serving as control group (CG) were extracted from the institutional database by a biostatistician not involved in the study. Demographic data for both groups, such as age, gender were collected, as well as cause and side of UVH and disease duration (DD, in months) were retrieved for UVH participants. Hearing loss was accounted for in the matching procedure between UVH participants and the CG, according to American Academy of Otolaryngology guidelines [1]. No history of falls or relevant metabolic, cardiac, vascular, rheumatologic, orthopedic, or neurological conditions were recorded in participants’ clinical history charts. Both UVH and CG participants were screened for blood test abnormalities such as evidence of liver or kidney dysfunctions. No participant was pregnant or breastfeeding at the time of data collection. Neurological conditions were excluded by means of the Mini Mental State Examination and brain MRI. Abnormalities possibly causing otoneurological dysfunction, such as neuro-psychiatric disorders, lung diseases, hepatitis, chronic kidney failure, vitamin deficiencies, diabetes, hypothyroidism, were considered as exclusion criteria [33]. No participant had ever undergone VR therapy. Participants taking drugs impacting on the cochleo-vestibular system, or with a recorded addiction to drugs or tobacco/alcohol consumption, following diets diverting from the recommendations of Food and Agriculture Organization or World Health Organization [27] or having a BMI > 25 were excluded. Individuals were also excluded from the study groups if they were unable to understand examination procedures, or to participate in such procedures because of physical conditions. All participants were also asked to fill –before the study –a food frequency questionnaire (FFQ) designed according to local dietary habits, in order to avoid confounding factors related to individual nutritional habits [12]. Energy intake and macro- and micro-nutrients were calculated by a registered dietician who was blinded to the study using the Metadieta software application (Me.Te.Da., San Benedetto del Tronto, Italy), which includes the Italian database of food composition (INRAN/IEO, 2008) [12].
The study was approved by the Regional Lazio1 Institutional Review Board (registration ID 1668/2017) and it adhered to the principles of the Declaration of Helsinki. The study was registered in the public registry ClinicalTrials.gov (ID: NCT05174104) and all participants provided written informed consent after receiving a detailed explanation of the study.
A clinical otoneurological examination, including binocular electrooculography analysis with positional maneuvers, Head Shaking Test, clinical Head Impulse Test, gait observation, limb coordination tests, Romberg stance test, pure tone audiometry and impedance, was performed on all study participants [33]. Participants with UVH –before and after VR –and CG underwent:
Otoneurological testing
Video head impulse testing (vHIT)
The EyeSeeCam™ System and the analysis technique used in previous studies were deployed [10, 33]. Results were classified as abnormal if gain was out of the calculated normative data and refixation saccades (revealed by visual inspection, according to Blodow et al. [10]) were present. According to the technique proposed by McGarvie et al. [28] and previous experiences published by Blodow et al. [26], in order to reach adequate data only for the right and left horizontal semicircular canal, the operator delivered in a random order and direction—with the video assistance of OtoAccess™ software—head impulses matching pre-fixed requirements (head rotation 15°–20°, duration 150–200 ms, peak velocity > 150°/ s) to achieve ten artifact-free impulses per side in the participants of both groups [37]. Median (med) values recorded from both sides at 60 ms were extracted from the manufacturer’s software (OtoAccess™) on.xls files for raw analysis. In line with previous procedures [10, 33], UVH diagnosis was confirmed by means of vHIT recording a horizontal VOR gain below 0.75 and 0.76 for left and right sides, respectively. These values were calculated as the lower cutoff value of the gain reference range (meannormal±2 standard deviations (SDs)), which is equal to 0.89±2(0.07) and to 0.88±2(0.06) for left and right sides, respectively, incorporating 95% of healthy population and age- and gender-matched with the population of healthy volunteers screened by our laboratory.
Static posturography testing (SPT)
A standardized platform (EDM Euroclinic®) was used for SPT. Each participant was instructed to keep an upright position for a recording period of 60 s for each test (standing on the platform with eyes closed or open). The sampling frequency in the time domain was 25 Hz [5, 33]. The posturographic parameters that were considered in our study were the trace length (length, mm) and the surface of the ellipse of confidence (area, mm2) [33] according to Prieto et al. [42].
Self-report (SRM) and performance measures (PM)
The Italian Dizziness Handicap Inventory (DHI) is a 25-item questionnaire assessing patient’s functional (DHI-F; 9 questions), emotional (DHI-E; 9 questions) and physical (DHI-P; 7 questions) limitations on a three-point scale [41]. The maximum of 100 points indicates the greatest disturbance to the patient and the minimum of 0 points suggests that there is no handicap. The activities-specific balance confidence scale (ABC) is used to record the perceived level of balance confidence during 16 daily-living activities, with scores ranging from 0 (no confidence) to 100% (complete confidence) [20]. The Dynamic Gait Index (DGI) evaluates a person’s ability to perform gait activities, such as avoiding obstacles [20]. The scale has eight items and each item allows scores from 0 (lowest level of function) to 3 (highest level of function) [20], with a total score ranging between 0 and 24.
BIA measurements
For body composition analysis, participants arrived at the laboratory between 08.00–09.00 AM after an overnight fast (≥8 hours) in order to minimize the likelihood that total body impedance could have been altered by a close meal [25], having abstained from physical exercise and from caffeine or alcohol ingestion in the 24 hours prior to the trial [36]. Height was measured to the nearest centimeter using a Stadiometer (Holtain Ltd, UK) [36]. During measurements, individuals were required to only wear underwear. Although the BIA device used in this study was designed for self-measurement without the need for specific technical skills, the same researcher conducted BIA measurements for all participants [16]. Single-frequency BIA with eight-point tactile electrodes (Omron HBF-500 BIA, Omron Medizintechnik, Mannheim, Germany), whose reliability when compared to DXA and MRI measurements was previously demonstrated [11], was used. This device requires the participant to stand on metal footpads, barefoot, and grab a pair of electrodes fixed on a handle, with the arms extended in front of the chest [11]. Manufacturers’ equations were used to predict fat mass (FM, in %), skeletal muscle mass (MM, in %), grade of visceral fat (VFlevel) and resting energy expenditure (REE, in kilocalories [Kcal]) [17]. The participant’s age, gender and height (cm) were entered into the device before instructing the participant to step onto the platform with feet shoulder width apart [36]. Each person was tested three times and measurements were averaged [16].
Subjects free-living data collection
The Apple Watch 44 mm (5th generation) using watchOS 6 (Apple Inc., Cupertino, California, USA) was used. The device was handled according to manufacturer’s instructions. Participants were instructed to wear the device on their left wrist. Weight and height were recorded in the iPhone (Series 11) Health app before testing started. The Apple Watch “workout” setting allows for a selection of different activity types, which when outdoor can also use the GPS signal from a paired iPhone. The “workout” mode was switched on and off by participants at the beginning and at the end of each targeted condition (typing, loading the dishwasher, sweeping and walking upstairs and downstairs). Such activities were previously found as reliably tracked by the Apple Watch [13]. During “workout” mode the photoplethysmography recording function is activated continuously, while when not in “workout” mode recordings are obtained every 10 minutes [6].
Physical activity output is provided on the Apple Watch while more detailed information, such as total energy expenditure, is available through the associate “Activity” app. Functions “stand reminder”, “daily coaching” and “goal completions” were deactivated ‘a priori’ in our trial, in order to avoid giving unintentional feedback to study participants. Data were extracted using the iPhone Health app and the iPhone Health Export app [13].
Study participants were shown how to use the device, and they were instructed to record start and finish times for each targeted conditions, as well as filing a diary about any symptom or problem they would encounter during the recording period. Participants were told to wear the devices at all times apart from device recharging periods, and not to perform any physical activity considered as moderate-to-vigorous (referring to conditions reported in general literature [3]), a precautionary measure devised to avoid unintentional increase of risk of falls or other injury in participants with UVH, caused by inaccurate postural control in challenging situations [52]. According to previous studies considering a short-time period as a good proxy for free-living conditions, in the absence of particular restrictions [13], all participants were required to wear the device for a minimum of 36 hours, so that one full calendar day of activity measurements was obtained [6]; as regard participants affected by UVH, another recording of the same duration was performed after VR. After the recording period (RP), in hours, devices were collected from participants and the relevant data was filed by experimenters, together with a comparison with the diary information. Participant data collection involved total daily EE (Kcal/day), hours/day spent upright, number of strides, distance covered (Km) and daily movement EE (Kcal/day), while also including EE (Kcal/min) in the four targeted conditions (typing, loading the dishwasher, sweeping and walking upstairs and downstairs) [6].
Vestibular rehabilitation protocol
In the light of the history, physical examination, and diagnostic tests for each UVH participant, an exercise program was developed by an otoneurologist and administered to the subject by a skilled physiotherapist blinded to the study. The treatment program given to the participants consisted of training and exercise components. Balance system functions, causes of dizziness, and rationale and contraindications for performing of exercise were explained during the training component. Subjects affected by UVH were actively involved in adapting the exercise program to suit their symptoms, capabilities, and lifestyle. The execution of the exercises was personalized by the therapist according to the individual symptoms and functional disability. The exercises were designed to be challenging during the training period, and different aspects of balance training were emphasized for different participants to provide individualization. Exercises can be summarized as follows [18, 20].
Adaptation exercises
To improve gaze stability, subjects were initially asked to move their heads in yaw rotation while focusing on a stationary hand-held target, X1 viewing. They then progressed to X2 viewing, in which the target and the head rotated in equal and opposite yaw directions. Exercises were performed in horizontal and vertical planes 3 times a day for 1 minute each.
Substitution exercises
Participants with little or no vestibular function were taught to use vision and somatosensation to substitute for their loss of vestibular function. For example, a subject might be instructed to fixate gaze during ambulation to stabilize walking and to decrease veering to the side, or to stand on the foam with eyes closed to keep balance. Substitution exercises could be modified to become increasingly more difficult as the subject improved.
Desensitization exercises
Disturbances that the subjects experienced during performance of their daily activities were determined. In those who reported enhanced sensitivity or poor tolerance to self or visual motion, additional desensitization exercises were added.
Balance exercises
Subjects attempted to restore balance while switching between static (for example standing) and dynamic movements (for example walking) by altering visual, somatosensory, and vestibular impulses.
The exercise program consisted of 2 sessions a week for a period of 4 weeks, and each session lasted for approximately 30 to 45 minutes in the rehabilitation unit. All participants affected by UVH were followed up once a week by the otoneurologist, who reviewed the exercises and made changes together with the physiotherapist. In addition to the exercise they performed at the hospital, all subjects were given instructions with diagrams of exercises to be performed twice a day as a home exercise program. Each home program was designed to take approximately 30 to 40 minutes. Home programs consisted of 4 to 5 substitution, habituation, and balance exercises that the participants performed with difficulty at the rehabilitation unit. During the training period in the hospital, compliance was monitored by the otoneurologist and physiotherapist. Home exercises were monitored with a chart that was filled in every day by the subjects [18].
Statistical analysis
Following previous experiences strongly associating UVH to balance control alterations and to changes in SRM/PM [32, 34], the sample size was calculated to detect inter-group differences in the results for the posturography variables (surface and length in both closed and open eyes condition) and DGI, DHI and ABC. The sample size for the test hypothesis was calculated accordingly with the context (independent samples and continuous variables), using a statistical power of 80% (1 –β) for an a error probability of 0.05. We used the t-test for independent samples and an effect size of 0.80. We thus determined to include at least 44 participants per group. The X2 test was carried out to define associations between categorical factors and groups. Given their quantitative nature, descriptive data were calculated as mean±SD for otoneurological values, SRM/PM scores and BIA measurements and free-living data collection. To assess that data for independent samples were of Gaussian distribution, D’Agostino K squared normality and Levene’s homoscedasticity test were applied (where the null hypothesis is that the data are normally and homogeneously distributed). A between-group analysis of variance was performed for each otoneurological, SRM/PM, BIA and free-living variable. In order to obtain a unique entry of the VOR gain, the average between right and left side was calculated in CG participants in agreement with previous quantitative studies [31, 38]. Gender was treated as a categorical predictor, while age and UVH DD were treated, where possible, as categorical and continuous predictors. The significant cut-off level (α) was set at a p value of 0.05. Bonferroni correction for multiple comparisons was used for the post hoc test of the significant main effects, and the corrected level of significance was set at 0.017. Then, according to previous protocols [35] and given the exploratory nature of the study, a two-tailed Spearman’s rank correlation was performed in UVH participants between pre-/post-treatment differences (Δ) in those otoneurological, SRM/PM, BIA and free-living measures scores which resulted as significantly different when comparing the pre- and post- scores. Given the large sample size of this group and the two-tailed nature of the test, a significant cut-off level (α) was set at a p value of 0.05 (STATISTICA 7 package for Windows).
Results
Among 51 right-handed UVH participants, 2 presented VOR gain above the cutoff level, 1 was affected by type II diabetes mellitus, 1 suffered from thyroiditis and 1 reported alcohol consumption above reference levels. Thus, 46 adults affected by chronic UVH participated in the study (Fig. 1). No differences were found between CG and UVH pre-VR in terms of socio-demographic and nutritional aspects (detailed information in Table 1).

Diagram depicting enrollment, treatment and follow-up stages of the protocol. Unilateral vestibular hypofunction, UVH; video-head impulse test, vHIT.
Socio-demographic and etiological aspects of unilateral vestibular hypofunction (UVH) and control group (CG) participants
Vestibulo-ocular reflex, VOR; standard deviation, SD; kilogram, Kg; meter, m; gram, g; milligram, mg; kilocalories, kcal; body mass index, BMI; disease duration, DD; acoustic neuroma not eligible for surgery, AN; petrous surgery, petrous; cochlear surgery, cochlear; HI, Hearing impairment defined according to American Academy of Otolaryngology guidelines; left, L; right, R.
Post-hoc comparisons demonstrated UVH participants to have a significant post-treatment improvement in VOR gain of the affected side (p < 0.001), in surface (p = 0.004 and p < 0.001 in eyes open and closed respectively) and length (p = 0.006 and p < 0.001 in eyes open and closed respectively) measures and along DHI subscales (p < 0.001 in DHI-F, DHI-E, DHI-P and total DHI), DGI (p < 0.001) and ABC (p < 0.001) scales (Table 2). All the pre-treatment measurements were found to be significantly (p < 0.001) different when compared to CG. Post-treatment measures –excepted surface and length in eyes open condition –were found to be significantly (p < 0.001) different when compared to CG.
Within-subjects and between-group effects of otoneurological, self-report and performance measures and anthropometric variables in unilateral vestibular hypofunction –before and after vestibular rehabilitation - and control group participants
Main pre/post-vestibular rehabilitation (VR) and between-group effects of otoneurological, self-report and performance measures and anthropometric variables in unilateral vestibular hypofunction (UVH) and control group (CG) participants. Vestibulo-ocular reflex, VOR; opened eyes, OE; closed eyes, CE; Dizziness Handicap Inventory, DHI; Activities-speci?c Balance Con?dence scale, ABC; Dynamic Gait Index, DGI; kilogram, Kg; meter, m; Body Mass Index, BMI; Standard Deviation, SD. VOR gain refers to the affected side and to the average between right and left side for UVH and CG participants, respectively. *, # and †, respectively indicate post-hoc significant comparisons between pre- and post-VR UVH, pre-VR UVH and CG and post-VR UVH and CG. Exact p-values of post-hoc comparisons are given in the text.
Although no differences were found in terms of weight, height and BMI between pre and post-treatment UVH and when compared to CG participants, all the pre-treatment UVH BIA parameters were found to be significantly different when compared with CG subjects (p < 0.001 for FM% and VFlevel and REE; p = 0.002 for MM%). UVH participants demonstrated a significant post-treatment increase in MM% (p = 0.008) and when comparing post-treatment UVH to CG participants VFlevel and MM% were found to be no more statistically different (Table 3, Fig. 2A).
Within-subjects and between-group effects of bioelectrical impedance analysis and free-living data measurements in unilateral vestibular hypofunction –before and after vestibular rehabilitation - and control group participants
Main pre/post-vestibular rehabilitation (VR) and between-group effects of bioelectrical impedance analysis and free-living data measurements in unilateral vestibular hypofunction (UVH) and control group (CG) participants. Fat mass, FM; visceral fat, VF; resting energy expenditure, REE; kilocalories, kcal; minutes, min; Standard Deviation, SD. *, # and †, respectively indicate post-hoc significant comparisons between pre- and post-VR UVH, pre-VR UVH and CG and post-VR UVH and CG. Exact p-values of post-hoc comparisons are given in the text.
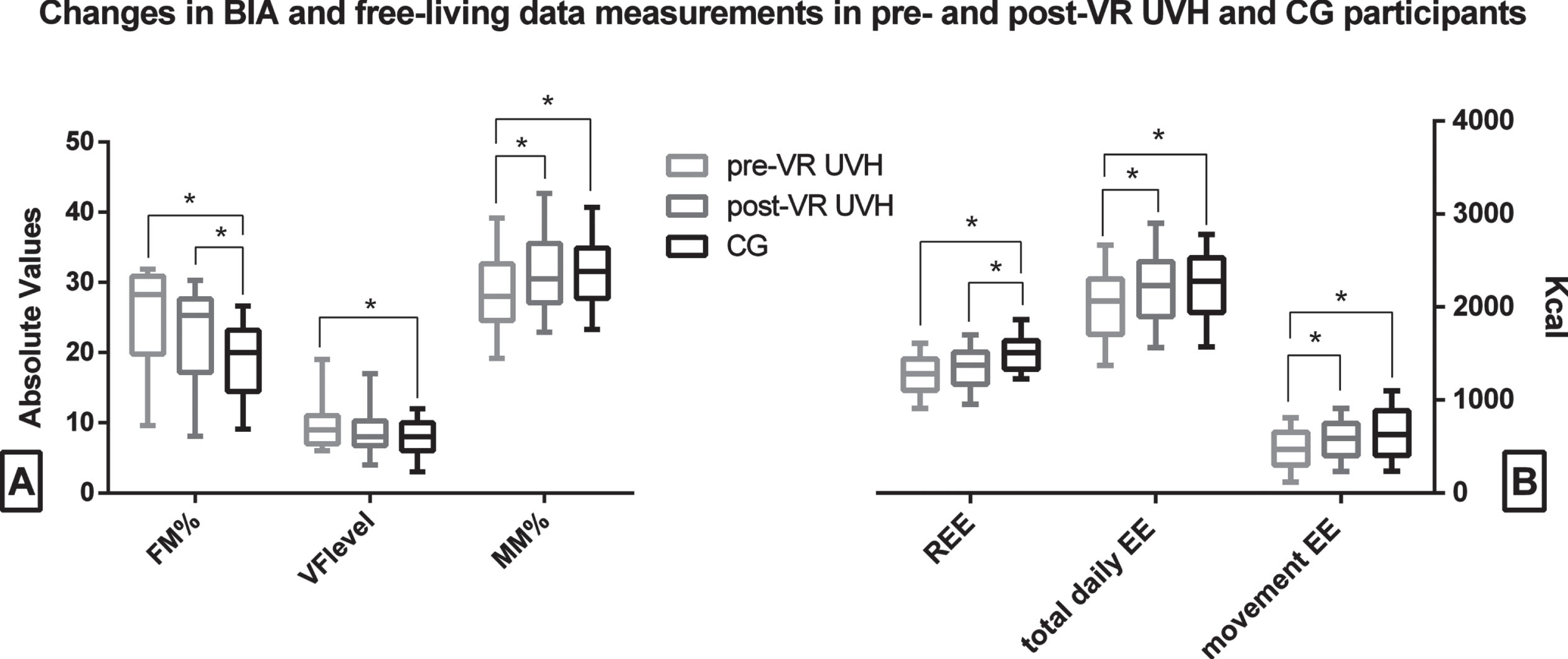
Box and whisker plot of differences in bioelectrical impedance analysis (BIA) (A) and free-living data measurements (B) between unilateral vestibular hypofunction (UVH) and control group (CG) participants. Fat mass, FM; visceral fat, VF; muscle mass, MM; kilocalories, Kcal; energy expenditure, EE; resting energy expenditure, REE. Brackets with asterisk indicate significant post-hoc comparisons. Values are reported as mean±standard devitation.
Pre-treatment UVH participants demonstrated significant lower values in movement EE (p < 0.001), hours/day spent upright (p < 0.001), number of strides (p < 0.001) and distance covered (p < 0.001) and total daily EE (p = 0.003) and to spend lower Kcal/min in sweeping (p < 0.001) and stairing (p < 0.001) with respect to CG (Table 3, Fig. 2B). After the VR protocol, UVH participants were found to significantly have an increase in movement EE (p = 0.008), total daily EE (p = 0.009) and number of strides (p = 0.009) and in Kcal/min spent in sweeping (p = 0.009) and stairing (p = 0.008) (Table 3, Fig. 2B). Post-treatment UVH participants demonstrated to be still significantly different to CG participants in terms of distance covered (p = 0.012) (Table 3). The UVH pre-VR, UVH post-VR and CG participants’ RPs were 28.3±2.4, 28.4±2.26 and 29.1±2.5 hours respectively and no significant symptom or setbacks possibly impacting on an adequate RP was reported in the diary in both groups.
Finally, in UVH participants a significant negative correlation was found between DD and ΔMM% (r = –0.69) and positive correlations were found between Δtotal daily EE and Δtotal DHI (r = 0.70), between Δmovement EE and ΔVOR gain of the affected side (r = 0.67) and between ΔKcal/min spent in stairing and ΔDGI (r = 0.73) (Fig. 3).
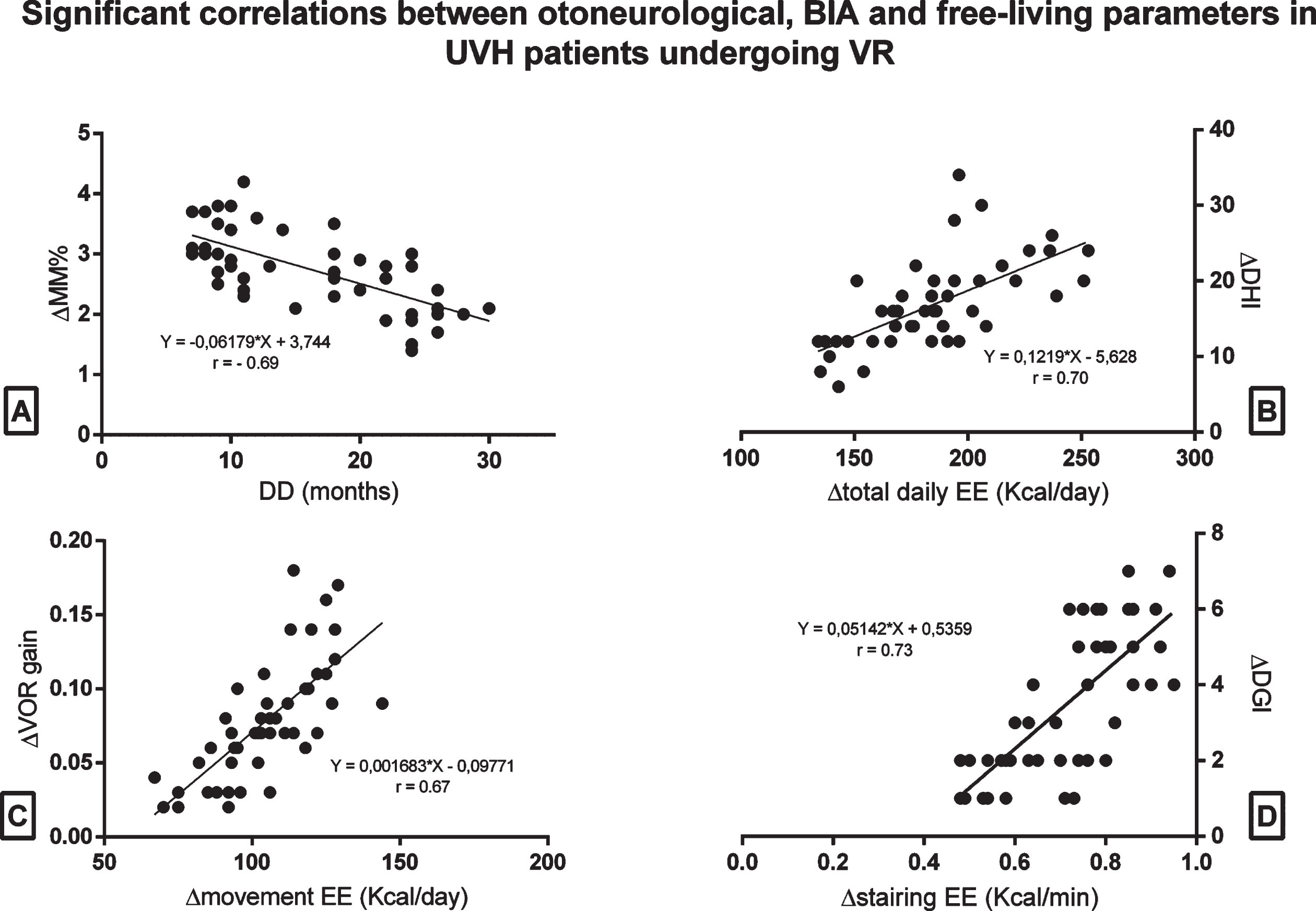
Significant negative correlation found in unilateral vestibular hypofunction (UVH) between disease duration (DD) and differences between pre and post-VR protocol (Δ) muscle mass percentage MM% (A). Significant positive correlations found in UVH between Δtotal daily energy expenditure (EE) and Δtotal Dizziness Handicap Inventory (DHI) (B), between Δmovement EE and Δ vestibulo-ocular reflex (VOR) gain of the affected side (C) and between Δ kilocalories/minute spent in stairing and Δ Dynamic Gait Index (DGI) (D). Kcal, kilocalories; min, minute.
Besides an expected improvement in otoneurological parameters (VOR gain, SPT parameters) and SRM/PM (DHI, DGI and ABC) after VR in UVH participants, which confirms previous studies related to the effectiveness of this kind of rehabilitation protocols [19, 34], the main interesting findings of the present study reside in the significant improvement found in body composition and daily-life related activities and EE after VR.
Interestingly, adults with UVH, after VR, demonstrated increases in MM%, total daily EE, movement EE, number of strides and Kcal/min spent in sweeping and stairing (Table 3, Fig. 2). Further, when comparing post-treatment UVH participants to CG, these parameters did not show any significant difference, as opposed to the differences found between pre-treatment UVH scores and controls.
Vestibular pathways are widely entangled at multiple central levels, thus vestibular dysfunction results in a complex syndrome, whose boundaries may include not only reflex balance impairment, but also a wide spectrum of spatial memory, cognitive and –especially –autonomic disorders [49]. In this scenario, present results corroborate previous studies demonstrating VR as exerting its effectiveness on multiple central levels [26]. Thus, if on one side VR demonstrated to be capable to impact on the basic output of the vestibular system, encoding angular and linear acceleration of the head in three dimensions and generating the VOR and vestibulo-spinal reflex [14, 19], for the first time, present data showed that its effectiveness may overcome such boundaries and extend to the connections between the vestibular system and brainstem autonomic centers.
In particular, studies addressed the medial and lateral vestibular nuclei as part of a complex neuronal pathway involving connections to the arcuate nucleus and the central melanocortin system, which are involved in energy homeostasis [29]. Melanocortinergic neurons have been found in the medial vestibular nucleus [43], while both the lateral and medial vestibular nuclei were showed to express enzymes involved in melanocortin signaling [22]. In this scenario, definite physiological evidences suggest the vestibular system to play an important role in homeostasis and the neuro-anatomical architecture allowing the vestibular system to perform this role at different levels [29, 30]. Beyond the fact that otolith stimulation has been found to cause the activation of the arcuate nucleus (ARC), which lies at the heart of the central melanocortin system, studies addressed medial (MVe) and lateral vestibular nuclei (LVe) as key points of this pathway [29]. Melanocortinergic neurons have been found in the MVe [43], while expression of the prolyl carboxypeptidase, an enzyme that play an important role in the modulation of melanocortin signaling, has been found in both LVe and MVe [22]. These structures, in turn, project specifically to pro-opiomelanocortin neurons in the nucleus of the solitary tract [50], which constitutes part of the central melanocortin system [21].
It is also noteworthy that previous evidence has shown a link between vestibular impairment and gait abnormalities in people with vestibular weakness, including decreased gait speed and increased variability in stance and swing time [7]. Specifically, vestibular cues are more influential during the dynamic phases of gait (e.g., weight transfer) compared with inverted pendulum phases (e.g., single-limb stance) [8]. Trials on people with vestibular loss demonstrated that vestibular cues play critical roles in the coordination of head and trunk movement [51]. Compared to healthy controls, individuals with vestibular dysfunction were found to walk with reduced gait speed, have alterations in center of mass movement, have impaired head orientation in conditions which preclude visual input, and prioritize trunk stabilization over head stabilization in eyes closed conditions [51]. These alterations have been associated to the debilitating effects that negatively affect vestibulo-ocular and vestibulospinal reflexes, which in turn affect quality of life, including severe balance deficits, inactivity and an increased risk of falls [45].
The implementation of VR may have possibly counteracted the mosaic of biological events occurring during the chronic stage of UVH, when deafferentation of vestibular nuclei takes place [15]. A patient-tailored, structured VR cycle could have impacted on lasting structural changes (i.e. reactive synaptogenesis or collateral axonal sprouting) which are thought to be less present within the deafferented vestibular nuclei. This lack of rearrangement by these circuits may have consequences along brainstem autonomic centers involved in energy homeostasis and gait and postural performance in which the vestibular system is entangled [48]. Speculatively, this may have led to significant increase in MM% and EE spent daily and during movement and –beside not surviving to post-hoc corrections possibly due to the short duration of the VR protocol –to decrease in FM%, VFlevel and increase in REE.
In this scenario, the significant negative correlation found between DD and ΔMM% and positive correlations found between Δtotal daily EE and Δtotal DHI, between Δmovement EE and ΔVOR gain of the affected side and between ΔKcal/min spent in stairing and ΔDGI (Fig. 3), tend to corroborate hypotheses indicating vestibular stimulation induced by the VR to act as a key regulator of muscle protein synthesis [23], foster muscle sympathetic nerve activity, regulate energy expenditure and tissue metabolism [44] and to be involved in the bi-directional interaction between obesity and sarcopenia and their association to the impairment of physical, postural and gait performance [24]. Clearly, these results could be interpreted in the light of the fact that also the repetitive exercises included in the VR may have influenced by themselves changes in BIA measurements and free-living data. VR may have indeed acted by contrasting inactivity, induced by sedentarism related to vestibular hypofunction, which may itself cause a rapid loss of muscle mass, particularly affecting antigravitary muscles that are constantly used for sustaining an upright posture, to perform movement and for maintaining balance [40].
In conclusion, present data showed, for the first time, that VR protocols may impact on metabolic function and body composition, possibly by i) contrasting structural changes involved within the deafferented vestibular nuclei, with consequences on neural pathways entangled in energy homeostasis, body composition, gait and postural performance and ii) contrasting inactivity, and its related consequences, inducing individuals to perform repetitive exercise. These results –which could open future perspectives in terms of the clinical and research approach to vestibular weakness and VR –deserve further in-depth studies.
Limitations of the study
The main limitation of the present study resides in the absence of a thorough assessment free-living data collection under physical activity and for a longer recording period in both UVH and CG participants. These aspects could have provided additional information related to different energy expenditure behavior. However, although everyday life recordings have been suggested to mitigate the overemphasizing effects of laboratory tests [46], the specifics of any given activity protocol (including our own) are unlikely to represent the distribution and importance of various activities in normal life, so it could be beneficial to assess a more prolonged recording time in free-living conditions [39]. Thus, further research including body composition and activity tracker assessment under physical activity for a longer recording period is needed to clarify hidden changes in body composition and in daily EE behavior in UVH patients. Finally, the possibility that patients might forget to switch on and off the activity tracker at the beginning and the end of the targeted activity could constitute a possible drawback in this kind of studies. This highlights the importance of an adequate training of participants and a strict monitoring by using a diary, which increased the likelihood of avoiding such circumstances.
Conflict of interests
The authors declare that they have no conflict of interest.