
Abstract
BACKGROUND/OBJECTIVE:
There exists limited information in the literature on dominant hand preference in relation with vHIT applications. The present study aimed to examine the relationship between the clinician’s dominant use of right- or left-hand and vHIT results.
METHODS:
A Synapsys vHIT Ulmer device was used in the study. The tests were administered by 3 clinicians experienced in vHIT, 2 of whom were right-handed and 1 left-handed. The test was applied to the 94 participants three times, one week apart.
RESULTS:
In this study, the correlation between right-handed clinicians and left-handed clinicians was examined, and in all SCCs, namely RA, LA, RL, LL, RP and LP, a moderate positive significant correlation was found between right-handed1 and right-handed2, between right-handed1 and left-handed, and between right-handed2 and left-handed.
CONCLUSIONS:
In this study, these findings suggested that measures were reliable across test sessions regardless of hand dominancy (right or left). Based on the vHIT results we obtained with three different right- or left-handed clinicians, the clinician should evaluate the results according to the dominant side.
Keywords
Introduction
The vestibulo-ocular reflex (VOR) stabilizes images on the retina by moving the eye in the opposite direction of the head, at the same degree and speed as the head, during head movement, thus helping to keep the image in the center of the visual field [4]. The vestibular system provides stable vision during head movements in this way. Anatomical components of the VOR consist of semicircular canals (SCCs) in the peripheral vestibular system, vestibular and ocular motor nuclei in the brainstem, and extra-ocular muscles [4].
VOR pathways evoked by the lateral SCC may be assessed with caloric testing, rotational chair testing, and scleral search coil testing [5]. The Video Head Impulse test (vHIT), which has been developed in recent years, enables the evaluation of VOR by stimulating 6 SCCs in a higher frequency range than these tests [12]. The vHIT records head and eye movements during and immediately after passive head impulses using a high-speed video camera, providing information about VOR gain and refixation saccades that are sometimes invisible to the naked eye. VOR gain is defined as the ratio of the slow phase compensating eye velocity to the head sway velocity [4].
Studies in healthy participants without vestibular pathologies showed good test-retest reliability with no significant difference in VOR gain between test sessions [1, 12]. There exists no study in the literature on dominant hand preference in relation with vHIT applications. Matino-Soler et al.,(2015) stated that the fact that swinging to the left causes higher acceleration may be related to using the right hand dominantly [6]. The present study aimed to examine the relationship between clinician’s dominant use of right- or left-hand and vHIT results. Our hypothesis in this study was dominant hand preference differentiates vHIT gains. Because the dominant hand is stronger, pushing with the dominant hand causes higher speed acceleration [6]. It causes lower VOR gain at higher speed accelerations. Therefore, for right-handed individuals, we expect these: RL VOR gain > LL VOR gain, LA VOR gain > RA VOR gain, and RP VOR gain > LP VOR gain. For left-handed individuals, we expect: LL VOR gain > RL VOR gain, RA VOR gain > LA VOR gain, and LP VOR gain > RP VOR gain.
Material method
This study was approved by the University Medical and Health Sciences Research Board and the Non-Invasive Clinical Research Ethics Committee of the university (Date: 01/10/2021 and Decision number: 2021/3421). Each participant was informed about the study and signed an informed consent form. The study was conducted at a local university hospital.
According to the calculation made with the G*power 3.1 program, the sample size was determined as at least 84 with an effect size of 0.20, margin of error of 0.05, a confidence level of 0.95, and a population representative power of 0.95. The sample size of this study was determined by power analysis. During the study, one individual was excluded due to droopy eyelids. The study included 94 individuals (43 males and 51 females). The inclusion criteria were having results in the normal range in pure-tone audiometry and bone-conduction audiometry. The bithermal caloric test, spontaneous nystagmus test, finger nose test, dysdiadochokinesia, Romberg test, sharpened Romberg test, straight walking test, toe heel walking test and positional tests were performed after detailed anamnesis taken to rule out central and peripheral vestibular system and pathologies. Any bithermal caloric test result above 25% was accepted as an exclusion criterion. The exclusion criteria were having psychological or neurological condition that would interfere with participation in the study; having a history of dizziness; having a history of motion sickness; having a history of a head injury/ear surgery; and, the presence of a cervical pathology or visual impairment.
A Synapsys vHIT Ulmer device was used in the study. The vHIT system consists of a high speed (100 Hz) infrared video camera mounted on an adjustable monopod, the ULMER II software, and a computer. Video signals were low-pass filtered below 25 Hz by the system, thus avoiding possible aliasing of high-frequency signals. For each canal plane, the operator tries to rotate the head at a velocity of 150–200°/s. The video camera recorded head and eye movements during head impulses. Minimum head acceleration was set at a threshold of 2000°/sec2 horizontal acceleration, and a threshold of 1500°/sec2 vertical acceleration. In horizontal and vertical SCCs, the synapsis vHIT device accepts or rejects the impulses according to these acceleration amounts. In the outputs we obtained as a result of the test, there was no result for acceleration. Individuals sat at a distance of 90 cm from the camera. The participants were asked to look at the fixed red lights at eye level 2 m away. The tests were administered by a total of 3 clinicians experienced in vHIT, 2 of whom were right-handed and 1 left-handed. After entering the case number and date of birth information attributed to the individuals into the system, calibration was performed to ensure the reliability of the pupil records taken from the eyes. During the calibration, the individual was asked to look steadily at the determined red target point without blinking. In addition, there were horizontal rectangular shapes for horizontal canals and vertical rectangular shapes for vertical canals on each SCC plane during the impulses. When the eye movements exceeded the rectangular shape as a result of the impulse, the push was considered invalid. The tests were administered at one-week intervals. In the study of Mutlu et al., (2020) which examined the difference between clinicians in vHIT measurements, clinicians applied 4 test sessions for a patient with a 10-minute break [9]. They explained the reason for their break as follows: “Breaks were offered to the participants throughout testing to minimize excessive blinks and fatigue”. In our study, on the other hand, there was a 1week period between test applications performed by 3 different clinicians on 1 patient. In the first week, the right-handed clinician1 performed the test, in the 2nd week, the right-handed clinician2 performed the test, and at the 3rd week, the left-handed dominant clinician performed the test. The 3 clinicians in our study performed the tests randomly, regardless of any order. In addition, two authors (FI and DUC) in the study blindly analyzed the vHIT test analysis graphic results independently, without knowing which tester (TE, SM, and SK) was using which hand. Six SCCs were randomly evaluated in 3 planes: lateral SCC and RA-LP (right anterior - left posterior) and LA-RP (left anterior - right posterior) SCCs. The important point here is to bring SCCs to the anatomically appropriate position and then apply the impulses. All three clinicians placed the same hand positioning on the individual for lateral canal SCCs (Fig. 1A). For lateral SCCs, hand positioning was done as follows. The two hands were placed on the top of the head, with the thumb on the upper back of the head, and the other fingers away from the forehead. For the stimulation of the lateral SCCs, the head was grasped with both hands and flexed 30 degrees while the individual was looking at the target, and sudden, unpredictable 10°–20° of impulses were applied to the right and left in the horizontal plane (Fig. 1A). In the assessment with the Synapsis vHIT device we used in the study, the subject was asked to turn their head 45° to the right in the horizontal plane and look at the fixed target on the opposite side for the LA-RP SCC plane, and 10°–20° impulses were applied in the vertical plane in the up and down directions (Fig. 1B). There were rectangular frames that ensure the accuracy of 45° right rotation in the horizontal plane [7] and 10°–20° impulses in the vertical plane during the pushes. The device only accepts eye movements that occur within these frames. For the RA-LP SCC plane, the subject was asked to turn their head 45° to the left in the horizontal plane [7] and look at the fixed target on the opposite side, and 10°-20° impulses were applied in the vertical plane in the up and down directions (Fig. 1C). There was a rectangular box in the RA-LP SCC plane, which also ensures the accuracy of the thrusts. Individuals were given 5–8 impulses for each SCC. The vHIT test result of an individual administered by three clinicians is given in Fig. 2.

A) Clinicians’ hand positions for RL and LL SCC, B) Clinicians’ hand positions for LA and RP SCC, C) Clinicians’ hand positions for RA and LP SCC.
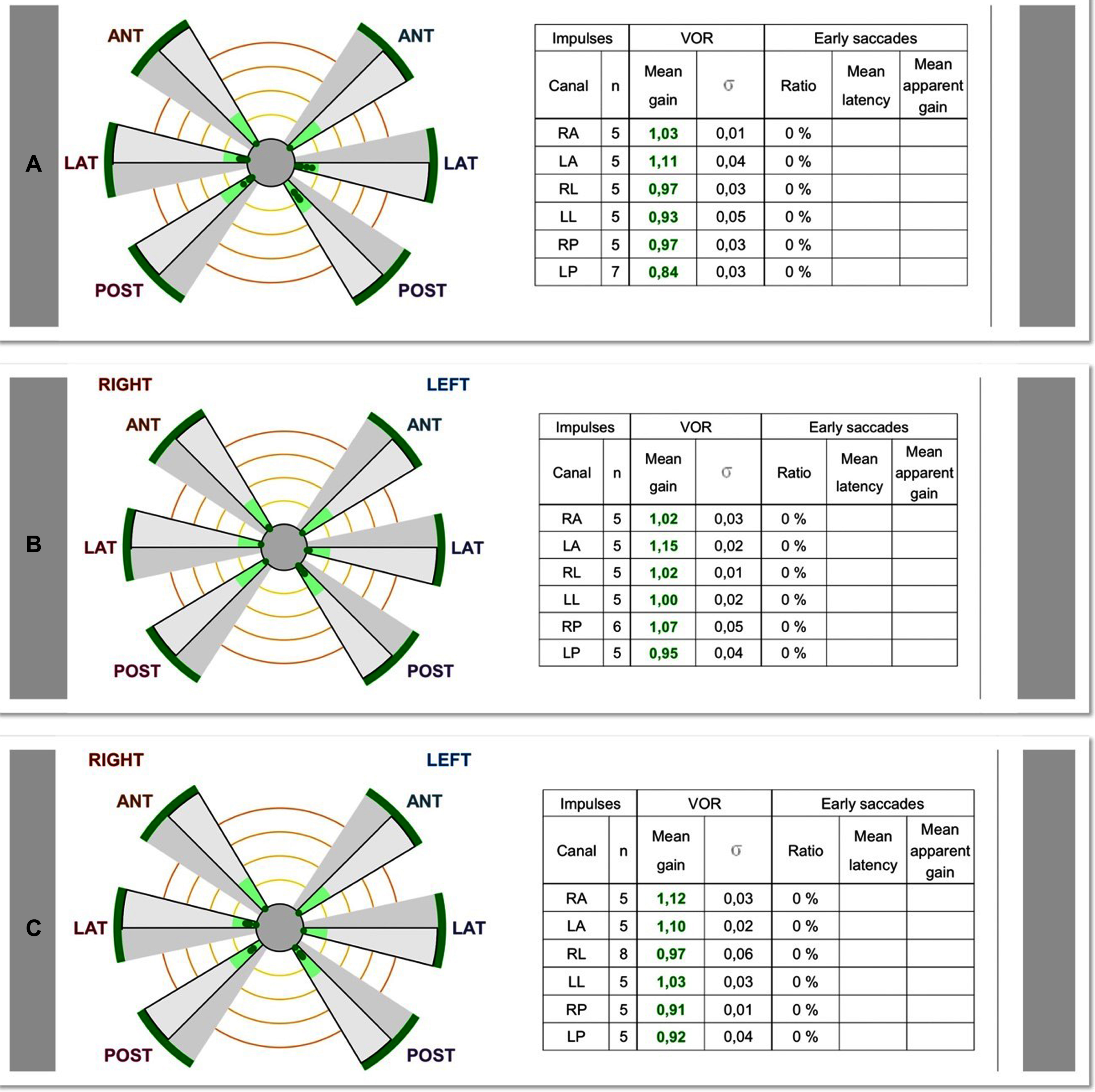
vHIT results of an individual A) Right-handed1 clinician, B) Right-handed2 clinician, C) Left-handed clinician.
The analysis of the data included in the research was carried out with the SPSS (Statistical Program in Social Sciences) 25 program. The Kolmogorov Smirnov Test was used to check whether the data included in the study fit the normal distribution.
Pearson correlation coefficient was also calculated. Interpretation of the values used in the evaluation of the findings: 0.00–0.19 no relationship (negligible), 0.20–0.39 weak relationship, 0.40–0.69 moderate relationship, 0.70–0.89 strong relationship, and 0.90–1.00 very strong relationship.
The evaluation of the measurement of the same subject among different observers is the dependent groups test setup. Dependent comparison tests are applied in the analyses to be made for dependent groups.
Comparisons of intra-clinician measurements were made with the repeated measure of ANOVA test for comparisons between clinicians.
All participants included in the study were provided with similar test setups and conditions, and the measurement values of the tests were recorded.
Results
The study included 94 participants: 51 (54.3%) females and 43 (45.7%) males. The mean age of the participants was 24.84±1.81 years, and the lowest age was 20 and the highest age was 29.
Intra-group and inter-group evaluation of measurements
The repeated measure of ANOVA test was used to evaluate whether there was a difference in the measurements. Information about the test results and descriptive statistical values are given in Table 1 below.
Pairwise comparisons of the mean VOR gains obtained in each semicircular canal by the vHIT measurements made by right-handed1, right-handed2, and left-handed testers and right handed1- right handed2, right handed1-left handed, and right handed2-left handed testers
Pairwise comparisons of the mean VOR gains obtained in each semicircular canal by the vHIT measurements made by right-handed1, right-handed2, and left-handed testers and right handed1- right handed2, right handed1-left handed, and right handed2-left handed testers
SD:StandardDeviation, sig1; statistical significance of Repeated Measure of ANOVA, sig2; *p < 0.05, There is a statistically significant between the two groups.
A statistically significant difference was found between the measurements of RA, LA, RL, LL, RP, and LP SCCs (p < 0.05) (Table 1).
While a statistically significant difference was observed in RA, RP, and LP SCCs between right-handed1 and left-handed clinicians (p < 0.05), no significant difference was observed in LA, RL, and LL SCCs (p > 0.05). While statistically significant difference was observed between right-handed2 and left-handed clinicians only in RA SCC (p < 0.05), no significant difference was observed in LA, RL, LL, RP, and LP SCCs (p > 0.05). A statistically significant difference was observed between right-handed1 and right-handed2 clinicians in all SCCs, namely RA, LA, RL, LL, RP, and LP (p < 0.05) (Table 1).
For all SCCs (RA, LA, RL, LL, RP, LP), there was a moderately significant positive correlation between right-handed1 and right-handed2 (p < 0.05). For all SCCs, there was a moderate significant positive correlation between right-handed1 and left-handed (p < 0.05). For all SCCs, there was a moderate significant positive correlation between right-handed2 and left-handed (p < 0.05) (Table 2).
Correlation of VOR gains by vHIT measurements of right handed1- right handed2, right\\ handed1-left handed, and right handed2-left handed testers for each semicircular canal
r; between two observation correlation coefficient, sig; *p < 0.05, There is a statistically significant relationship between the two tests.
In this study, the correlation between right-handed clinicians and left-handed clinicians was examined, and in all SCCs, namely RA, LA, RL, LL, RP and LP, a moderate positive significant correlation was found between right-handed1 and right-handed2, between right-handed1 and left-handed, and between right-handed2 and left-handed. To the best of the authors’ knowledge, there exists no study on dominant hand preference in vHIT evaluations in the literature. For this reason, for the planes where RA-LP/LA-RP SCCs are located, we preferred the ergonomically more comfortable hand positioning of the pushes, which is frequently applied in the literature, regardless of the clinicians’ dominant hand use. Since our aim was to examine the effect of the clinician’s dominant hand on the results, especially for the planes where the RA-LP/LA-RP SCCs are located, we asked three clinicians to apply the test with the same hand positioning and grip style.
In this study, it was observed that the VOR gain of the side where the head was moved was higher in lateral SCCs (mean right lateral SCC VOR gain > mean left lateral SCC VOR gain) for right-handed clinicians (Figs. 3–5). It was observed that for the left-handed clinician, lower VOR gain was obtained for the lateral SCCs (mean right lateral SCC VOR gain < mean left lateral SCC VOR gain) in the direction of head movement (Figs. 3–5). Matino- Soler et al., (2015) evaluated only lateral SCCs with the vHIT device used by a right-handed clinician, and observed that the average rightward velocity of the head impulse they applied in their study was lower than the leftward velocity [6]. They commented that higher speeds result in lower VOR gain. They reported that this factor causes higher VOR gain in the right lateral SCC compared to the left lateral SCC for rightward impulses [6]. Similarly, Patterson et al., (2015) evaluated vHIT results in different grip positions on lateral SCCs applied by a right-handed clinician, and observed that the right lateral SCC VOR gain was higher than the left lateral SCC VOR gain [10]. Apart from these studies in lateral SCCs, there are studies in which all six SCCs are evaluated by only one right-handed clinician [1, 3]. The method and results of similar studies are tabulated and summarized (Table 3). In our study, we evaluated six SCCs as in these studies and vHIT test results applied by two right-handed clinicians in our study were similar, agreeing with these studies. Higher VOR gain was obtained in the right lateral SCC than in the left lateral SCC, in the left anterior SCC than the right anterior SCC, and in the right posterior SCC than in the left posterior SCC. However, the device does not give a figure for acceleration in the outputs we obtained as a result of the test. Our hypothesis in our study was that if the dominant hand could apply higher speed, we would get lower VOR gain. Since there is no speed information on the device, we could not examine the relationship between VOR gain and speed separately.
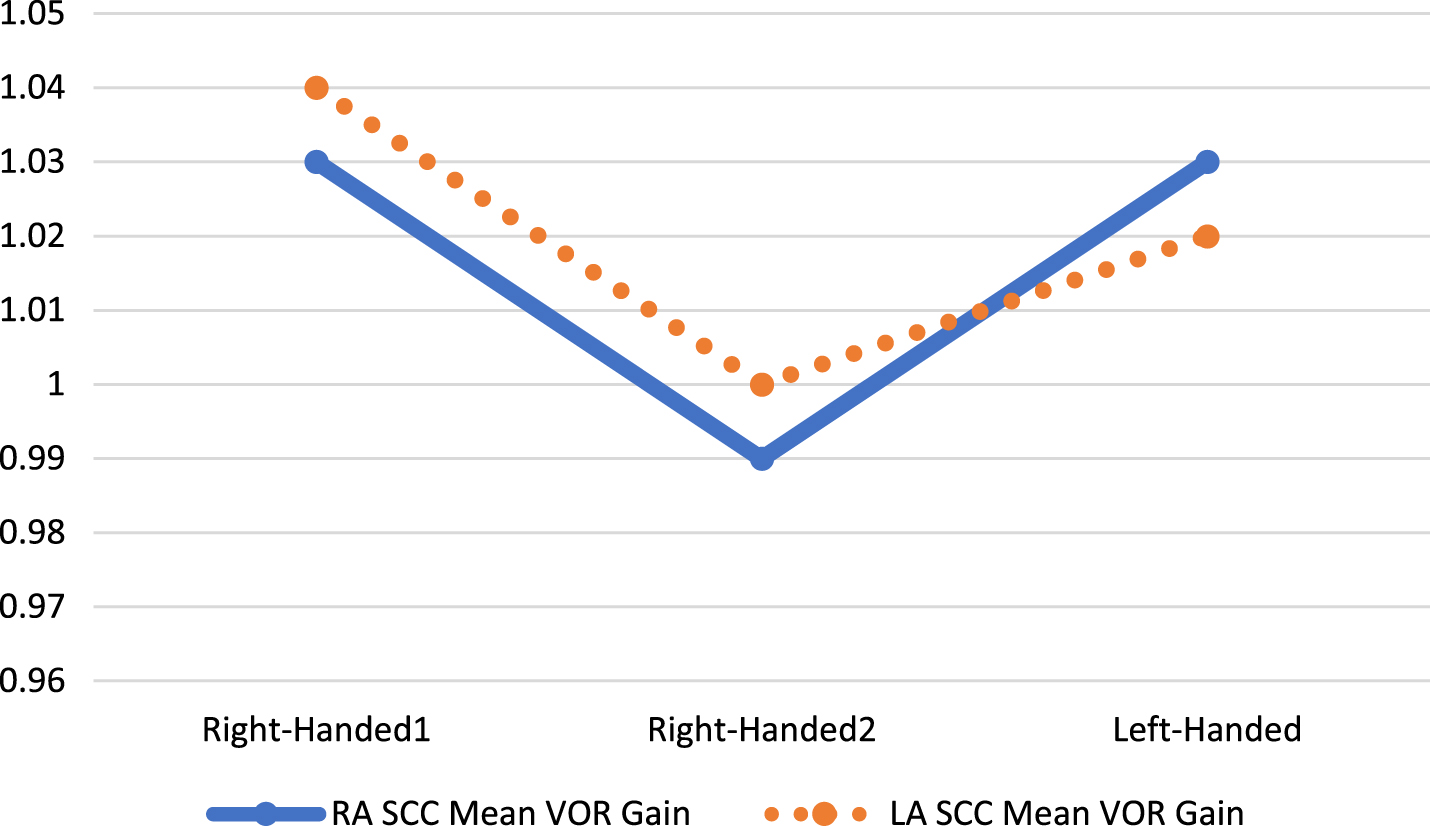
The mean VOR gains obtained in RA and LA SCCs by the vHIT measurements made by right-handed1, right-handed2, and left-handed testers.

The mean VOR gains obtained in RL and LL SCCs by the vHIT measurements made by right-handed1, right-handed2, and left-handed testers.

The mean VOR gains obtained in RP and LP SCCs by the vHIT measurements made by right-handed1, right-handed2, and left-handed testers.
In the following studies where the VOR gain in semicircular canals was evaluated using fHIT and vHIT devices, information given about the effect of right hand dominance on VOR gain in semicircular canals by the testers
The fHIT (Functional Head Impulse test) is a test method with a similar impulse system with vHIT and functionally evaluates the VOR. In this method, the individual tries to correctly predict the direction of the Landolt C character, which flashes briefly on the screen during head impulses in the LL-RL, RA-LP, and LA-RP SCCs. The average rate of correct answers (RCA) is calculated from the answers that the participant gives correctly. Similar to our study, in a study with the fHIT device performed by a right-handed clinician, the followings were found: right anterior SCC RCA was higher than that of the left anterior SCC; right posterior SCC RCA was higher than that of the left posterior SCC; and, right lateral SCC RCA was higher than that of the left lateral SCC. They explained the reason as follows: due to the clinician’s right-hand dominant use, the average rightward velocity of head impulses was lower than that of the leftward velocity, resulting in higher RCA obtained during head impulses [2].
In this study, both the right-handed and left-handed clinicians applied impulses in the RA-LP SCC plane, the clinician placed their left hand on the individual’s chin, while the right hand was placed on the head and applied the impulse. For the LA-RP SCC plane, both the right-handed and left-handed clinicians placed their right hand on the individual’s chin, while the left hand was placed on the head and applied the impulse. Higher VOR gain was obtained in the left anterior canal compared to the right anterior canal, and in the right posterior canal compared to the left posterior canal. We think that the reason for this is the lower VOR gain due to an unintentional higher acceleration in the impulses where the person performing the impulse uses their dominant hand more actively for impulses. In our study, there was no statistically significant difference only between right-handed clinicians and left-handed clinicians; there was a statistically significant difference among right-handed clinicians in some SCCs; and, even in some SCCs, there was no statistical difference between right-handed clinicians and left-handed clinicians. In our study, our hypothesis was that the dominant hand would apply more speed, and thus, lower VOR gain would be obtained. According to the SCC VOR results we obtained from the ANOVA results, there are more differences in terms of VOR gain in SCC among clinicians with the same hand dominance (righthanded 1- right handed 2) than clinicians with different hand dominance (right-handed1-left-handed and right-handed2-left-handed). It seems that a real message here is that there may be some hand dominance differences noted, but really test-retest conditions should be with the same clinician to minimize the difference due to the technique. In future studies, in addition to comparing right-handed and left-handed clinicians with the same hand dominance, more precise information on hand dominance can be obtained and technical errors can be minimized by examining intra-clinician test-retest results. Furthermore, we attributed this outcome to the user difference rather than the right or left-hand dominancy of the individuals.
A previous study with a scleral search coil for lateral SCCs showed that when both eyes were recorded during head impulses, VOR gain was higher in the adducting eye than in the abducting eye [13]. In our study, video recordings were taken for both eyes, as in the scleral search coil test technique. While the explanations regarding the different behaviors of the extraocular medial and lateral rectus muscles in the studies of Weber et al. (2008), and the findings of VOR gain as a result of vHIT performed by the right-handed clinician in our study were consistent, but it was not compatible with the findings of VOR gain resulting from vHIT performed by the left-handed clinician. In this study, the clinician’s dominant hand was not stated [13]. Therefore, we think that this result is compatible with right-handed individuals and should be compared with the results of left-handed clinicians.
In a study involving a healthy pediatric group, the test-retest reliability and interrater reliability for the VOR mean gain estimate was good for all canals [11]. In another study comparing the test results of healthy individuals and individuals with vestibular pathology, again it was observed that the agreement of test-retest results was excellent for all SCCs, both in healthy individuals and in the affected and unaffected ears of the group with vestibular involvement [12]. In our study, while a good agreement was observed in lateral SCCs, an acceptable agreement was observed in vertical SCCs, and we think that one reason for this outcome may be due to the minimum horizontal acceleration threshold was set at 2000°/sec2, while the vertical acceleration threshold was set at 1500°/sec2 in the vHIT device. Another reason may be that we may have reached different results because impulse can be done more easily in lateral SCCs.
One of the limitation of our study was that different dominant features can be observed in organs such as hands, feet, eyes, and ears in individuals. Since all 3 clinicians had homogeneous dominant characteristics, these results may differ for the test results applied by clinicians with different dominant characteristics. The other limitation is that we could not compare the relationship between velocity and VOR gain since the velocity score was not given exactly in the vHIT device used. In addition, better quality results could have been obtained by looking at the test-retest measurements of the clinicians themselves. Another limition is the interval between repeated measurements. Although there is no study in the literature examining the differences that may occur due to hand dominance, we could not find any study, except for one study that provided information on the interval between repeated measurements. In the study of Mutlu et al., (2020) in which they applied vHIT in 1 patient with 4 different clinicians, it was stated that there was a 10-minute break between the applications [9]. In our study, vHIT was applied in 1 patient by 3 different clinicians, with a 1-week break. There is no consensus in the literature on this issue. New studies that examine the effect of test interval on test results can be done in the same individual.
In this study, these findings suggest that measures are reliable across test sessions by different side hand dominancy (right or left). Based on the vHIT results we obtained with three different right- or left-handed clinicians, the clinician should evaluate the results according to the dominant side. We think that this study, which we carried out in healthy individuals, should be performed in individuals with unilateral vestibular pathology in the future.
Footnotes
Acknowledgments
The authors are grateful to all participants in this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Author contributions
Conceived and designed the experiments: TE, GK. Performed the experiments: TE, ŞK, SM, HA, MAD. Analyzed the data: Fİ, DUC, EK. Literature review: EK, FMK. Wrote the paper: TE, GK, FMK, EK. Revision: HA, MAD.