
Abstract
BACKGROUND:
Vestibular rehabilitation therapy (VRT) is effective for most patients with dizziness and imbalance. Home exercise programs are widely used. It is unknown, however, how specific the instructions for exercises have to be.
OBJECTIVE:
To evaluate the effects of expert assessment and instructions in a booklet-based home VRT program for patients with chronic dizziness.
METHODS:
Randomized controlled study on 74 participants with disabling dizziness for >3 months. All study participants received a booklet-based VRT for training at home. Participants were prescribed 20 minutes of exercise, twice a day. The intervention group (n = 37) received specific instructions (expert physiotherapist). The control group (n = 37) practiced without specific instructions. Primary outcome was the total score of the Dizziness Handicap Inventory (DHI-G). All outcomes were assessed at baseline, after 4 weeks, and at follow up 4 weeks later.
RESULTS:
Both groups improved (DHI-G 43.94±18.89 at inclusion to 33.06±19.67 at follow-up in controls and 42.82±16.60 to 22.65±19.12 in the intervention group). The intervention group, however, improved more (p = 0.014).
CONCLUSIONS:
We show a significant effect of expert physiotherapy guidance in home-based VRT. This strengthens the role of the physiotherapist in VRT: Tailored, personalized instructions are needed to get the best effect of VRT.
Introduction
Dizziness and vertigo are common complaints that often bother affected subjects over weeks, months, and years. Patients perceive an uncomfortable disruption of spatial orientation and suffer from the false perception of movements [3, 39].
The daily life of those affected is described as very restricted. Activities are avoided. Some patients with peripheral vestibular hypofunction suffer from persistent dizziness caused by incomplete vestibular compensation [4, 36, 45]. Further, secondary functional dizziness may develop after a vestibular disorder [10, 11, 15, 24]. Dizziness and vertigo contribute to limitations in daily life [32, 33]. The participation and independence of the affected is significantly limited. Especially in elderly patients with chronic dizziness gait unsteadiness and falls occur [40]. This may result in a fear of falling, which further reduces the patient’s mobility and activity [19]. Specific vestibular rehabilitation therapy (VRT) to adjust, substitute, and habituate deficits is an effective treatment option for patients with dizziness, vertigo and balance disorders [11, 29, 47]. Some guidance for vestibular exercises at home is already available for this purpose [5, 7–9]. Despite moderate to strong evidence for VRT, access is limited in many countries [15]. This is due to the lack of trained specialist therapists and to the insufficient standardization of treatment [49].
At our center, a vestibular rehabilitation booklet is provided for patients with various causes of dizziness and vertigo. Clinical experience suggests that patients who receive the booklet with specific instruction by an experienced physiotherapist do better than those receiving the booklet with just the general advice to do training with it. To optimize vestibular rehabilitation with self-exercise programs at home and thus to efficiently reduce symptoms, it seems important to examine the effect of specific physiotherapeutic instructions.
The primary purpose of the study was to examine the effects of a booklet-based exercise program that is individually adapted by a physiotherapist, compared to the more general standard instruction to use the booklet. A secondary purpose is to evaluate the efficacy of the tailored training program to reduce the intensity of dizziness and to improve balance. In addition, we asked whether fear of falling can be reduced and participation improves after the instructed treatment at home.
Methods
To estimate the sample size, previous vestibular rehabilitation studies in patients with vestibular disorders were reviewed [13, 28, 43]. Based on these data, we expected a mean improvement on the DHI questionnaire (=change in DHI total score) of 10±14 points for the intervention group compared to the control group. For a two-tailed hypothesis test with 80% power and a significance level of 5%, the required sample size yielded 31 patients in both the intervention and control groups. With an expected drop-out of 20%, 74 patients had to be included in the study.
Participants
Seventy-four adult study participants with chronic dizziness and balance disorders (symptoms for more than three months) were recruited for the study at the outpatient clinic of the German Center for Vertigo and Balance Disorders (DSGZ) at the Ludwig-Maximilians University of Munich. Potential participants were identified and asked to participate in the study after outpatient work-up. The recruiting period started in 2016 and ended in 2020. Patients with chronic dizziness, vertigo, and balance problems (>3 month) due to peripheral (uni- or bilateral hypofunction) or central vestibular (brainstem, cerebellum) disorders were included.
Exclusion criteria were: (1) episodic vertigo syndromes such as vestibular migraine, Meniere’s disease or benign paroxysmal positional vertigo; (2) recent changes (last 3 month) in the medication or planned changes during the two-month of individual study duration; (3) patients with orthopedic or neurological diseases that affect balance; (4) patients with contraindications to VRT (severe pain, severe cervical syndrome); (5) patients unable to follow verbal and written instructions or not able to give written informed consent; (6) patients who, unrelated to the study, received physiotherapy or occupational therapy interventions to treat dizziness and balance.
All study participants (n = 74) had the initial assessment (T0) and were randomized into the intervention group (n = 37) and the control group (n = 37). The randomization was done by the online software tool Randoulette (provided by the Institute for Medical Information Processing, Biometry and Epidemiology –IBE at the LMU Munich; www.en.ibe.med.uni-muenchen.de/services/studienrandomisierung/index.html). Block randomization (block sizes of 2, 4 and 6) ensured a 1:1 ratio in terms of size of the intervention and control groups, peripheral and central diseases, sex and age. Study participants and investigators were blinded to group allocation. The physiotherapist was not blinded. After four weeks of training, the post-intervention assessment (T1) was done and the follow-up examinations (T2) were executed after another four weeks (Fig. 2). Participants were advised to continue exercising during the follow-up period. The follow-up could be carried out in a total of 68 study participants (Fig. 1). The dropouts were included in the descriptive and comparative statistics of the participant characteristics at T0.
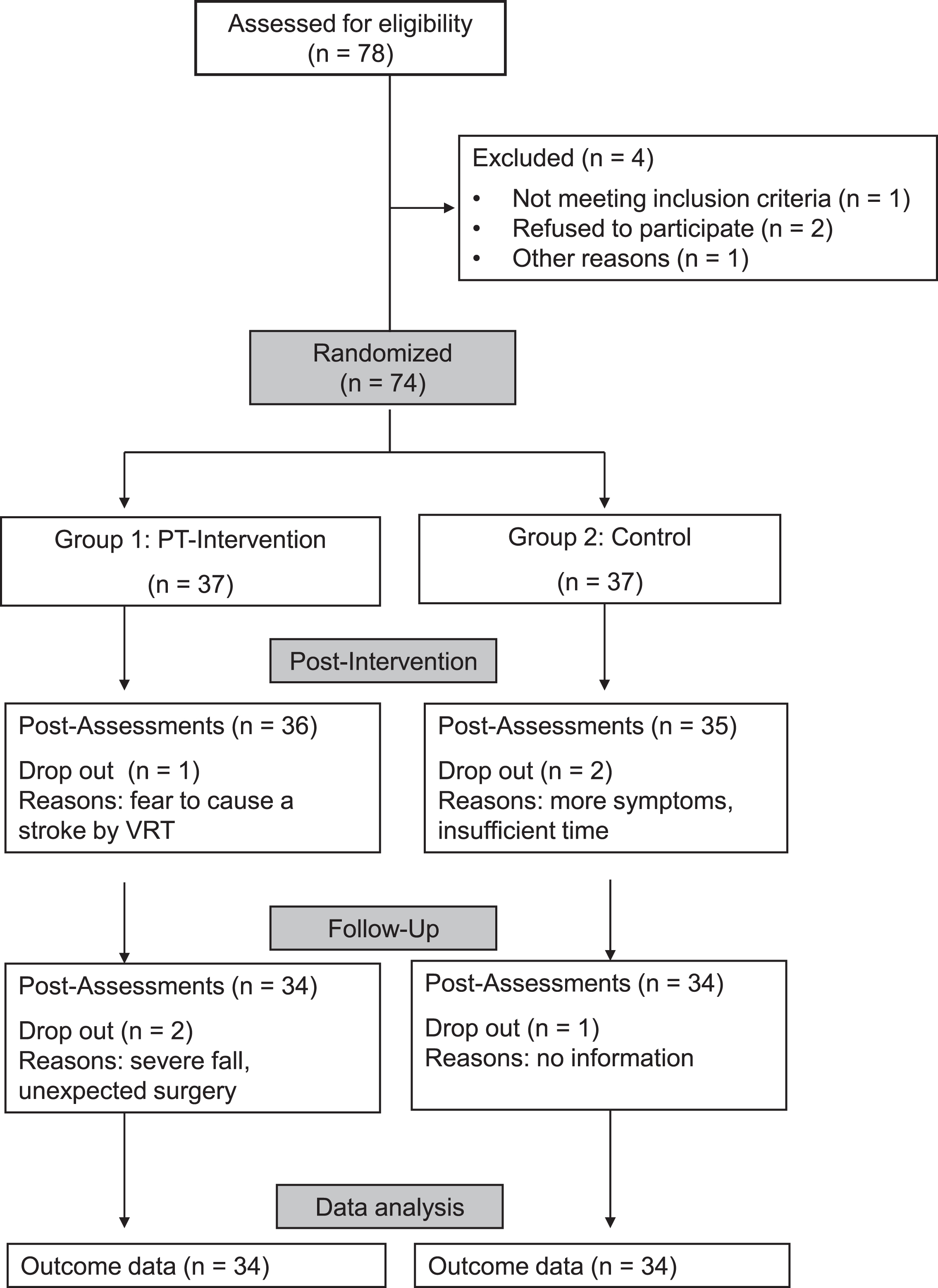
Flow chart of the study.
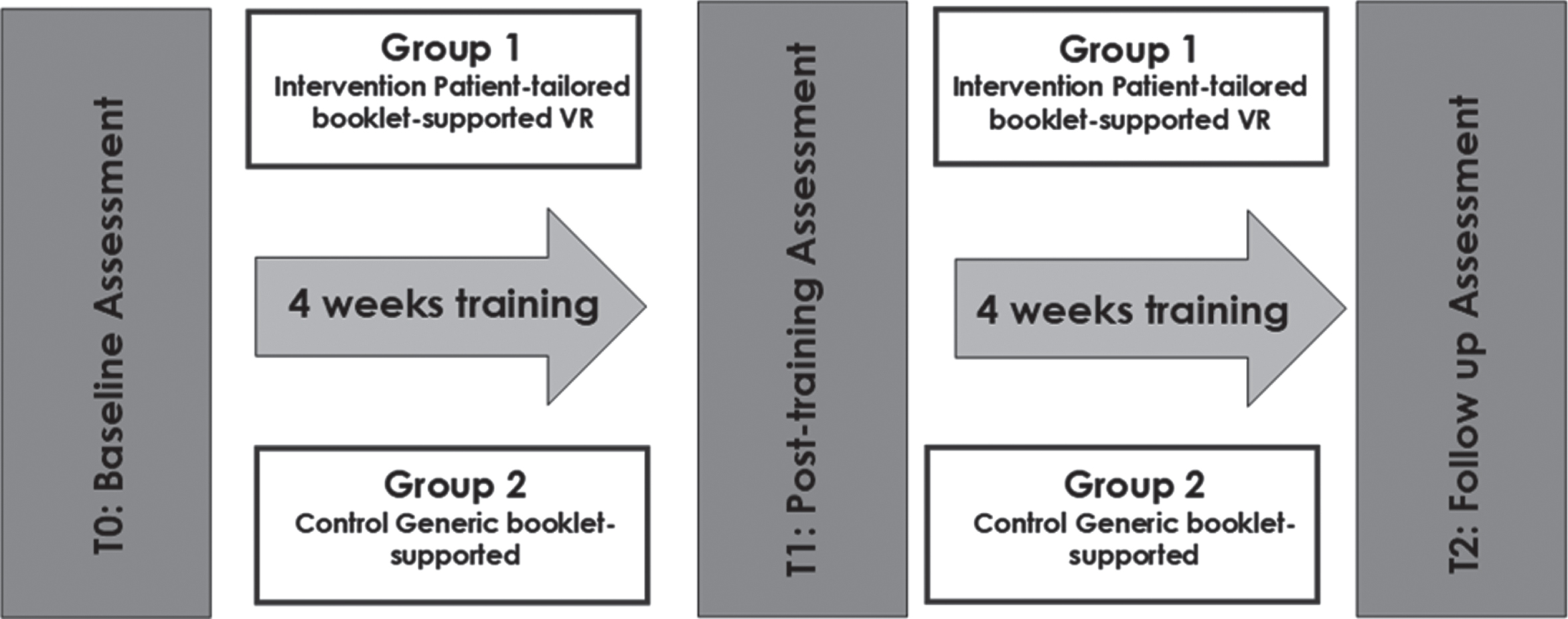
Course of the study.
The study protocol has been approved by the Ethics Committee of the University of Munich (370-15). All procedures were in accordance with the Helsinki declaration and all study participants gave their written signed informed consent. The study was registered with the German Register of Clinical Studies (DRKS ID: DRKS00009016).
Outcome measures
The study participants were assessed with a battery of clinical and objective balance measures, as well as self-assessment instruments. The Dizziness Handicap Inventory (DHI-G) total score was the primary outcome. Secondary outcomes were the Visual Analog Scale for dizziness and balance disorders (VAS), the Activity-specific Balance Confidence scale (ABC-G), the Vestibular Activity and Participation Questionnaire (VAP-G), instrumented static posturography, the Timed-up-and-Go test (TUG), the Falls Efficacy Scale (FES-I), the therapy diary, the Problematic Experiences of Therapy Scale (PETS), and the accuracy scale.
All outcomes were assessed on admission to the study (T0), after four weeks of training (T1) and at follow-up after another four weeks (T2). Assessments were carried out by a blinded medical-technical assistant from the center (DSGZ). The study participants from both groups were recommended to continue exercising after the actual intervention (Fig. 2).
The
The
The
The
The
The
The
The
Intervention
To minimize systematic errors, all study participants were assessed and instructed by the same physiotherapist, an expert in VRT and a specialist therapist for dizziness and balance disorders (SK). The therapist kept the time with the study participants’ constant at 60 minutes in both groups. Study participants in both trial arms received a brochure for VRT at home (see supplementary material). The exercise selection was based on documented evidence for vestibular rehabilitation [11, 15, 29, 47]. The booklet includes 16 illustrated exercises for adaptation, habituation and substitution in vestibular dysfunction. The following eight weeks (intervention and follow-up), all study participants were asked to exercise at home for 20 minutes twice a day using the flyer. In order to monitor the therapy, they kept a standardized diary.
Data analysis
Data were analyzed using SPSS (IBM SPSS Statistics, Version 26). Data are reported as mean±SD. The effects of each dependent variable was analyzed using an analysis of variance for repeated measures (repeated measure ANOVA) with group (intervention vs. control) and time point (T0, T1 and T2) as factors and Bonferroni post hoc analysis. The homogeneity of variance was confirmed using the Levene test (p-value greater than 0.05). The requirement for sphericity was checked using the Mauchly test and, in the case of inhomogeneous factor levels, subjected to the Greenhouse-Geisser correction procedure. The evaluation method for the study was carried out as per protocol analysis. Results were considered significant if p < 0.05.
Results
Participant characteristics
Table 1 shows baseline characteristics of study participants in the two groups. At baseline, the groups were comparable with respect to all assessed characteristics. The majority of study participants were between 60 and 79 years old. Only one study participant required professional assistance. Most study participants were able to perform daily life activities without any support (n = 41) or only required minor support from family and friends (n = 32).
Baseline characteristics of study participants in the intervention and control group
Baseline characteristics of study participants in the intervention and control group
*Medication not only for dizziness.
Severe adverse events of the intervention did not appear (falls, fractures, hospitalizations). Study participants were informed before the start of the intervention that symptoms (dizziness) can worsen during therapy. ANOVA results are summarized in Table 2.
Repeated measures ANOVA results
Repeated measures ANOVA results
Effects of time, group and interaction on outcome measures –significant effects are marked in bold. Abbreviations: DHI-G - Dizziness Handicap Inventory, p - physical, e - emotional, f –functional; TUG - Timed up & go test; ABC-G - Activities-Specific Balance Confidence Scale; FES-I - Falls Efficacy Scale; VAP-G - Vestibular Activities and Participation Measure; PU –Posturography; EO - eyes open; EC - eyes closed; VAS total - Visual-analog scale for dizziness and balance disorders; PETS - Problematic Experiences of Therapy Scale.
At baseline, DHI-G total revealed equal dizziness-related limitations of daily activities in the intervention and control group (p = 0.796). Both groups reported an improved DHI-G total score after 4 weeks of VRT (T1, p < 0.001), and further improvement at follow-up (T2, p < 0.001). Home-based exercises with instructions in the intervention group yielded greater improvements in DHI-G total score at T1 (p = 0.045) and T2 (p = 0.030) compared to controls (Fig. 3A). These general effects were differently manifested at the level of DHI subscores. With respect to DHI-G (p) reflecting physical activity and symptom triggers, both groups showed equal improvements at T1 and T2 (both p < 0.001) (Fig. 3B). With respect to DHI-G (e) and (f) reflecting emotional and functional aspects respectively, both groups showed reduced subscores at T1 and T2 (both p < 0.001), with greater improvement in the intervention group at T2 (DHI-G (e): p = 0.016; DHI-G (f): p = 0.042) (Fig. 3CD).
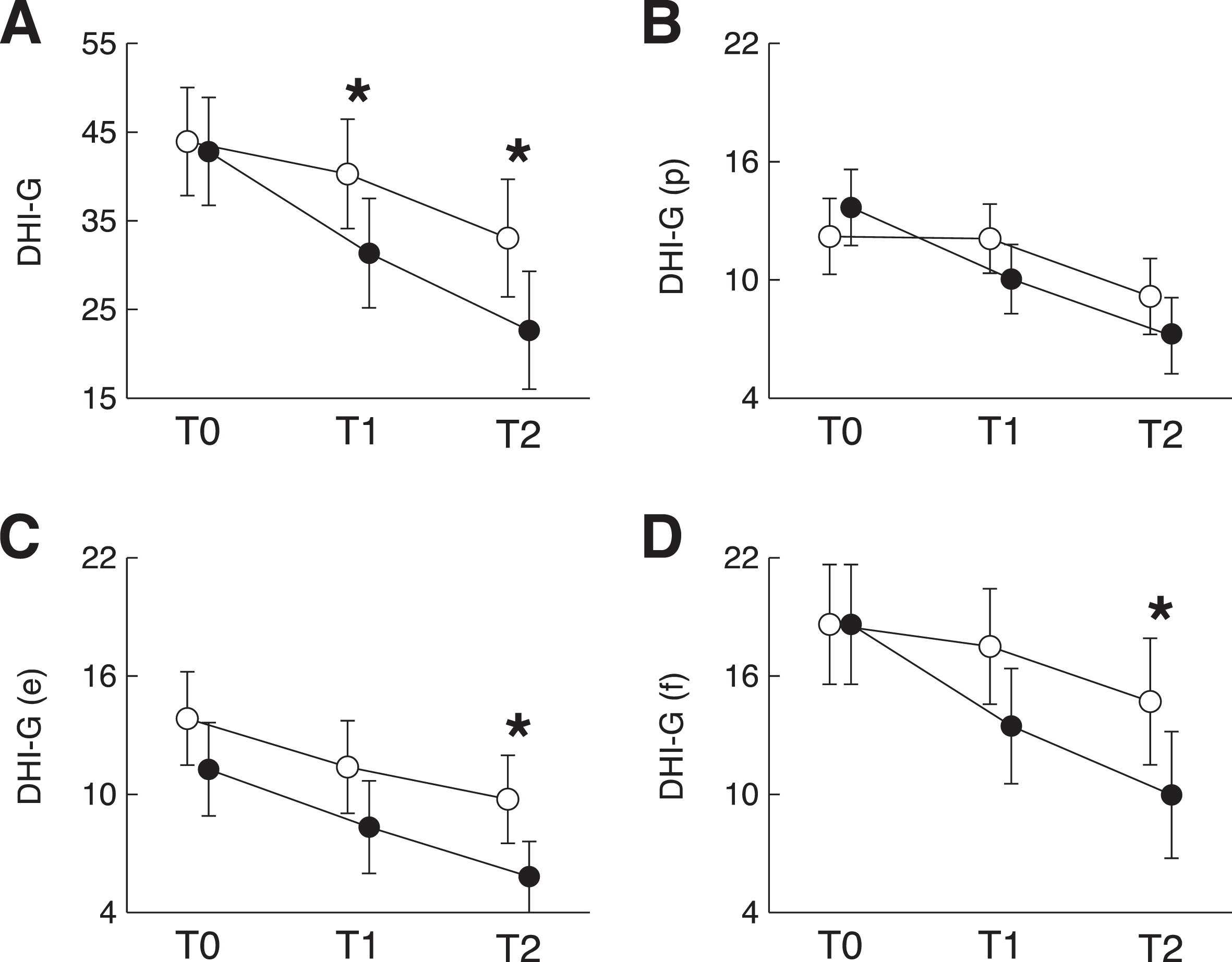
Results for the DHI-G. Mean±SD are shown. A: DHI-G total score; B: DHI-G subscore (p); C: DHI-G subscore (e); D: DHI-G subscore (f). Abbreviations: DHI-G - Dizziness Handicap Inventory, p - physical, e - emotional, f –functional;; T0 –baseline; T1 –after 4 weeks of training; T2 –at follow-up (8 weeks after T0). Significant differences between groups are marked by an asterisk (*).
At baseline, subjectively perceived vertigo as assessed by the VAS was comparable between the intervention and control group (p = 0.082). Both groups reported a reduced intensity of symptoms after 4 weeks of VRT (T1, p < 0.001) and a further improvement at follow-up (T2, p < 0.001). Home-based exercises with instructions in the intervention group yielded greater reductions in VAS at T1 (p = 0.002) and T2 (p < 0.001) (Fig. 4A).
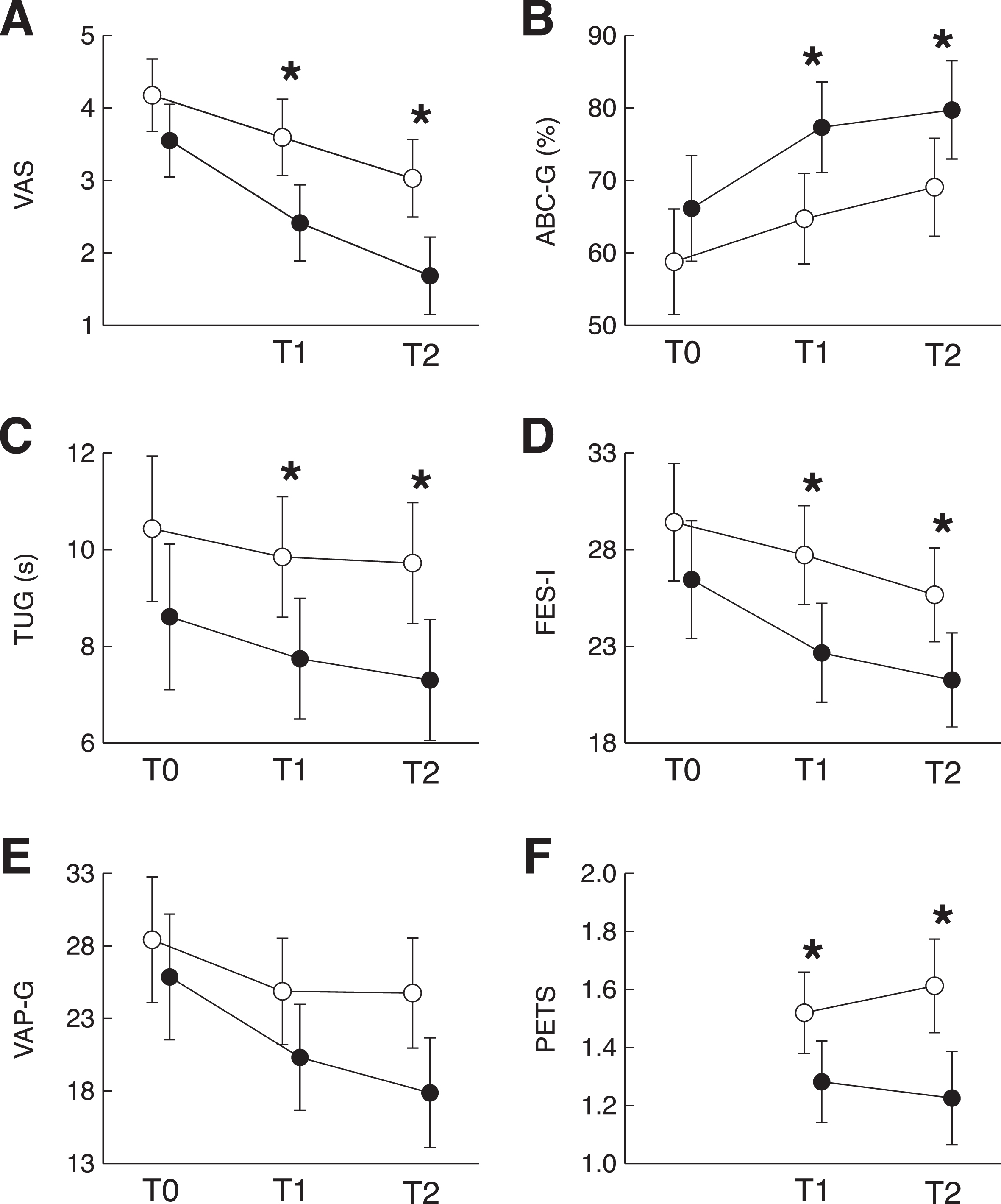
Results for VAS, ABC-G, TUG, FES-I, VAP-G, and PETS. Mean±SD are shown. A: VAS total, B: ABC-G, C: TUG, D: FES-I, E: VAP-G, F: PETS. Abbreviations: ABC-G - Activities-Specific Balance Confidence Scale; FES-I - Falls Efficacy Scale International-G; PETS - Problematic Experiences of Therapy Scale; TUG - Timed up & go test; VAP-G - Vestibular Activity and Participation Questionnaire; VAS: Visual Analog Scale for dizziness and balance disorders; T0 –baseline; T1 –after 4 weeks of training; T2 –at follow-up (8 weeks after T0). Significant differences between groups are marked by an asterisk (*).
Fall-related self-efficacy levels as assessed by the ABC-G were comparable between groups at baseline (p = 0.131). Both groups reported reduced ABC-G at T1 (p < 0.001) and further improvement at follow-up (p < 0.001). The intervention group showed greater reductions in ABC-G at T1 (p = 0.005) and T2 (p = 0.027) (Fig. 4B).
At baseline the TUG performance was comparable between both groups (p = 0.092). Both groups showed improved TUG performance at T1 (p = 0.004) and a further improvement at T2 (p < 0.001). Home exercise with instructions in the intervention group resulted in greater improvements in the TUG performance at T1 (p = 0.020) and T2 (p = 0.008) (Fig. 4C).
At baseline, the FES-I was comparable between both groups (p = 0.173). Intervention and control group reported reduced FES-I T1 (p < 0.001) and a further reduction at follow-up (p < 0.001). This reduction was more pronounced in the intervention group at T1 (p = 0.007) and T2 (p = 0.013) (Fig. 4D).
At baseline, the VAP-G was not different between groups (p = 0.408). Both groups reported a reduced total VAP-G score at T1 (p = 0.001) and further improvement at T2 (p < 0.001). The home exercises resulted in a greater reduction in total VAP-G score at T2 (p = 0.013) in the intervention group (Fig. 4E).
In the PETS, participants documented reasons that hindered them from performing the exercises. In general, participants in the intervention group that were provided with individualized instructions for their home exercises reported less reasons that kept them from performing exercises at T1 (p = 0.001) and T2 (p = 0.020) (Fig. 4F). In the control group, the most prevailing reasons for missing exercises were associated to limited resources of time (Table 3).
Descriptive statistics (mean±SD) of outcome measures at T0, T1, T2
Abbreviations: DHI-G overall - Dizziness Handicap Inventory, p - physical, e - emotional, f –functional; VAS total - Visual-analog scale for dizziness and balance disorders; TUG - Timed up & go test; ABC-G - Activities-Specific Balance Confidence Scale; FES-I - Falls Efficacy Scale; VAP-G - Vestibular Activities and Participation Measure; PU –Posturography; EO - eyes open; EC - eyes closed; PETS - Problematic Experiences of Therapy Scale (total, subscores a, b, c, d).
The instrumented static posturography showed no difference between the intervention and control group in any of the examined stance conditions (Fig. 5).

Results of static posturography (sway path). Mean±SD are shown. A: standing on firm surface with eyes open, B: standing on firm surface with eyes closed, C: standing on foam with eyes open, D: and standing on foam with eyes closed. Abbreviations: T0 –baseline; T1 –after 4 weeks of training; T2 –at follow-up (8 weeks after T0).
The evaluation of the therapy protocols showed a high training compliance in both groups. More than 80% of the study participants performed the exercises daily. In less than 10%, training took place only once a day but was mostly supplemented by additional sports activities. There was no significant difference between the two groups with respect to training intensity.
Compared to controls, individualized instructions for home-based VRT yielded more pronounced training improvements in the primary outcome measures, i.e., DHI-G. Analogous effects were found for the DHI-G subscores (p) and (e) and most secondary outcomes with the exception of the VAP-G and measures of standing balance from posturography.
This study examined the effect of an exercise therapy intervention.
Discussion
This randomized controlled clinical trial demonstrated an additional beneficial effect of specific and individualized instructions by an experienced physiotherapist on a booklet-based home VRT.
Vestibular rehabilitation is an effective treatment
Previous research has proven that vestibular training is in many cases the most effective treatment option for dizzy patients [14]. The evidence for VRT effects is in particular high for patients with peripheral vestibulopathy [24]. Patients with central vestibular disorders also benefit from VRT [9, 40]. However, there is still insufficient evidence to distinguish between different forms of vestibular rehabilitation. Despite the strong evidence for vestibular rehabilitation a large proportion of dizzy patients report difficulty in getting access to VRT programs [30, 44, 50].
VRT as a home exercise program
Advice to do exercises at home is often given. Instructions are provided offline (printed booklet, flyer) or online (app, website) [46, 50, 52]. There is evidence that home exercise programs can improve symptoms in dizzy patients [2, 7, 8, 13, 21, 22, 28, 42, 43, 50, 52]. In our study, both groups of study participants improved after four and after eight weeks of booklet-based home training. This is consistent with previous findings [2, 5, 6, 9]. Home exercise programs in general have a positive effect on patients with chronic dizziness [15, 21, 22, 28, 46, 50, 52]. Self-training at home is also done to compensate for the poor access to hands-on vestibular rehabilitation [5, 30, 49]. However, many patients in home-based programs receive training material without individualized instructions. Corresponding to existing literature our results showed the effectiveness of a booklet-based vestibular training at home in reducing dizziness [45].
Individualized patient-specific instructions
Our study was able to show that specific and individualized physiotherapeutic support is beneficial for the outcome of VRT training at home. There was a significant reduction in dizziness symptoms, demonstrated as an improvement of the DHI-G score. The physiotherapist addressed the specific problems of participants and selected exercises based on standard assessments. Therapy complexity, starting positions, and specific exercises could be tailored to the individual subject. With the precise instructions participants are able to adapt the exercises in intensity, speed, and starting positions by themselves. The findings are consistent with existing literature on tailored VRT [13, 43]. In contrast to van Vugt et al. [46], we were able to show that a specific physiotherapeutic intervention with individualized instructions has a significant additional effect on reducing perceived symptoms and associated limitations. Our results suggest that participants benefit from accurate information. We assume that a tailored adaption of training to the patient’s needs can enhance compensation of the vestibular deficits. Patients guided by specific physiotherapy have a higher chance of reducing their dizziness on the VAS by at least 50%. A decrease of the intensity of dizziness might lead to a reduced use of health system services and thereby contribute to efficient and cost-saving patient care. Thus, we highly emphasize the recommendation of therapy adapted to the individual needs of patients.
Limitations of the study
The study has some limitations. Almost 90% of our cohort suffered from peripheral vestibular disorders, only about 10% (n = 8) had central vestibular syndromes. It is thus not clear if the findings can be generalized to all dizzy patients. Further, our sample from a tertiary dizziness center might not be representative for the situation in the practice of physiotherapists and general practitioners. However, the highly selected chronic patients at our center should be more difficult to treat. Other patients will therefore most likely also benefit from tailored training programs. For safety reasons, we decided not to provide standardized exercises with eyes closed for home use. Although previous work has shown that after vestibular loss, exercises on an unstable surface with and without eyes closed are crucial for compensation [6, 16, 23] we had to minimize the risk of falls in the home setting. Patients were encouraged, however, to do the training at the limit and as difficult as tolerated. The present study used standardized instruments for assessment. In particular the primary outcome measure DHI-G is frequently used in the literature. However, only static but not dynamic balance has been measured. Dynamic conditions are relevant as many patients report on difficulties during walking. However, we believe that the general limitation of the study participants was well covered by the available measures. In analogy to most therapy studies, we were not able to blind the therapist. We, however, do not think that this may have impacted the study outcomes, since all analysis was performed by investigator not involved in the intervention.
Summary
This study shows that an individualized instruction on how to perform training in a home-based vestibular rehabilitation program improves the training outcome compared to uninstructed exercises. A single intervention by an experienced physiotherapists might be sufficient to optimize the efficiency of the home-care program. It is essential that VRT is included in the curriculum for physiotherapist pre- and post-graduate education to ensure availability of the specific knowledge. Further studies on the duration of the training, intensity and frequency of vestibular rehabilitation are necessary in order to contribute effectively and efficiently to rehabilitation. Especially with regard to different disorders and syndromes, it remains necessary to develop specific treatment options.
Footnotes
Author contributions
SK, CS, and KJ conceptualized and designed the study. SK, TA, JD, MW and CS recruited patients, collected and analyzed data. SK made a first draft of the manuscript. SK, KJ and MW prepared the final draft of the manuscript. All authors read and approved the final manuscript.
Funding
The study was supported by the Schön Klinik Bad Aibling SE & Co. KG (staff cost for the Neurorehabilitation Research Platform at the German Center for Vertigo and Balance Disorders of the LMU Munich).
Disclosures
S. Kellerer reports no disclosures.
T. Amberger reports no disclosures.
J. Dlugaiczyk reports no disclosures.
C. Schlick reports no disclosures.
M. Wuehr reports no disclosures.
K. Jahn reports no disclosures.