
Abstract
BACKGROUND:
Cochlear implantation (CI) is associated with changes in the histopathology of the inner ear and impairment of vestibular function.
OBJECTIVE:
The objectives of our study were to evaluate patients for clinical manifestations of space perception and balance changes before surgery, compare them with asymptomatic subjects (controls), and report changes in posturography and subjective visual vertical (SVV) during the acute post-surgery period in patients.
METHODS:
Examination was performed using static posturography and the SVV measurement. We examined 46 control subjects and 39 CI patients. Patients were examined pre-surgery (Pre), 2nd day (D2) and then 14th day (D14) after implantation.
RESULTS:
Baseline SVV was not different between patients and control group. There was a statistically significant difference (p < 0.001) in SVV between subgroups of right- and left-implanted patients at D2 (–1.36±3.02° and 2.71±2.36°, right and left side implanted respectively) but not Pre (0.76±1.07° and 0.31±1.82°) or D14 (0.72±1.83° and 1.29±1.60°). Baseline posturography parameters between patients and control group were statistically significantly different during stance on foam with eyes closed (p < 0.05). There was no statistically significant difference in posturography among Pre, D2 and D14.
CONCLUSIONS:
CI candidates have impaired postural control before surgery. CI surgery influences perception of subjective visual vertical in acute post-surgery period with SVV deviation contralateral to side of cochlear implantation, but not after two weeks.
Introduction
Cochlear implantation (CI) is accepted as an effective rehabilitation method in patients affected by sensorineural hearing loss. Although cochlear implantation is considered to be surgically safe, changes in the histopathology of the inner ear and impairment of vestibular function in the post-surgery period has been reported [14, 30]. Multiple mechanisms that could lead to vestibular dysfunction during or after CI surgery are: direct trauma caused by electrode insertion into the cochlea, endolymphatic hydrops or electrical stimulation of implant itself [17]. Previous studies used questionnaires, testing of vestibulo-ocular reflex and posturography to objectively assess the effects of CI on vestibular function [9, 10]. More recent studies have reported a relatively wide range of findings. Adverse vestibular symptoms have been reported to occur in 0.33% to 75% of patients [28]. Reduction in VOR function has been reported in 23% to 100% of patients [33]. A postoperative risk of developing balance disorders –at least temporarily –has been reported, ranking widely from 0.16% to 75% [15, 29].
Few previous studies have examined posturography and perception of subjective visual vertical (SVV) in relation to CI. Results of some authors reported that comparison of pre-surgery posturography parameters between the CI and control groups were not significantly different [24], but there are papers that documented the opposite finding [8, 18]. However, it was documented that the pre-surgery risk of fall is higher among CI candidates than in healthy population [23]. Significant differences were found in static posturography comparing pre- and one week post-surgery in patients with CIs turned off [11].
Many cochlear implanted patients experienced dizziness in the first weeks following surgery [20, 26]. One possible cause of dizziness can be explained by utricular hyperfunction in the operated ear [31]. The most accurate test of utricular function is the Vestibular Evoked Myogenic Potential (VEMP) [7]. However, VEMP testing is difficult to perform second day after surgery. Thus we chose the SVV, which can be more easily administered to patients in acute stage after surgery. Many patients have deviated SVV at pre-operative and post-operative assessments. Statistically significant changes were not seen when comparing pre-operative and post-operative SVV one week, and one month after surgery [22]. In contrast, a recent study by Truong et al. showed impaired perception of SVV one day after surgery [31].
Studies have been limited by the design, limited follow up, small patient numbers or variable surgical techniques.
The first goal of our study was the assessment of patients for clinical manifestations of space perception (SVV) and balance dysfunction (posturography) before surgery and to compare them with asymptomatic subjects (controls). The second goal of the study was to report changes in posturography and SVV from pre- to the acute post-surgery period.
Methods
Subjects
We tested two groups of subjects, CI patients and controls. The CI group consisted of thirty-nine patients (23 females and 16 males) aged 44.7±13.6 years (mean±SD, range 18.7–72.3 yrs) who underwent unilateral CI for sensorineural hearing loss. The etiology included profound congenital hearing loss with progression (20 patients), idiopathic progressive hearing loss (14 patients), fracture of the temporal bone (2 patient), severe hearing loss after therapy with streptomycin in childhood (1 patient) and meningitis (2 patients). All the patients underwent genetic examination (three patients had connexin 26 mutation). The subjects received a unilateral CI (Cochlear Profile with Slim Perimodiolar electrode –CI532 –25 patients, Cochlear Profile with Contour Advance electrode –CI512 –2 patients, Advance Bionics Ultra with SlimJ electrode –8 patients and Medel Synchrony with Flex28 electrode –4 patients). All patients underwent a standard procedure of cochlear implantation involving cortical mastoidectomy, posterior tympanotomy, and electrode insertion through a round window. The implantation was performed on the right side in 18 patients and on the left side in 21 patients. They had no other neurootologic disorders, and a negative history of major neurologic disorders. The patients did not complain of dizziness or impaired balance function. The clinical neurootologic examination did not reveal a vestibular disorder. Otolith function was preoperatively tested with bone-conducted cVEMP in 15 patients. Absent responses were observed in four patients. In eleven patients responses were present.
All patients underwent surgery at the Department of Otorhinolaryngology –Head and Neck Surgery, University Hospital Motol, 1st Faculty of Medicine, Charles University, Prague.
The control subjects were recruited from employees at the 2nd Faculty of Medicine, Charles University in Prague. The control group consisted of forty-six subjects (29 females and 17 males) aged 44.0±12.3 years (mean±SD, range 19.4–69.7 yrs). All of them were free of known vestibular or other neurological disorders. All subjects gave informed consent before the experiment. The study was performed in accordance with the Helsinki Declaration and the study protocol was approved by the local ethical committee.
Apparatus and testing procedures
All patients and subjects were examined in the period between October 2018 and October 2021. Examinations took place in the Neuro-otology laboratory at the Department of Neurology, University Hospital Motol, 2nd Faculty of Medicine, Charles University, Prague. All subjects were examined by the same experienced physiotherapist using the uniform testing protocol. Patients examinations were performed three times, one day before the surgery (Pre), in the early post-surgery period (2nd post-operative day, D2) and then on the 14th post-operative day (D14). Control subjects were examined only once to compare pre-surgery parameters between groups. Examination in the study protocol consisted of posturography and SVV measurement.
Body sway during static posturography was quantified by displacement of the center of foot pressure (CoP). Subjects stood on a force platform (Kistler, type 9286BA, software MARS, Switzerland), sampling frequency 350 Hz, test duration 30 s. All subjects were tested by the modified Clinical Test for Sensory Integration of Balance consisting of four different conditions of quiet stance: stance on firm surface with eyes open/closed and stance on foam surface with eyes open/closed [27]. The subject’s feet were positioned next to each other splayed at an angle of 30°, arms always in the hanging position. If the feet moved at any time during the test, they were repositioned and the test was repeated. For quantification of body sway we used total CoP sway path (SP) and CoP sway area (SA).
Examination of the SVV was performed using the Synapsys system (Synapsys Subjective Vertical, France) consisting of an LCD screen, special goggles with eye occluders and remote control. During examination subjects sat upright with their hands on the remote control and looked into the screen two meters away. The subjects could not see the rim of the screen and surrounding space. On the screen there was a contrasting, straight line. On each trial the software randomly deviated the line right or left, through a random angle. Then the subject used the remote control to align the line to the vertical position. Each click of the remote control changed the position of the line by one degree. Each subject completed six SVV trials in the static condition. SVV estimated position was calculated as mean deviation of each trial.
Statistical analysis was carried out using Statistica 13.3 (TIBCO Software Inc., USA). Descriptive statistics are provided as mean±SD if normally distributed otherwise median and [interquartile range]. Lognormally distributed parameters provided as backtransformed mean and SD. Normality was visually assessed and confirmed using Shapiro-Wilk’s test. SA and SP were log-transfomed before statistical analysis. Single parameter between group comparison was carried out using t-test for independent samples. Multiple parameter analysis was done using general linear model (repeated measures ANOVA, Fisher post-hoc where applicable). Level of statistical significance was set at p < 0.05.
Results
There were no differences in age and sex between controls and patients pre-operatively. Baseline SVV was not different between patients and control group (0.49±1.50 and 0.42±1.09, respectively). There was a significant difference (p < 0.001) in SVV between subgroups of right- and left-implanted CI at D2 (–1.36±3.02 and 2.71±2.36 respectively) but not Pre (0.76±1.07 and 0.31±1.82) or D14 (0.72±1.83 and 1.29±1.60). For SVV see Figure 1.
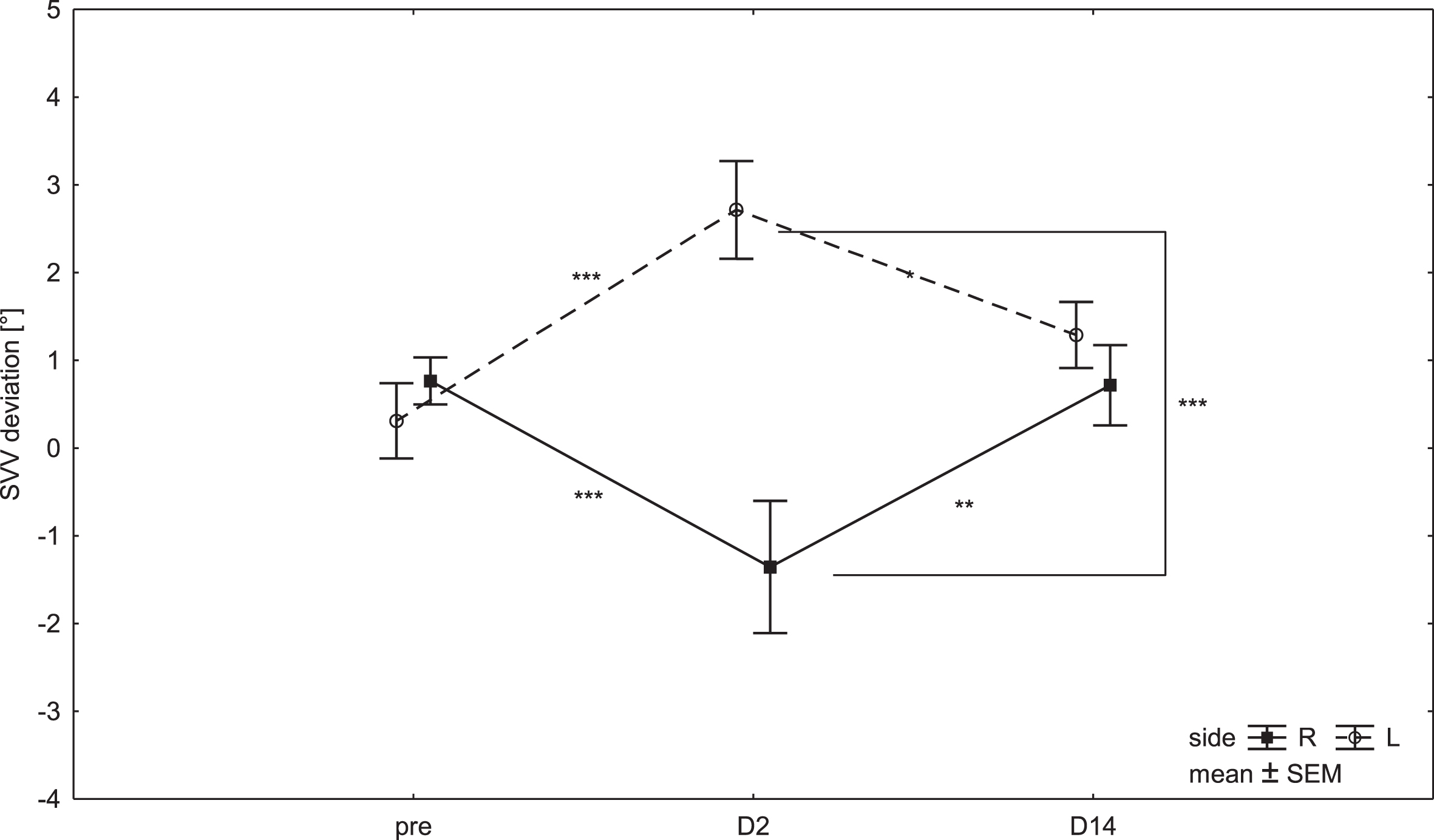
Subjective visual vertical in patients before the surgery (Pre), in 2nd post-operative day (D2) and 14th post-operative day (D14). Dots inside the box represent the mean. Ends of the whiskers represent standard error of the mean (SEM). L –left side surgery (dashed line), R –right side surgery (full line).
Baseline posturography parameters (sway area) between patients and control group were statistically significantly different only on foam surface with eyes closed (p < 0.05). See Figure 2. As expected there was a significant difference between eyes and surface conditions (p < 0.001). There were no statistically significant differences among Pre, D2 and D14 in posturography parameters. See Figure 3.
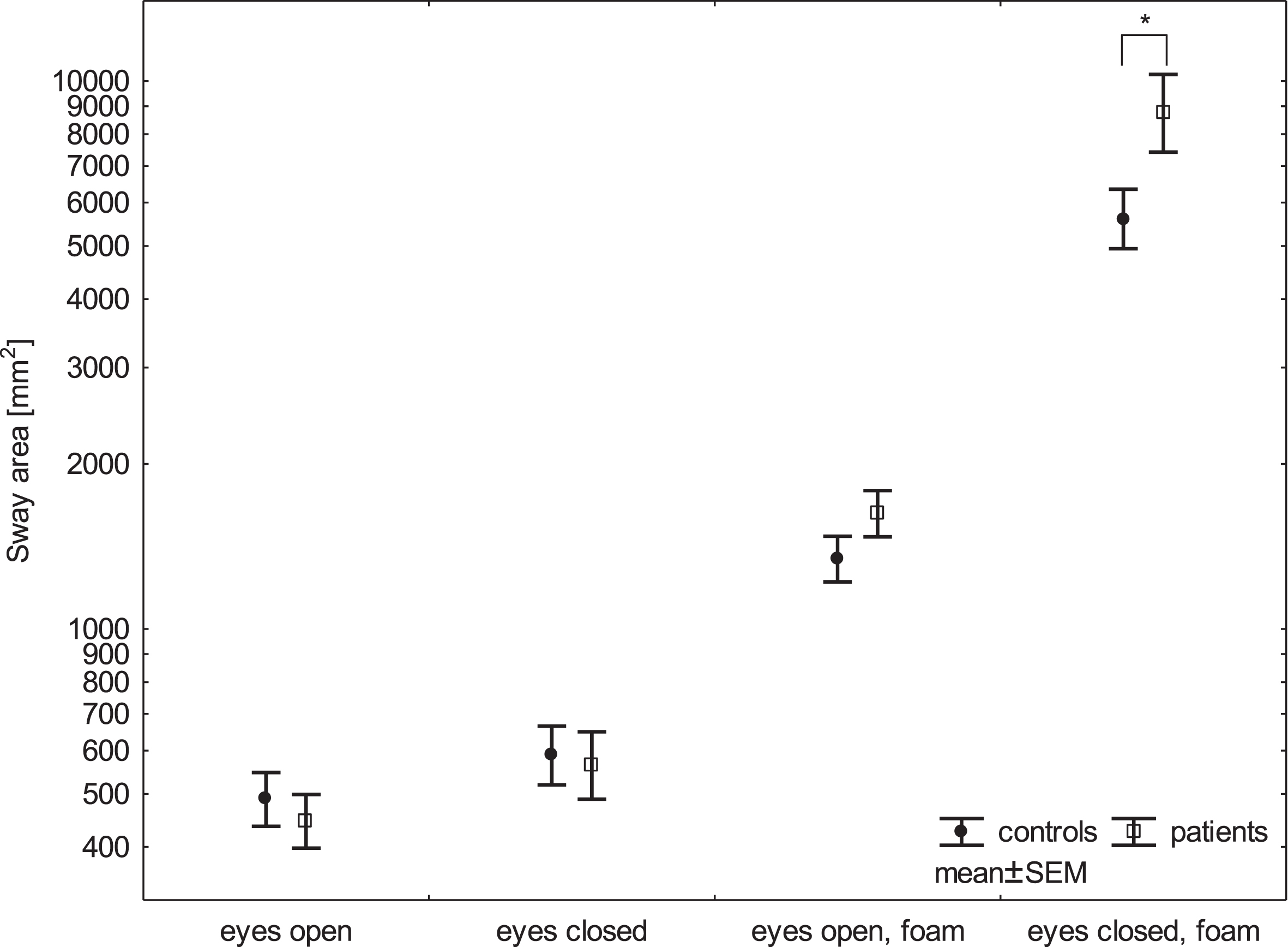
Comparison of posturography parameter sway area between CI patients and controls. Dots inside the box represent the mean. Ends of the whiskers represent standard error of the mean (SEM), log scale.
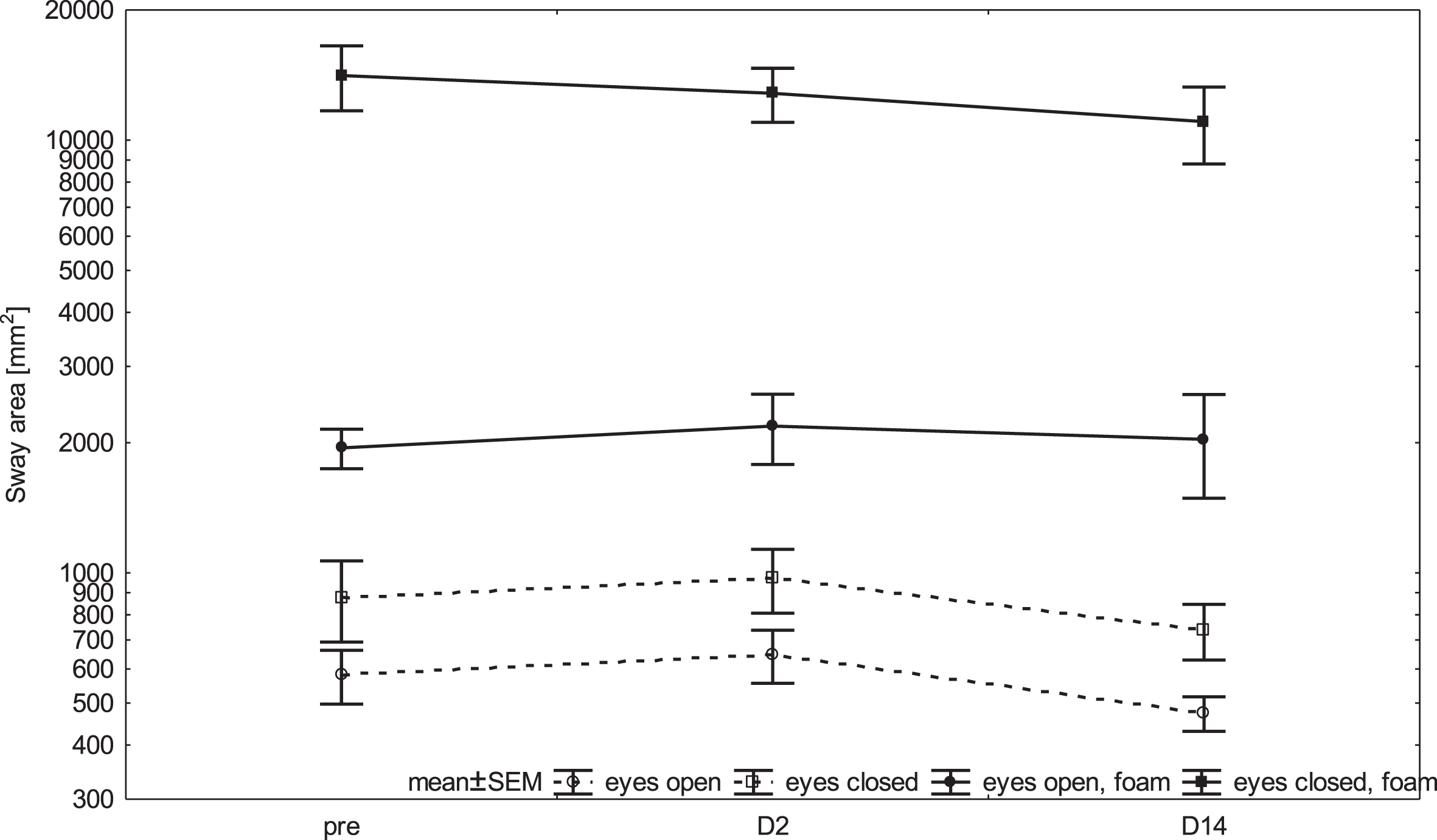
Comparison of posturography parameter sway area before the surgery (Pre), in 2nd post-operative day (D2) and 14th post-operative day (D14). Dots inside the box represent the mean. Ends of the whiskers represent standard error of the mean (SEM), log scale.
In the current study, we focused on differences in perception of SVV and postural control between patients scheduled for CI and controls. The second goal of the study was to describe dynamics of postural control and SVV perception in acute time period around the surgery.
We used SVV as the way to measure verticality perception based on vision by asking subjects to adjust a line along the perceived earth-vertical without using external visual cues.
In upright head orientation healthy human subjects can adjust their SVV to true vertical within a mean error less than two degrees [1, 2]. Tilts of the SVV are a sensitive tool for detecting an imbalance in otolith (utricular) function and are generally accepted as a valid indicator [13]. Utricular hypofunction causes ocular torsion away from the side of the lesion and, consequently, deviation of SVV towards the side of the lesion and conversely utricular hyperfunction (stimulation) causes the opposite ocular torsion [6]. Ocular position is a major determinant of the perceived orientation of visual stimuli [13].
Posturography assesses the integrative vestibular performance associated with the maintenance of posture, which involves integration between the vestibular system and other sensory inputs, such as vision and proprioception. However, there is some redundancy across sensory system, particularly during static balance.
The main finding is that CI patients did differ before surgery significantly from the control group in posturography only in condition stance on foam surface with eyes closed. Our results correspond with other authors, who described similar differences in postural control using Sensory Organization Test or modified Clinical Test for Sensory Integration of Balance [18, 24]. Deaf patients who are candidates for cochlear implantation have normal or decreased vestibular function. This dysfunction in some patients is related to more than one pathology of the labyrinth, which can result in altered balance performance [19]. Second explanation could be that hearing loss of CI candidates consumes cognitive resources, which could thereby limit the resources available to support balance [25]. Subjects with uncorrected hearing loss (pre-CI surgery) have decreased balance performance compared with normal hearing controls [24].
We did not detect a worsening in posturography parameters after CI surgery. In literature were described contradictory results, some authors found significant worsening in posturography after CI surgery [11]. But results of another study indicate that patients undergoing unilateral CI experience some substantial improvements in objective measures of balance function after CI surgery and device activation [5]. The mechanism underlying the findings is that electrical stimulation could provide inputs to the vestibular system and thus improving balance in some way. Our results were similar to Brey et al. who described non- significant difference between pre- and post- implantation [4].
The second important finding was a significant difference SVV between subgroups of right and left implanted CI in D2 (right and left side implanted) but not Pre and D14. This finding means that immediately after surgery there is disturbance in vestibular function. Post-surgery vestibular disorders are widely reported in cochlear implant recipients. Gnanasegram at al. described asymmetric spatial orientation deficits in nearly half of the children participants with cochlear implant [12]. Different etiologies are postulated for these postoperative symptoms of dizziness [21]. Van den Broek et al. describe disruption of endolymphatic flow caused by the electrode itself, which could lead to an endolymphatic hydrops similar to Ménière‘s disease [32]. A mechanical irritation of the membranous labyrinth, or the labyrinthitis triggered by a foreign body in the cochlea, could also cause vestibular disorders in patients with cochlear implants [4]. Histopathologic changes are frequently found in the saccule and utricle but are less frequently found in the semicircular canals following CI [30]. These histopathologic changes may correlate with functional impairment of the otolithic organs. SVV testing operates on the principle that unilateral utricular hypofunction causes ocular torsion away from the side of the lesion and, consequently, deviation of SVV towards the side of the lesion [3].
In our patients pre-operative SVV testing was within physiological limits and they did not differ from control subjects. Although some studies show that up to 40% of the patients exhibited abnormal SVV of pre-operative patients [22]. In the immediate post-operative period patients exhibited abnormal SVV than at pre-operative assessment. Assessment two weeks post-operatively demonstrated that deviation of SVV returned to normal range. Our data showed that immediately after surgery there is functional disturbance of utricular function. SVV measurements suggest that CI causes utricular hyperfunction in the implanted ear. The recent study by Imai et al. found that utricular function is deteriorated after CI in contrast to saccular function. Their explanation has two parts: 1) insertion of the electrode caused perilymphatic fistula and presence of air in the vestibule, and 2) air is collected in the utricle because is anatomically higher than the saccule and may cause this dysfunction [16]. The return of SVV values to pre-surgery levels in first two weeks could be explained by tissue recovery and resolution of edema after implantation and central compensation.
In conclusion the use of a test sequence of posturography to analyze balance function showed that static postural control was already impaired before surgery and there is a significant difference CI and control groups. Patients’ parameters did not change among pre-surgery, immediate post-surgery and two week period. In SVV we did not observe a difference between controls and patients before surgery but found a significant difference in SVV between subgroups of right- and left-implanted CI in D2 but not Pre and D14. This finding means that immediately after surgery there is disturbance in utricular function.
Footnotes
Acknowledgments
This work was supported by the Cooperatio Program (research area Sport Sciences –Biomedical & Rehabilitatioan Medicine and research area Surgical discipline) and by Ministry of Health of the Czech Republic (grant NV19-06-00189). The authors would like to greatly acknowledge Helen S. Cohen, EdD, Baylor College of Medicine, TX, USA, for her language corrections, technical assistance and helpful comments.